1313
Dual-venc Dual-echo (DVDE) Phase-contrast MRI for Simultaneous Measurement of Arterial and Venous Blood Flow1Philips Healthcare, Gainsville, FL, United States, 2Philips Healthcare, Best, Netherlands, 3Boston Children’s Hospital and Harvard Medical School, Boston, MA, United States, 4Children's Hospital Colorado and University of Colorado, Aurora, CO, United States
Synopsis
Phase-contrast (PC) MRI enables non-invasive quantification of blood velocity and flow. The velocity encoding factor (venc) selected by the operator is chosen to maximize the velocity-to-noise ratio (VNR) while preventing aliasing artifacts. To minimize the acquisition time increase associated with an additional venc, a dual-venc dual-echo (DVDE) technique has been proposed where both venc images are acquired within a single TR as dual-echo images. Compared to the single-venc PC-MRI, DVDE allows simultaneous imaging of arterial and venous blood flow with an enhanced VNR and similar blood flow and velocity.
Background
Phase-contrast (PC) MRI enables non-invasive quantification of blood velocity and flow [1]. The velocity encoding factor (venc) selected by the operator is chosen to maximize the velocity-to-noise ratio (VNR) while preventing aliasing artifacts. Multi-venc approaches have been proposed to improve the VNR without velocity aliasing artifacts but this leads to increased scan time for the additional venc acquisitions. To minimize the acquisition time increase associated with an additional venc, a dual-venc dual-echo (DVDE) technique has been proposed where both venc images are acquired within a single TR as dual-echo images [2, 3]. In this work, we sought to compare DVDE to conventional single-venc PC-MRI.Methods
