1226
Repeatability and reliability of 2D phase-contrast and 4D flow MRI when measuring cerebral arterial and venous pulsatility1Centre for Clinical Brain Sciences, University of Edinburgh, Edinburgh, United Kingdom, 2Siemens Medical Solutions USA, Inc., Cleveland, OH, United States
Synopsis
We examined the test-retest repeatability and intraobserver reliability of 4D flow MRI while assessing the pulsatility and flow rates of a variety of cerebral arteries and veins in healthy volunteers. A subset of these vessels were also measured using 2D phase-contrast MRI, a more established method, to assess the level to which the lower-resolution (but higher-coverage) 4D method could compare to its 2D counterpart. Flow pulsatility appears to play a role in the development of cerebral small vessel disease and so testing the capabilities of 4D flow in this context is an important step before applying it to clinical studies.
Introduction
Intracranial vessel stiffness (manifest as pulsatility of flow) is implicated in the development of cerebral small vessel disease (SVD)1. Techniques such as transcranial Doppler ultrasound and 2D phase-contrast MRI (PC-MRI) allow us to assess blood flow velocity within the brain but come with certain drawbacks such as operator-dependency and limitation to insonation windows. The emergence of 4D flow MRI allows us to measure blood flow across a relatively large vascular network in a single acquisition, but evidence of reliability and repeatability is scarce.Subjects and methods
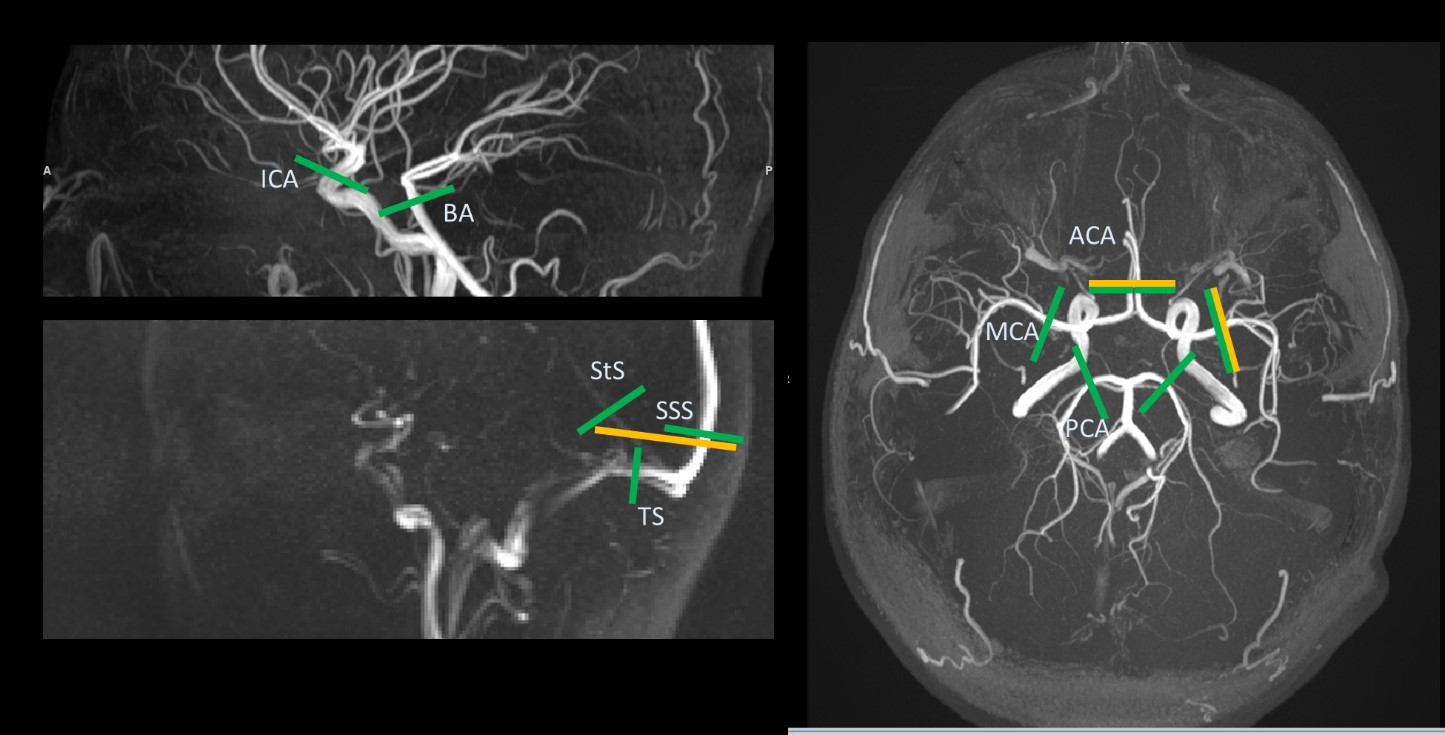
We scanned healthy volunteers at 3T (MAGNETOM Prisma with a 32-channel head coil, Siemens Healthcare, Erlangen, Germany), each over two sessions on a single day. 2D phase-contrast MRI with retrospective peripheral pulse gating was used to examine the right middle cerebral artery (RMCA) (TE/TR: 6.17/10.34ms, flip angle (FA): 12°, temporal resolution: 20.68ms, VENC: 80cm/s, voxels: 0.85x0.85x3.1mm3), anterior cerebral arteries (ACAs) (TE/TR: 6.24/10.44ms, FA: 