1301
Optimization of an MRI protocol for non-contrast saccule and utricle visualization at 1.5T1Canon Medical Systems Spain and Portugal, Barcelona, Spain, 2Canon Medical Systems Corporation, Tochigi, Japan, 3Canon Medical Systems Europe, Zoetermeer, Netherlands
Synopsis
This study evaluates the feasibility of different approaches for the visualization of endolymphatic content in inner ear structures on 1.5T MR systems without the need of contrast injection. The results show that using an optimized high-resolution 3D T2w sequence combined with DLR-based denoising tools it is possible to visualize the utricle and saccule structures on healthy volunteers. The next step will be testing this technique on patients with endolymphatic hydrops.
INTRODUCTION
Various techniques have been developed over the last years to observe endolymphatic hydrops through MRI. Most of them require the injection of contrast agent with subsequent waiting times in order to enhance the contrast difference between endolymph and perilymph [1][2]. Some other studies have developed protocols that did not require contrast injection, but they all have been performed using a 3T system due to the exigent requirements in terms of image resolution and tissue contrast [3][4]. The aim of this study was to optimize on healthy volunteers an MR technique for saccule and utricle visualization on a 1.5T system without the need of contrast injection, by benefiting from advanced tools such as denoising based on Deep Learning Reconstruction (DLR).METHODS
