1195
A Monte Carlo Analysis of Guidewire Safety Comparing a Body and Local Coil Array1Radiology, University of California, Sacramento, CA, United States, 2Biomedical Engineering Department, School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3Perinatal Imaging, King's College London, London, United Kingdom, 4Center for Image Sciences, University Medical Center Utrecht, Utrecht, Netherlands, 5Biomedical Engineering, Medical Imaging Analysis, Eindhoven University of Technology, Eindhoven, Netherlands
Synopsis
Metallic Endovascular devices can be unsafe when used during MR guided procedures. A potential solution to the heating problem might be to use a local coil instead of a body coil to excite the imaging volume. In this work we present a Monte Carlo analysis using many random guidewire trajectories and the transfer function to estimate the scatter electric field at the guidewire tip imbedded in a heterogenous dielectric.
Introduction
The use of interventional devices is limited due to heating caused by coupling of the device to the MR scanner’s RF coils. Methods based on parallel transmit have been used to make devices safe1–3, while others have reduced the power of the pulse sequence directly4. In a previous abstract we showed that a body coil can cause more implant/device/tip heating than a local transmit coil array5. However, that data shows results for a single geometrical guidewire trajectory in a homogeneous dielectric. To further understand the combined influence of geometry and heterogenous dielectric medium, we sought through simulation, to generate multiple random guidewire trajectories and evaluate their potential for heating using the transfer function approach6. In this work we compare the predicted scattered electric field at the guidewire tip when excited by a local coil array or a body coil.Methods