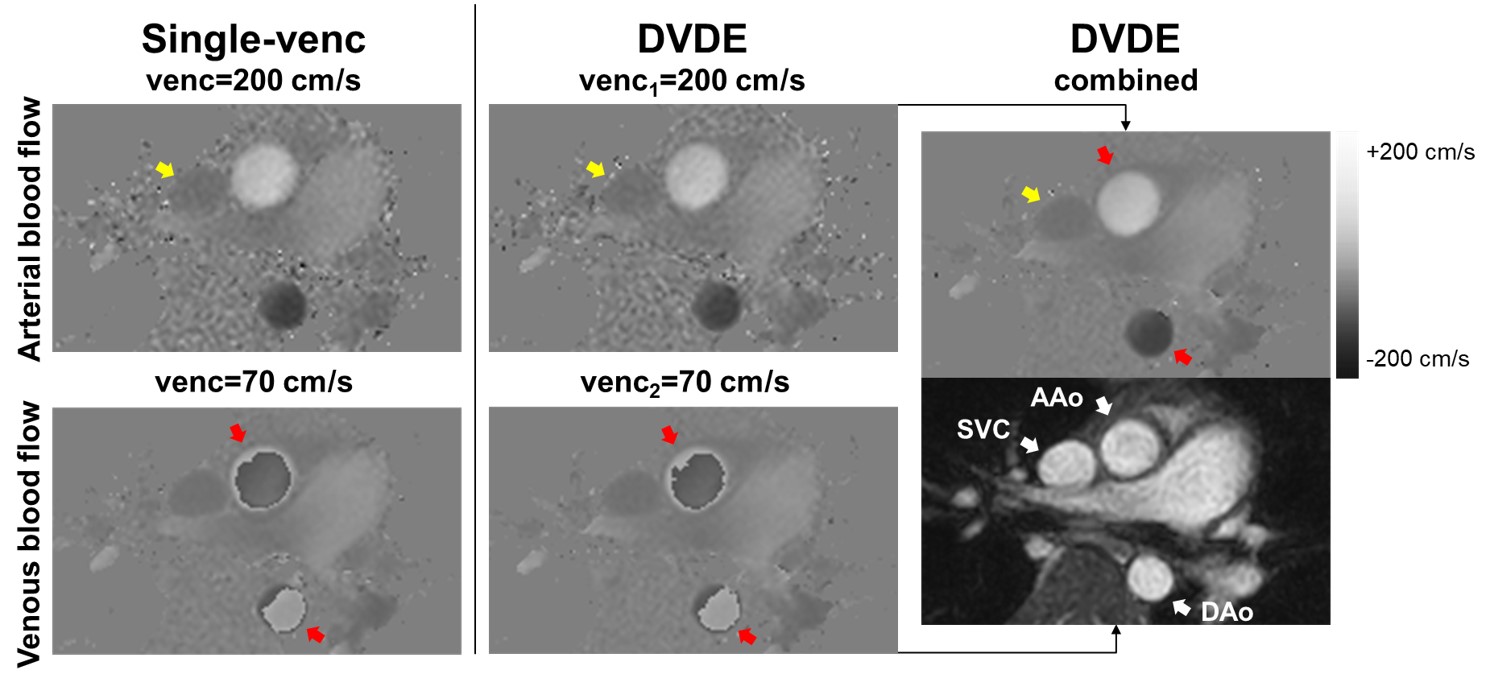
Fifteen patients referred for clinical cardiovascular MRI exams (6 female, median age 16 (1-40) years old) were imaged on Philips Ingenia 1.5 T scanner. An axial imaging plane was prescribed that included the ascending and descending aorta (AAo and DAo) (fast arterial flow) and the superior vena cava (SVC) (slow venous flow) in cross-section. Using this imaging plane, 3 PC images with through-plane velocity encoding were consecutively acquired: 1) a conventional single-venc acquisition using a high venc (200-300 cm/s), 2) a conventional single-venc acquisition using a low venc (70-100 cm/s), and 3) a DVDE acquisition using both a high and a low venc (venc1 = 200-300 cm/s and venc2 = 70-100 cm/s). DVDE single-echo images were generated from the high- and low-venc data separately, and DVDE combined images were generated by performing phase unwrapping of the low-venc images using the high-venc images as the unwrapping threshold. Typical imaging parameters were as follows: spatial resolution 1.5×1.5 mm, slice thickness 6 mm, field-of-view 250×208 mm, flip-angle 12°, acquired heart-phases 20 reconstructed to 30, SENSE 2, and number of signals averages 3. All image reconstruction was performed inline on the scanner. Mean blood flow, maximum mean velocity, and VNR of the DVDE single-echo and DVDE combined data were statistically compared with the single-venc data using the intraclass correlation coefficient (ICC) and a Wilcoxon signed-rank test. P <0.05 was considered statistically significant.Results
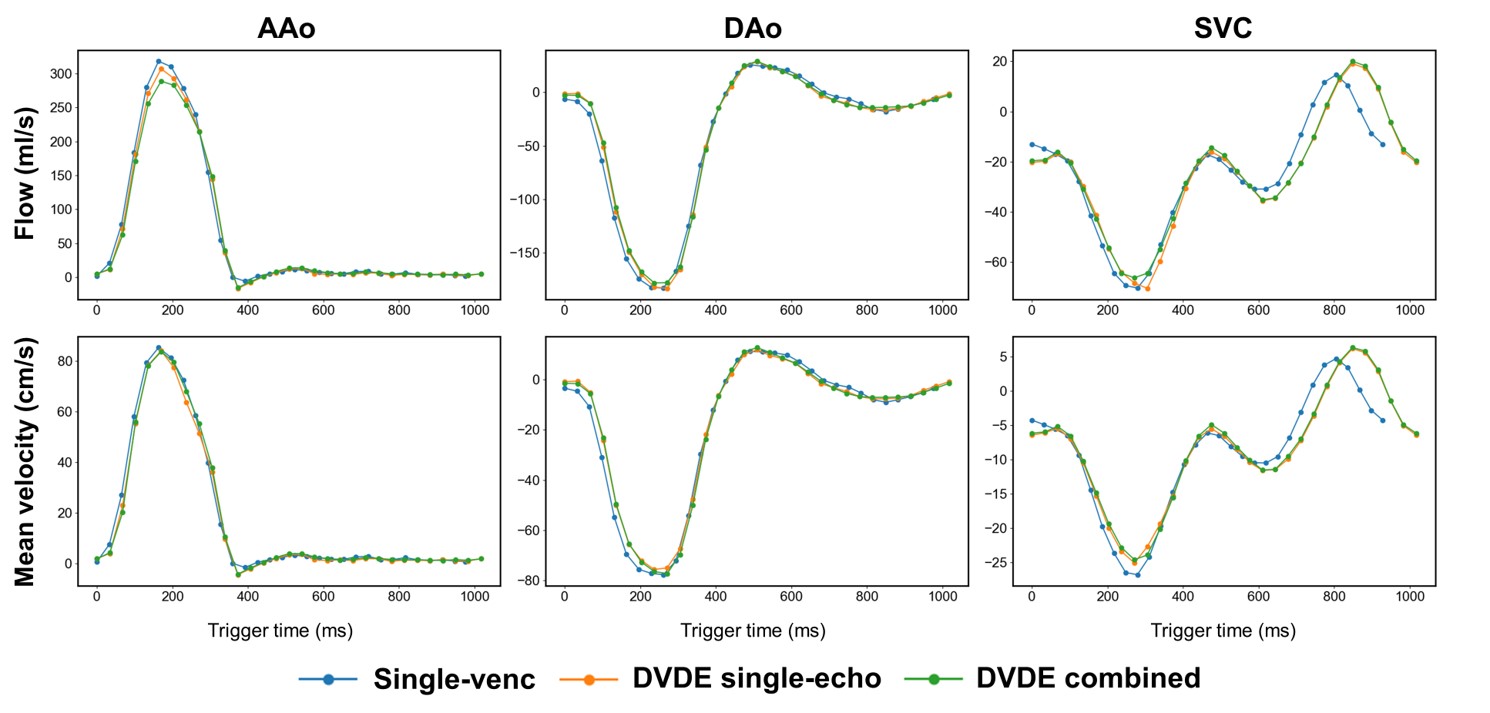
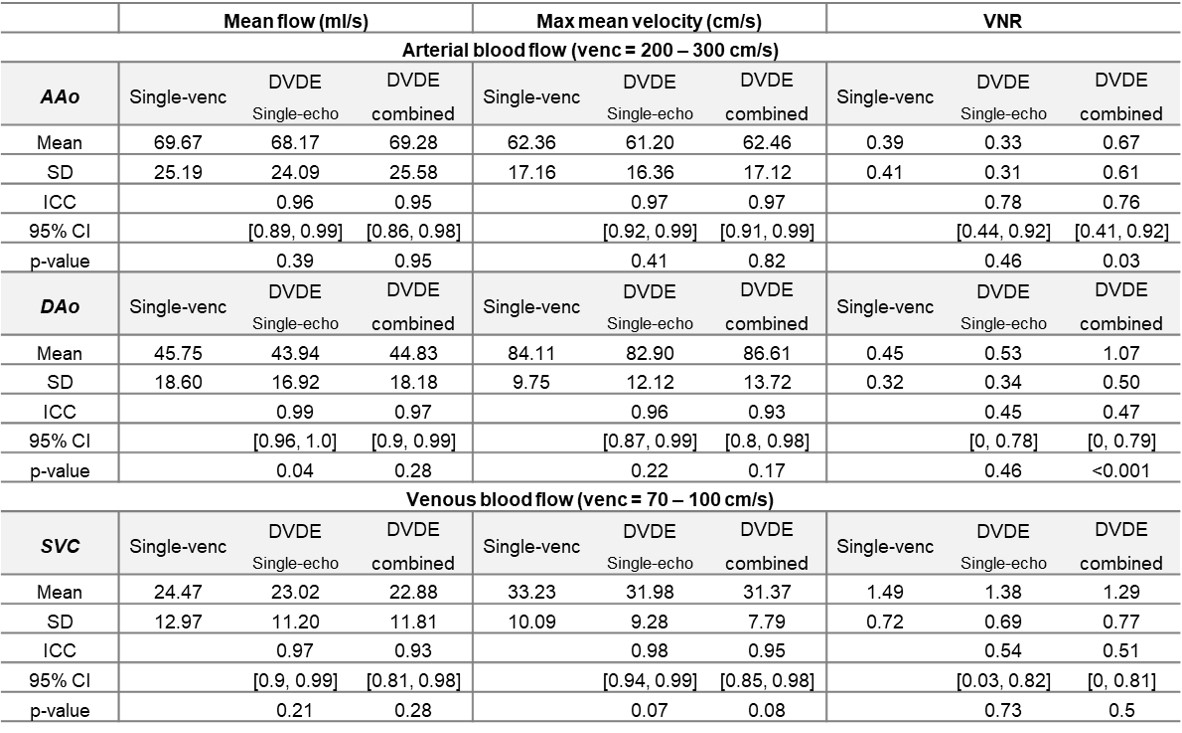