Six healthy volunteers were scanned on a Vantage 1.5T Orian XGO 1.5T MR system (Canon Medical Systems Corporation, Tochigi, Japan) using a 16ch head and neck coil. For the MR protocol optimization, two different approaches were tested. The first one consisted in finding the optimal inversion time (TI) for endolymph and perilymph differentiation on a 3D FLAIR sequence, reproducing some previous work that was done on a 3T system [3]. Acquisitions with 15 increasing TI values between 208 and 3000ms were performed, and the resulting images were evaluated to determine the point with the optimal visualization of the endolymph. The second approach consisted in building a high-resolution (HR) 3D T2-weighted (T2w) sequence and evaluating the endolymph visualization. A DLR-based denoising solution [5] was applied and adjusted in order to improve SNR. 3D FLAIR sequence was performed with the following parameters: FASE3D, TR=7000ms, TE=475.2ms, TI=3000ms, recon. resolution=isotropic 0.45mm, acquisition time=7min. For HR 3D T2w the parameters were the following: FASE3D, TR=5000ms, TE=400ms, recon. resolution=isotropic 0.25mm, acquisition time=7:20min. Image evaluation was performed by visual inspection in order to assess vestibular endolymph depiction. The focus was especially on saccule and utricle visualization for the corresponding MPRs, while comparing the images with and without DLR. Signal profile plots in axial planes were used to evaluate the structures differentiation.RESULTS
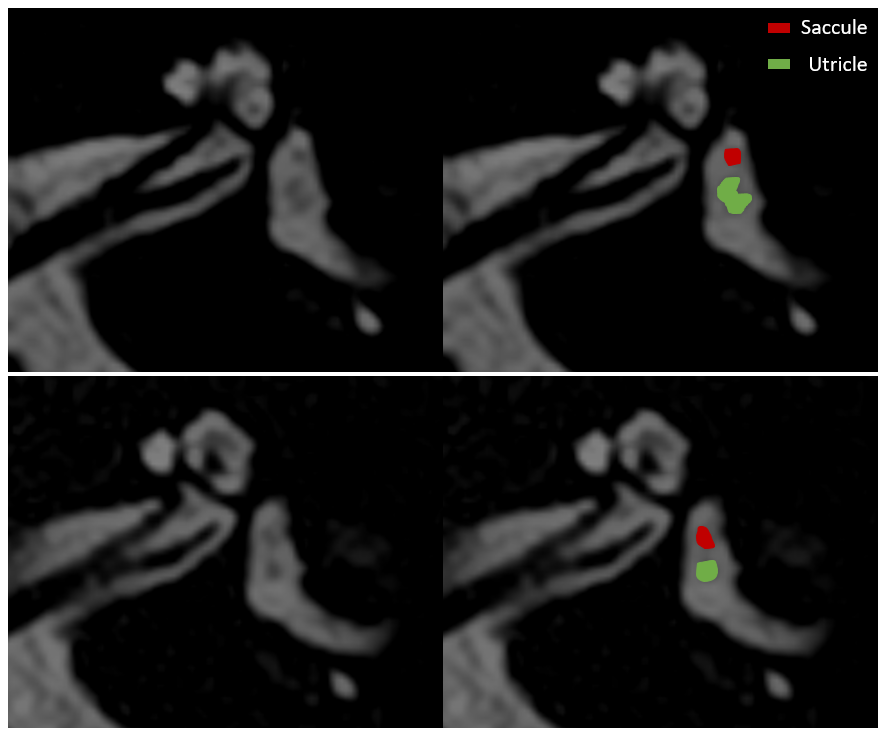
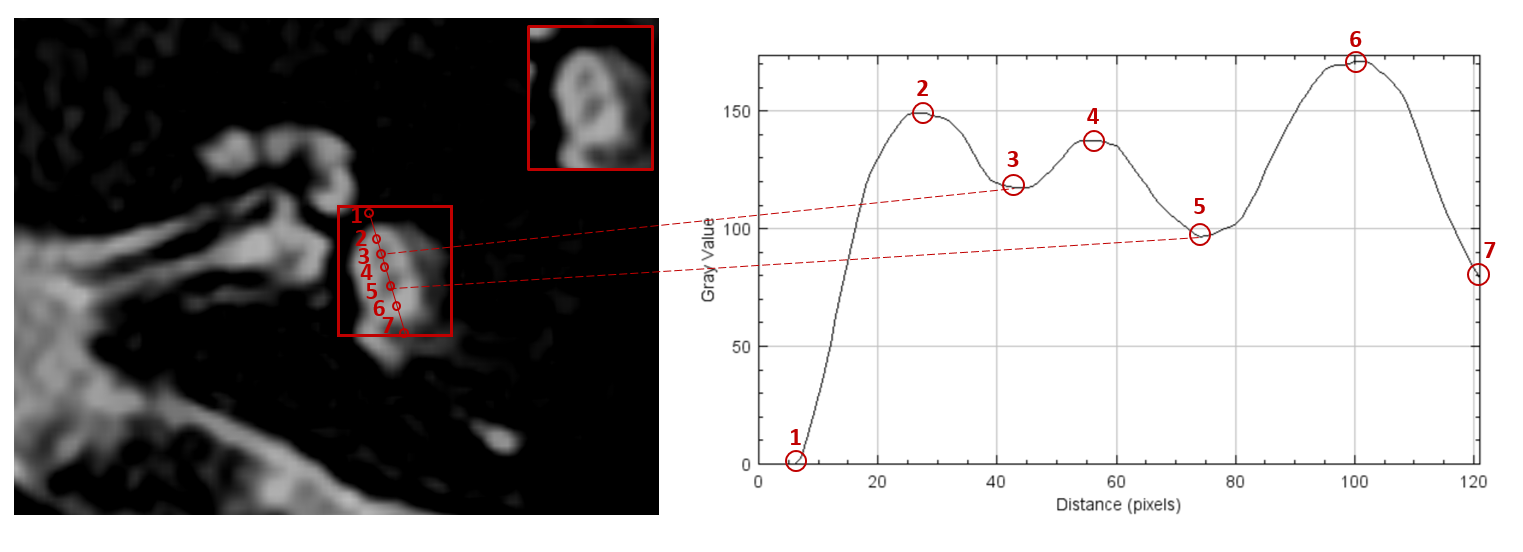
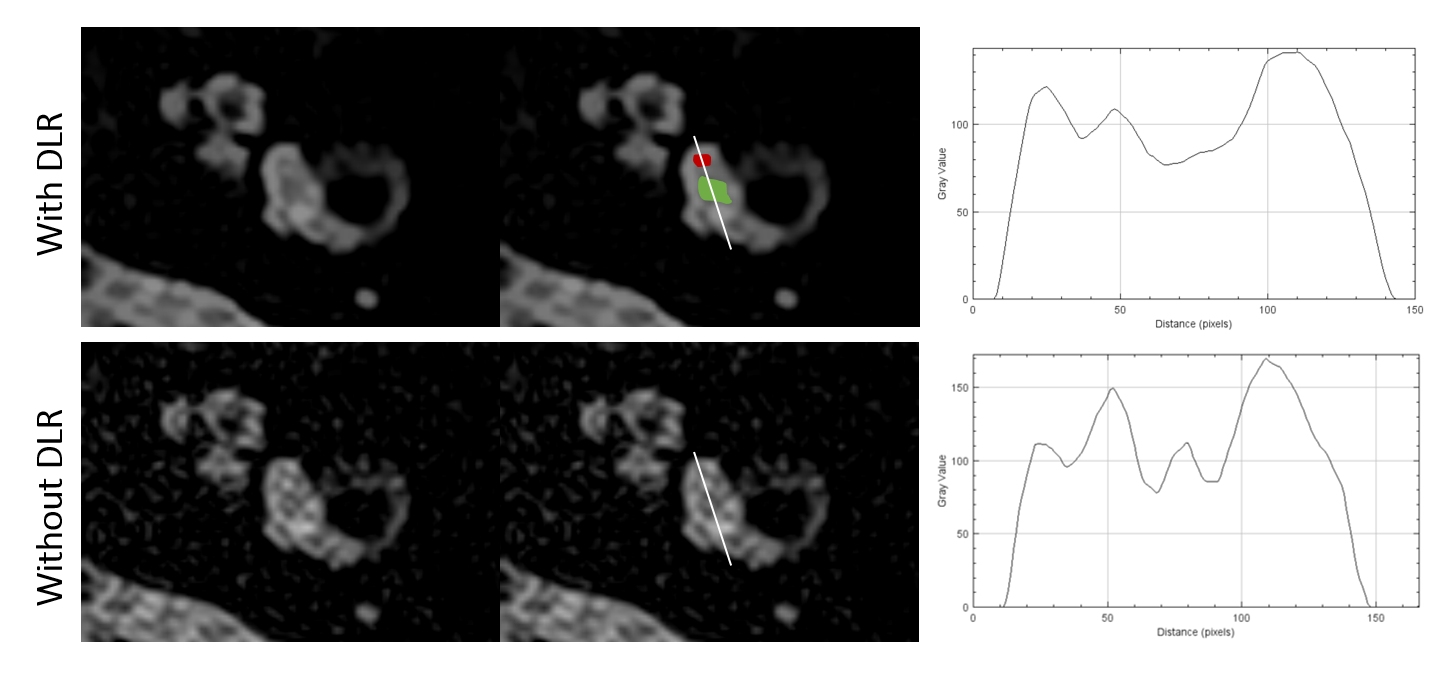
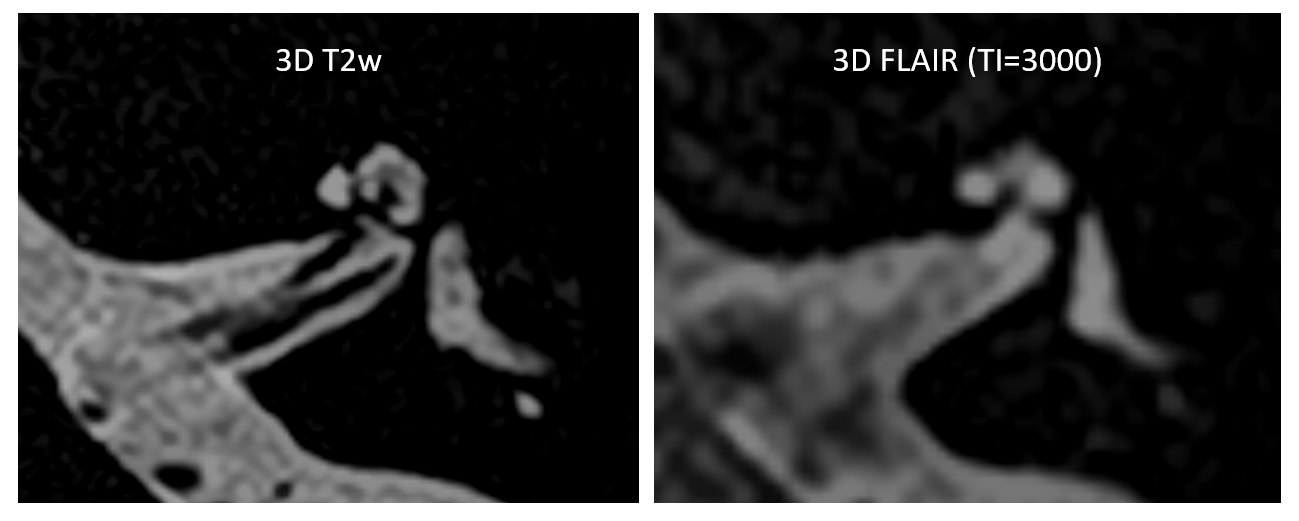