12°, temporal resolution: 20.88ms, VENC: 70cm/s, voxels: 0.83x0.83x3.1mm3), and the venous sinuses (TE/TR: 6.62/10.94ms, FA: 12°, temporal resolution: 21.88ms, VENC: 50cm/s, voxels: 0.71x0.71x3.1mm3) (Figure 1). Prototype 4D phase-contrast MRI with retrospective peripheral pulse gating was used to capture a volume (180x224x40mm3) containing all major cerebral vessels (TE/TR: 2.85/5.48ms, FA: 7°, temporal resolution: 87.68 ms, VENC: 100cm/s voxels: 1x1x1mm3). Analysis of the RMCA and superior sagittal sinus (SSS) from both 2D and 4D images was repeated by one analyst to test intraobserver reliability. In-house Matlab code was used to extract flow data and subsequently calculate pulsatility using a modified Gosling’s2 pulsatility index equation (PI = (flowmax – flowmin)/ flowmean)). Intraclass correlation coefficients (ICC) and Bland-Altman plots were used to assess method conformity and repeatability.Results
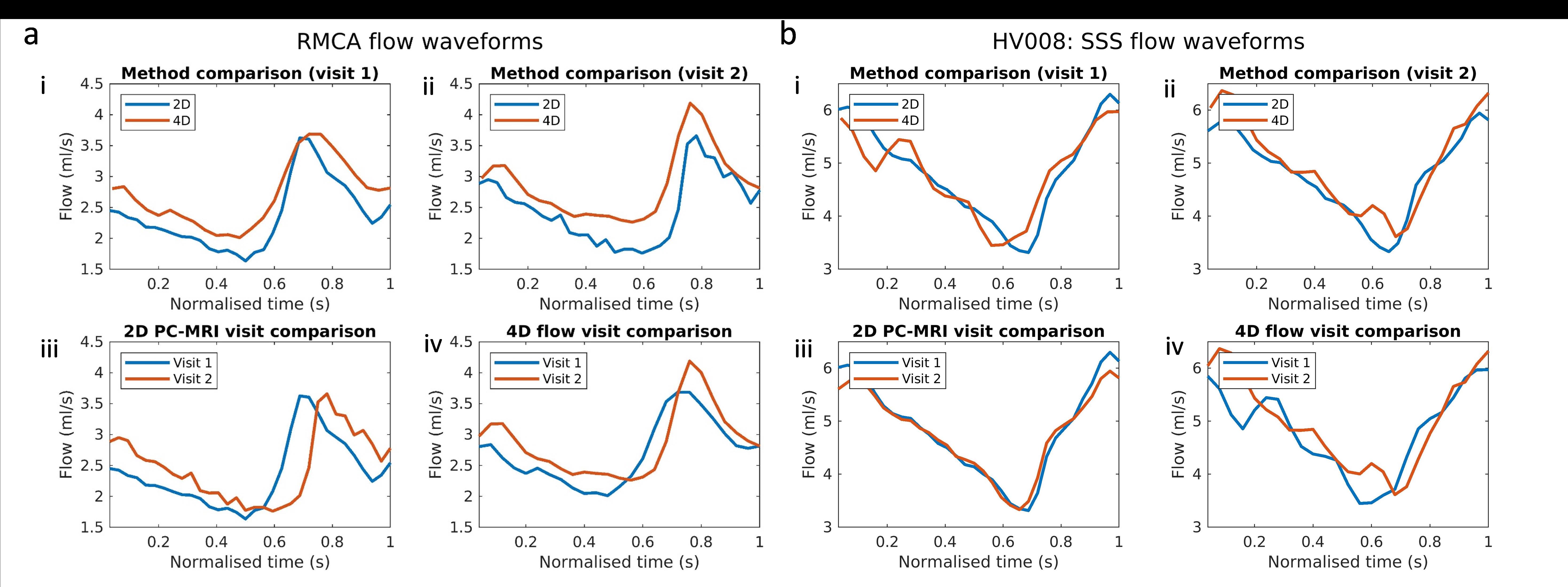
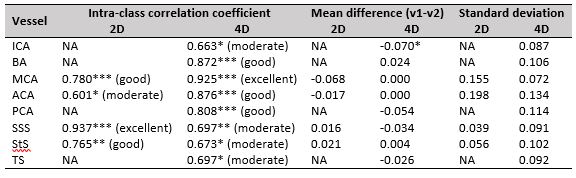
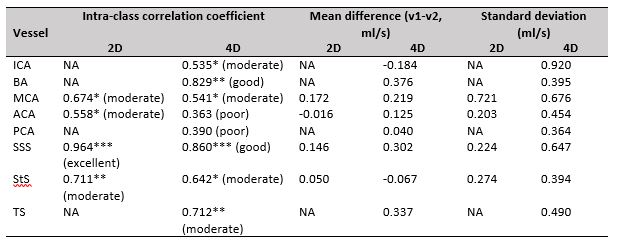
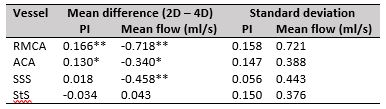
We recruited 11 healthy volunteers (mean age 31.64±12.01 years, 7 males), of whom 10 had complete MRI data across both visits. Intraobserver reliability: With 2D data, ICC scores of 0.991 and 0.999 (excellent) were found for intraobserver reliability of the RMCA and SSS PI measurements, respectively. With 4D data, ICC scores of 0.877 (good) and 0.906 (excellent) were found. Mean flow measurements were more consistent in the 2D (ICC = 0.975-0.999) than the 4D (ICC = 0.459-0.723) method. Test-retest repeatability: Across the RMCA, ACAs, and veins, the 2D PI measurements showed overall good repeatability (ICC = 0.601-0.937) - with the smaller ACAs providing the lowest scores - and an overall mean difference between visits of -0.012 ± 0.041. The 4D PI measurements showed good repeatability across thirteen vessels (ICC 0.564 – 0.925) - with the ICAs and ACAs providing the lowest scores - and a mean difference between visits of -0.002 ± 