Fig. 1 shows typical phase images from the single-venc, DVDE single-echo, and DVDE combined. Single-venc and DVDE single-echo images show similar phase patterns, while DVDE combined shows increased VNR in all vessels without velocity aliasing artifact. For both arterial and venous blood flow, both DVDE single-echo and DVDE combined had a similar mean blood flow compared to single-venc (Table 1 and Fig. 2). Both DVDE single-echo and DVDE combined had a similar maximum mean velocity compared to the single-venc (Table 1 and Fig. 2). In all vessels, DVDE single-echo had a similar VNR compared to the single-venc. For venous blood flow, there was no difference in VNR between DVDE combined and the low venc conventional single-venc. For arterial blood flow, DVDE combined demonstrated a higher VNR vs. the high venc conventional single-venc.Conclusions
Compared to the single-venc PC-MRI, DVDE allows simultaneous imaging of arterial and venous blood flow with an enhanced VNR and similar blood flow and velocity. Simultaneous measurement of arterial and venous blood flow with three-directional velocity-encoding in 4D-flow will be evaluated in the future.Acknowledgements
No acknowledgement found.References
[1] Pelc NJ, Herfkens RJ, Shimakawa A, Enzmann DR. Phase contrast cine magnetic resonance imaging. Magn Reson Q 1991;7:229–254.
[2] Jang J, Zhao Y, Smink J, Powell JP. Moghari HM. Dual-venc dual-echo cardiovascular phase-contrast MRI. SCMR 2021.
[3] Ajala A, Zhang J, Pednekar A, Buko E, Wang L, Cheong BY, Hor PH, Muthupillai R. Mitral valve flow and myocardial motion assessed with dual-echo dual-velocity cardiac MRI. Radiology: Cardiothoracic Imaging. 2020 Jun 25;2(3):e190126.
Figures