The 3D T2w sequence allowed visualizing the endolymphatic content, as it presented a lower signal that the perilymph surrounding it (Figure 1). After applying DLR, the vestibular endolymphatic content was clearly identifiable for all the cases after reconstructing the image in the adequate axial plane, independently for each ear. On profile plots (Figure 2) saccule and utricle differentiation was confirmed in 83.3% of the cases (10 out of 12). For the same acquisitions without DLR, visualization of endolymphatic content was still possible in most cases, but the capacity to differentiate the saccule and the utricle was reduced due to the noise (Figure 3). On the contrary, the 3D FLAIR approach resulted in images with poor endolymph-to-perilymph contrast in comparison with the 3D T2w acquisitions. Endolymph was not identified in most cases (Figure 4).DISCUSSION
The 3D T2w approach outperformed the 3D FLAIR one both in resolution and in contrast between endolymph and perilymph. The Inversion Recovery (IR) pulse from the FLAIR sequence caused a significant signal decrease, limiting the acceptable resolution that can be achieved. FLAIR only allowed scanning with a 44% lower resolution while only being 4.5% faster. For all the TI values that were tested, the images showed low contrast between endolymph and perilymph, preventing to reproduce the previous study at 3T [3] and to find a TI value that clearly differentiates the two structures. One hypothesis for this low contrast could be linked to the impossibility to use T2Prep values higher than 200ms, while in the 3T study they required a value of 400ms to obtain optimal results [3]. While 3D T2w used a higher resolution and could suffer from higher noise, DLR denoising allowed to recover a SNR high enough to clearly identify the endolymphatic structures. For the images processed without DLR, structures’ delineation was more challenging, or even not possible in some cases.CONCLUSION
