1380
Quantitative Evaluation of Normal Lumbosacral Plexus Nerve Using Diffusion Tensor Imaging with Multiband SENSE
Nan Zhang1, Caizhong Chen1, and Qingwei Song2
1Department of Radiology, Zhongshan Hospital affiliated to Fudan University, Shanghai, China, 2Department of Radiology, The First affiliated hospital of Dalian Medical University, Dalian, China
1Department of Radiology, Zhongshan Hospital affiliated to Fudan University, Shanghai, China, 2Department of Radiology, The First affiliated hospital of Dalian Medical University, Dalian, China
Synopsis
DTI can provide valuable structural information that may become an innovative tool in evaluating lumbosacral plexus nerve entrapment. Multiband SENSE technique could be used to accelerate the image acquisition .The present study aims to explore the feasibility of DTI with multiband SENSE on normal lumbosacral plexus nerve. The study showed that MB SENSE=2 was recommended for DTI on normal lumbosacral plexus nerve, which facilitated a 32% shorter image acquisition time than conventional SENSE accelerated diffusion tensor imaging.
Synopsis
DTI can provide valuable structural information that may become an innovative tool in evaluating lumbosacral plexus nerve entrapment. Multiband SENSE technique could be used to accelerate the image acquisition .The present study aims to explore the feasibility of DTI with multiband SENSE on normal lumbosacral plexus nerve. The study showed that MB SENSE=2 was recommended for DTI on normal lumbosacral plexus nerve, which facilitated a xx% shorter image acquisition time than conventional SENSE accelerated diffusion tensor imaging.Introduction
DTI can provide valuable structural information that may become an innovative tool in evaluating lumbosacral plexus nerve entrapment. However, the use of DTI to investigate peripheral nervous tissue has not been widely adopted because of the relatively small sample size, the image quality which is easily affected by the movement of abdominal organs and the long scan time4. Multiband SENSE technique, in which multiple slices are acquired simultaneously, allows substantial reduction in scan time while maintaining sufficient anatomical coverage.1-3 The aim of this prospective study was to investigate the feasibility of DTI measurements with MB SENSE on the lumbosacral plexus nerve in healthy volunteers.Methods
A total of 25 healthy volunteers (33.42±16.51 years, range:11-70 years, 10 males)underwent DTI scanning with Multiband SENSE on a 3T whole‐body human scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands) by using a 16 coil. DTI was performed using an echo-planar imaging sequence with the following imaging parameters: TR/TE= 2900/64 msec, FOV 288 × 288 mm2, slice thickness 3 mm, overlap 0mm, b-value 0 and 800s/mm2, number of directions of motion-probing gradients 15, flip angle 90o, number of slices 55, image matrix 96 ×66. The acceleration factor was set 1.6 for in-plane SENSE, 2 / 3 for Multiband SENS, resulting in an acquisition time of 7 min 55 sec, 3 min 57sec and 1 mi 57sec, respectively. Mean FA values of the lumbosacral plexus nerves (both sides of lumbar roots L3 to S1) were quantified.Differences among various segments of lumbar nerve roots were compared with Kruskal-Wallis test. FA values of different lumbosacral plexus nerve in SENSE 1.6 、MB SENSE 2 and MB SENSE 3 were compared with independent samples Kruskal-Wallis test. The whole length of the lumbar roots nerve from L3 to S1 can be visualized clearly by using diffusion tensor tractography (DTT) .Results