0.038 across the thirteen individual vessels. Mean flow repeatability was mostly moderate in 2D (ICC = 0.558-0.964) and 4D (ICC = 0.363-0.860) cases. Method comparisons: The mean differences in PI between methods range from -0.034 to 0.166 (overall mean 0.07 ± 0.094) across the four vessels assessed using both, indicating underestimation by the 4D method. Mean differences in flow between methods range from -0.718 to 0.043 ml/s (overall mean -0.368 ± 0.316 ml/s), with nearly all values negative – indicating overestimation by 4D flow compared to 2D.Discussion
Both scan types showed good repeatability for PI measurements but mean flow measurements were less repeatable. As expected, the smaller and more tortuous vessels (such as the ACAs and ICAs) provided the most challenge due to resolution limitations and slice placement, respectively. VENC in the 2D scans was not sufficient in some MCA cases, resulting in aliasing that had to be corrected. This likely reduced the 2D MCA ICC scores. Furthermore, the 4D VENC of 100cm/s across the whole volume was sufficient to prevent aliasing. While some 2D scans had to be repeated due to initial suboptimal slice placement, 4D flow acquires a single volume which can be processed post-hoc and therefore reduces wasted time. Both 2D and 4D method showed high intraobserver reliability (again, for PI more so than flow), with the 2D method showing slightly more so. This is likely due to 2D processing taking place on single pre-acquired slices (leaving little room for variation between repeats) whereas the 4D volume had to be ‘resliced’ at the desired location each time (leaving more room for variation). The 2D results often showed higher PI than the 4D results. This is likely due to higher spatiotemporal resolutions of the former method, potentially allowing pulsatile flow to be more accurately sampled. The lower resolution of our 4D scan likely led to partial volume effects in some vessels and therefore flow overestimation. Several studies have compared 4D flow with 2D