This study concludes that it is possible to visualize endolymphatic structures at 1.5T, without the need of contrast agent injection, when using 3D T2w images in combination with denoising tools based on deep learning. Future studies will perform this 3D T2w sequence on patients suffering from inner ear disorders such as endolymphatic hydrops and will evaluate how these are visualized.Acknowledgements
No acknowledgement found.References
[1] Naganawa S, Nakamichi R, Ichikawa K, Kawamura M, Kawai H, Yoshida T, Sone M. MR Imaging of Endolymphatic Hydrops: Utility of iHYDROPS-Mi2 Combined with Deep Learning Reconstruction Denoising. Magn Reson Med Sci. 2021 Sep 1;20(3):272-279
[2] Baráth K, Schuknecht B, Naldi AM, Schrepfer T, Bockisch CJ, Hegemann SC. Detection and grading of endolymphatic hydrops in Menière disease using MR imaging. AJNR Am J Neuroradiol. 2014 Jul;35(7):1387-92
[3] Fukutomi, Barreau et al. ISMRM proceedings 2021, nr 3927
[4] Venkatasamy A, Veillon F, Fleury A, Eliezer M, Abu Eid M, Romain B, Vuong H, Rohmer D, Charpiot A, Sick H, Riehm S. Imaging of the saccule for the diagnosis of endolymphatic hydrops in Meniere disease, using a three-dimensional T2-weighted steady state free precession sequence: accurate, fast, and without contrast material intravenous injection. Eur Radiol Exp. 2017;1(1):14
[5] Kidoh M, Shinoda K, Kitajima M, Isogawa K, Nambu M, Uetani H, et al. Deep Learning Based Noise Reduction for Brain MR Imaging: Tests on Phantoms and Healthy Volunteers. Magn Reson Med Sci. 2019
Figures