Differences of FA values were not found between the right and left side nerves at the same lumbar segment (P>0.05). There was no statistically significant difference in FA values of different lumbosacral plexus nerve using SENSE1.6 、MB SENSE2 and MB SENSE3(Table1). The whole length of the lumbar roots nerve from L3 to S1 based on SENSE 1.6 and MB SENSE 2 can be visualized clearly by using DTT, the distal end of the nerve tract based on MB SENSE3 was poor(Figure1). Scan time was reduced by 50% using MB = 2 compared with conventional.Discussion and Conclusion
The lumbosacral plexus nerve DTI is technically subject to the following factors: magnetic sensitive artifacts caused by the adjacent vertebral body and pelvis in the nerve course area, artifacts caused by abdominal organ movement and cerebrospinal fluid and chemical displacement artifacts, and relatively small lumbosacral nerve root diameter .According to this study, diffusion tensor imaging based on multiband SENSE can show and provide quantitative information of human lumbosaeral plexus nerves. This study indicated that MB SENSE=2 was recommended for DTI on normal lumbosacral plexus nerve, which facilitated a 50% reduction in scan time than conventional SENSE accelerated DTI.Acknowledgements
No acknowledgement found.References
[1] Feinberg DA, Setsompop K. Ultra-fast MRI of the human brain with simultaneous multislice imaging. J Magn Reson 2013;229:90-100. [2] Chen L, T Vu A, Xu J, Moeller S, Ugurbil K, Yacoub E, et al. Evaluation of highly accelerated simultaneous multi-slice EPI for fMRI. Neuroimage 2015;104:452-9. [3] Moeller S, Yacoub E, Olman CA, Auerbach E, Strupp J, Harel N, et al. Multiband multislice GE-EPI at 7 tesla, with 16-fold acceleration using partial parallel imaging with application to high spatial and temporal whole-brain fMRI. Magn Reson Med 2010;63:1144-53 [4] guchi Y,Ohtori S,Orita S,et a1.Quantitative evaluation and visualization of lumbar foraminal nerve root entrapment by using diffusion tensor imaging:preliminary results[J].AJNR Am JNeuroradiol,2011,32:1824—1829.Figures
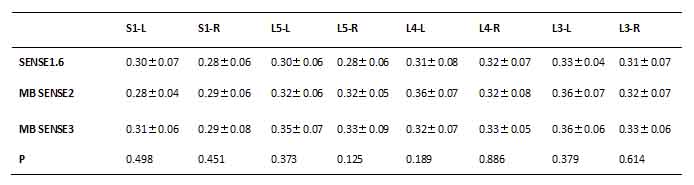
Table1 12
subjects had left and right nerve roots at each segment of L3 to S1 Comparison
of lateral and medial FA values between vertebrae x±s)based
on SENSEN1.6、MB SENSE2 and MB
SENSE3
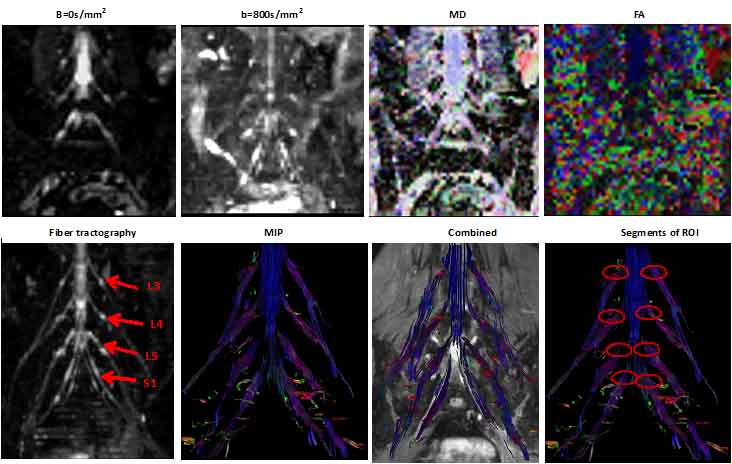
Figure1
Upper
row:b=0s/mm2,b=800s/mm2,mean diffusivity(MD),and fraction
anisotropy(FA)map.Bottom row:Fiber tractography(FT)results of the iumbosacral
nerves,a maximal intensity projection(MIP),FT and T2WI FFE combined,and disply
of the segments at each level region of interest(ROI) placement.Dates obained
by using diffusion tensor imaging based on SENSE1.6.
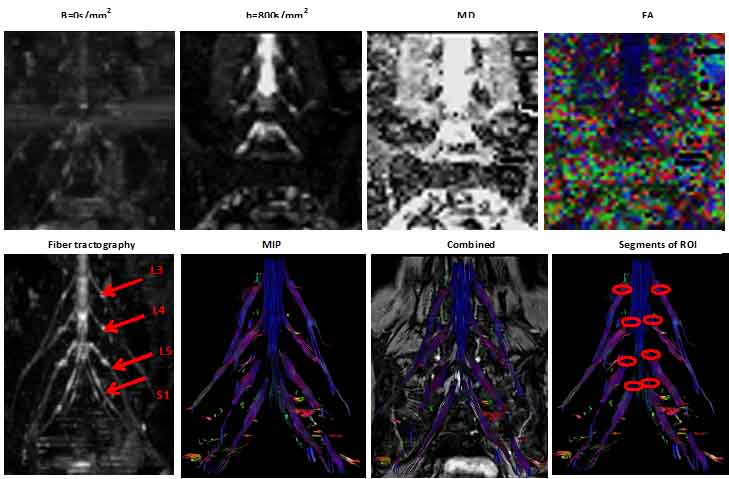
Figure2
Upper
row:b=0s/mm2,b=800s/mm2,mean diffusivity(MD),and fraction
anisotropy(FA)map.Bottom row:Fiber tractography(FT)results of the iumbosacral
nerves,a maximal intensity projection(MIP),FT and T2WI FFE combined,and disply of
the segments at each level region of interest(ROI) placement.Dates obained by
using diffusion tensor imaging based on mutiband SENSE 2.
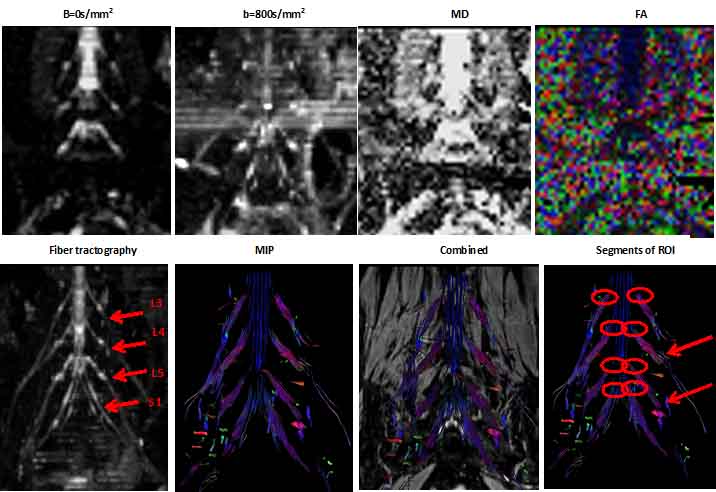
Figure3
Upper
row:b=0s/mm2,b=800s/mm2,mean diffusivity(MD),and fraction anisotropy(FA)map.Bottom
row:Fiber tractography(FT)results of the iumbosacral nerves,a maximal intensity
projection(MIP),FT and T2WI FFE combined,and disply of the segments at each
level region of interest(ROI) placement.Dates obained by using diffusion tensor
imaging based on mutiband SENSE3.The distal end of the L5 and L4 nerve fibers
shown by the arrow is not well displayed.
DOI: https://doi.org/10.58530/2022/1380