PC-MRI and found strong correlations across techniques when measuring flow in the internal carotid3, basilar4, and cerebral arteries4-6. However, this is the first time that this many cerebral arteries and veins have been examined using single 4D flow acquisitions across repeat visits, with valuable comparisons between 2D and 4D methods.Conclusion
The 4D flow sequence used here demonstrates a relatively fast scan (~10-15 mins) that is capable of assessing the pulsatility of major cerebral vessels with good repeatability and accuracy in relation to 2D PC-MRI. 4D flow in fact often demonstrated better repeatability than 2D PC-MRI, suggesting we can be fairly confident in its application when measuring cerebral pulsatility.Acknowledgements
We gratefully acknowledge Michael Stringer for his advice on the initial phase-contrast code set-up and processing, Francesca Chappell for her statistical knowledge, and Yulu Shi for the 2D PC-MRI processing methodology.References
1. Shi Y, Thrippleton MJ, Blair GW, et al. Small vessel disease is associated with altered cerebrovascular pulsatility but not resting cerebral blood flow. J Cereb Blood Flow Metab. 2018: 271678X18803956.
2. Gosling RG and King DH. Arterial assessment by Doppler-shift ultrasound. Proc R Soc Med. 1974; 67: 447-9.
3. Schrauben E, Wahlin A, Ambarki K, et al. Fast 4D flow MRI intracranial segmentation and quantification in tortuous arteries. J Magn Reson Imaging. 2015; 42: 1458-64.
4. Meckel S, Leitner L, Bonati LH, et al. Intracranial artery velocity measurement using 4D PC MRI at 3 T: comparison with transcranial ultrasound techniques and 2D PC MRI. Neuroradiology. 2013; 55: 389-98.
5. Dunas T, Holmgren M, Wahlin A, et al. Accuracy of blood flow assessment in cerebral arteries with 4D flow MRI: Evaluation with three segmentation methods. J Magn Reson Imaging. 2019.
6. Wahlin A, Ambarki K, Birgander R, et al. Measuring pulsatile flow in cerebral arteries using 4D phase-contrast MR imaging. AJNR Am J Neuroradiol. 2013; 34: 1740-5.
Figures