1391
Field Strength and Gadolinium Dose Dependency of Dynamic Time-Resolved 4D MRA of the Brain Using Golden-Angle Radial Sparse Parallel (GRASP) MRI1Department of Radiology, Children's Healthcare of Atlanta, Atlata, GA, United States, 2Department of Radiology and Imaging Sciences, Emory University, Atlanta, GA, United States, 3Department of Radiology, New York University Langone Medical Center, New York, NY, United States, 4Department of Radiology, Maimonides Medical Center, Brooklyn, NY, United States, 5Department of Radiology, Weill Cornell Medical Center, New York, NY, United States, 6Department of Neurology, New York University Langone Medical Center, New York, NY, United States
Synopsis
GRASP MRI obtained as part of routine clinical care, without specific angiographic parameters, can be reconstructed post-hoc into dynamic 4D MR images and can be displayed with high spatial and temporal resolution. Additionally, contrast dose and magnet strength appear to have minimal effect on the diagnostic quality of angiographic images. Further exploration into diagnostic accuracy and the tolerance of varying field strength and dosing to further increasing degrees of acceleration is warranted.
Introduction:
GRASP, a fast and flexible MRI technique that combines compressed sensing, parallel imaging, and golden-angle radial sampling, is acquired continuously and can be retrospectively reconstructed using user-defined parameters optimized for application-specific uses.1 We have explored GRASP methodology using a custom reconstruction and visualization pipeline to produce MR angiography from anatomic brain imaging obtained in routine practice. Herein, we systematically analyzed the effects of magnet field strength and contrast dose on the performance of 4D GRASP MRA in a two-rater study of angiographic quality and accuracy.Methods:
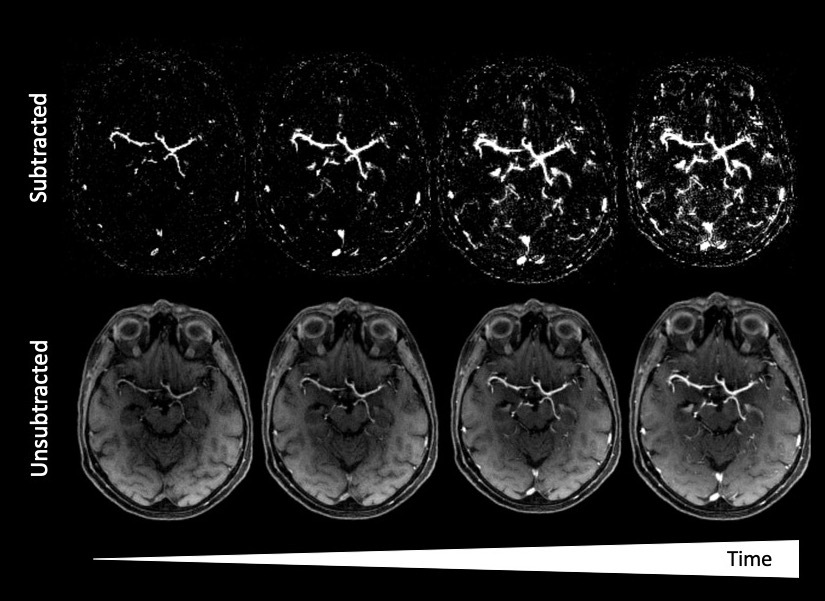
Axially-acquired GRASP scans obtained during the course of routine clinical care at 1.5 (Avanto/Aera, Siemens Healthcare, Germany) and 3T (MAGNETOM Skyra/Prisma, Siemens Healthcare, Germany). A weight-based gadolinium dosing regime was employed in all subjects using a high-relaxivity agent (Gadavist) that was injected 20sec after the start of the GRASP acquisition, some scans with full and some with half dose administration per clinical protocol. Images were reconstructed by combining 3 consecutive radial views into one frame, resulting in a time resolution of ~900ms/frame and spatial resolution of approximately 1.0mm3. Images were reconstructed using SyngoVia software (Siemens Healthcare, Germany). Images were scored by two neuroradiologists, blinded with respect to scanner strength and contrast dose, for image quality, dynamic imaging capabilities, and apparent imaging and angiographic reconstruction artifacts. Peak arterial and venous enhancement phases were identified and subsequently scored qualitatively using a 4-point Likert scale (0 severely limited, nondiagnostic examination; 1 fair, diagnosis possible but limited; 2 good, diagnosis readily possible; and 3 excellent diagnostic quality), with attention to 6 vascular segments: 1) intracranial ICA; 2) MCA M1; 3) MCA M2; 4) MCA M3; 4) MCA M4; 5) deep cerebral veins; and 6) dural venous sinuses. Raw images and subtracted angiography were made available to readers (Figure 1). Differences in median Likert scales were compared using the Mann-Whitney U-test or Wilcoxon signed rank test, when appropriate.Results:
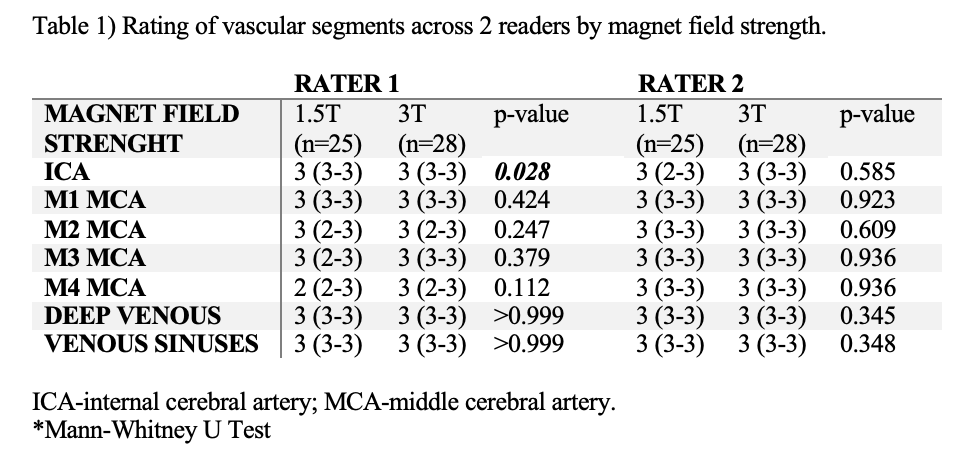
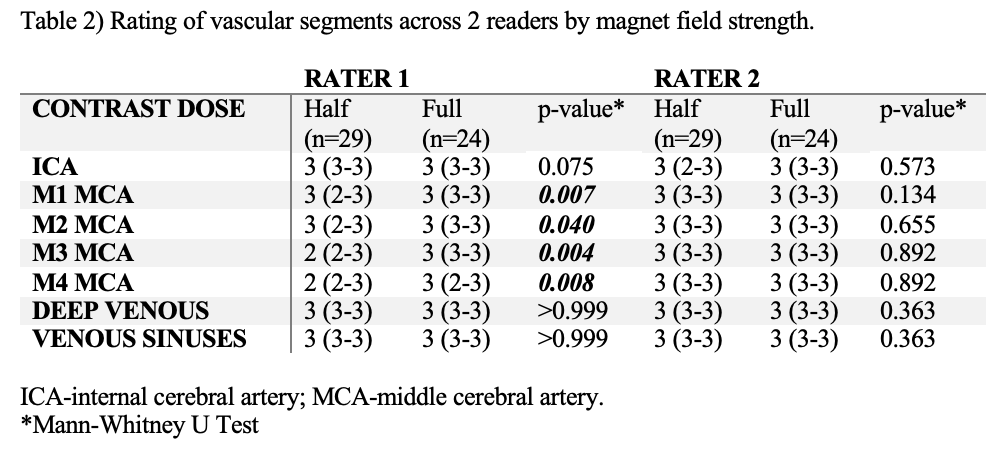
Fifty-three examinations were reviewed (72% female, median age 60 (IQR46-70): 25 cases were acquired at 1.5T and 28 at 3T, with 29 at half and 24 at full dose gadolinium. Comparing 1.5T with 3T, Rater 1 found 3 distinct angiographic frames at 1.5T (IQR3-4) and 5 frames at 3T (IQR4-6), p<0.001, while Rater 2 found 3 frames (IQR 2-3) and 4 frames (3-4), respectively, p<0.001. Likert scores for vascular diagnostic quality across vascular segments overall did not vary by magnet strength (Table 1), with median values of ‘excellent diagnostic quality’ for nearly all vascular segments. Comparing scans with half and full gadolinium contrast dose, Rater 1 found 4 distinct angiographic frames at half dose (IQR3-5) and 4 frames at full dose (IQR3-5), p=0.355, while Rater 2 found 3 frames (IQR 3-4) and 3 frames (3-4), respectively, p=0.977. Likert scores for diagnostic quality across vascular segments were overall lower for half-dose scans for Rater 1 compared with full dose (Table 2), although with medians in the “good” to “excellent” range, and not significantly different for Rater 2, with medians of “excellent”. Overall, there were few artifacts identified, with only 2 cases described as limiting diagnostic quality.Discussion:
Using a highly flexible plug-and-play reconstruction and visualization pipeline, 4D MRA using GRASP exhibits excellent performance and high reader confidence in dynamic angiography. The angiographic quality of GRASP reconstructions appears to be at most minimally effected by contrast dose and magnet strength. Several attributes make GRASP uniquely optimized for dynamic angiography. GRASP is acquired as a continuous radial stack-of-stars acquisition of k-space, which allows scans to not depend on exact timing of the data acquisition, significantly simplifying the examination in routine clinical practice. An arbitrary number of consecutive radial views can therefore be combined into a single image frame to create angiographic imaging of any desired temporal resolution. An additional advantage to radial k-space sampling is its reduced sensitivity to motion artifacts.2 Additionally, GRASP simultaneously provides anatomical T1-weighted images with high spatial resolution as well as dynamic angiographic images of the entire imaging volume. These factors make GRASP an intriguing and attractive approach for dynamic MRA.Conclusion:
4D MRA reconstructed post-hoc from GRASP MRI, obtained as part of routine clinical care without specific angiographic parameters, can be displayed with high spatial and temporal resolution. Additionally, contrast dose and magnet field strength appear to have minimal effect on the diagnostic quality of angiographic images. Further exploration into diagnostic accuracy and the tolerance of varying field strength and dosing to further increasing degrees of acceleration is warranted.Acknowledgements
No acknowledgement found.References
1. Feng L, Grimm R, Block KT, et al. Golden-angle radial sparse parallel MRI: combination of compressed sensing, parallel imaging, and golden-angle radial sampling for fast and flexible dynamic volumetric MRI. Magn Reson Med 2014;72:707-717
2. Chandarana H, Feng L, Block TK, et al. Free-breathing contrast-enhanced multiphase MRI of the liver using a combination of compressed sensing, parallel imaging, and golden-angle radial sampling. Invest Radiol 2013;48:10-16
Figures