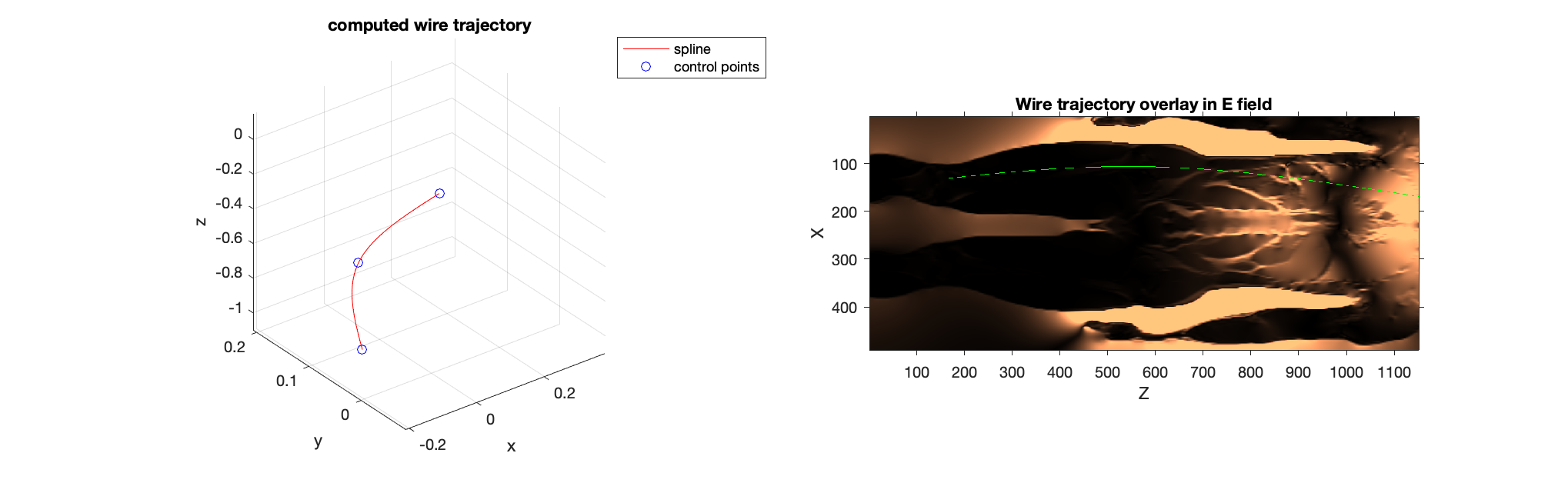
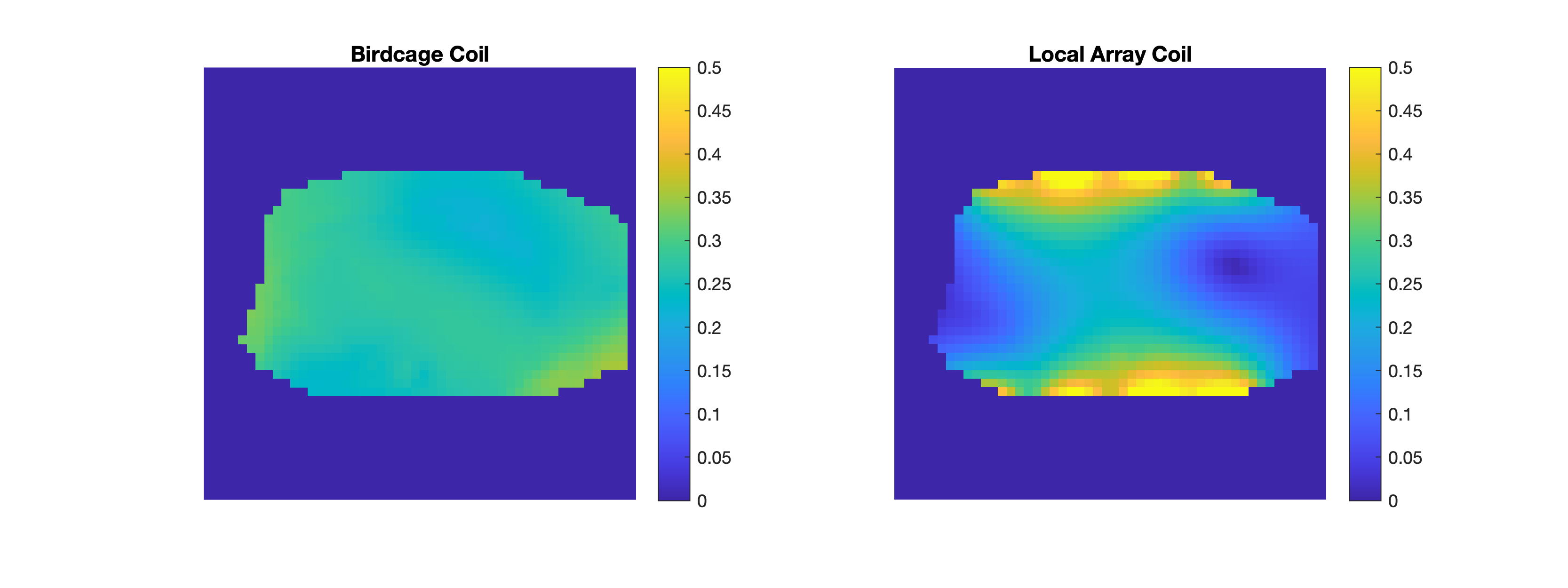
The transfer function7 for 44cm and 100cm long wires in a dielectric medium (permittivity =79, Sigma = 0.47 Sm-1) was calculated from simulated (Sim4Life, ZMT, Zurich, Switzerland) excitation with a plane wave at the tip. The guidewire was modeled as an insulated 1mm wire with 5mm of the tip exposed by removing the insulation. A full human sized phantom, Duke8, was excited with a local coil array with 8 coil loops (200mm x 50mm) in CP mode, with 4 coils posterior and 4 anterior. The same Duke phantom was also excited with a body bird cage coil 45cm long with 16 rungs in a high-pass configuration. The electric field was scaled to so that the B1+ field was approximately equivalent within a region of interest (10cm x 10cm x 10cm) (figure 1). The random guidewire trajectories were generated using MatLab R2021a (MathWorks Inc, MA, USA) by randomly selecting a set of 3 control points with the ‘rand’ function and computing the trajectory of a spline connecting the control points (figure 1). The spline was created constrained to the control points using the function ‘cscvn()’. A total of 10,000 trajectories were modeled.The scattered electric field produced at the guidewire tip was computed by integrating the tangential component of the electric field produced by either of the simulated coils along each wire trajectory multiplied by the relevant wire transfer function.
Results
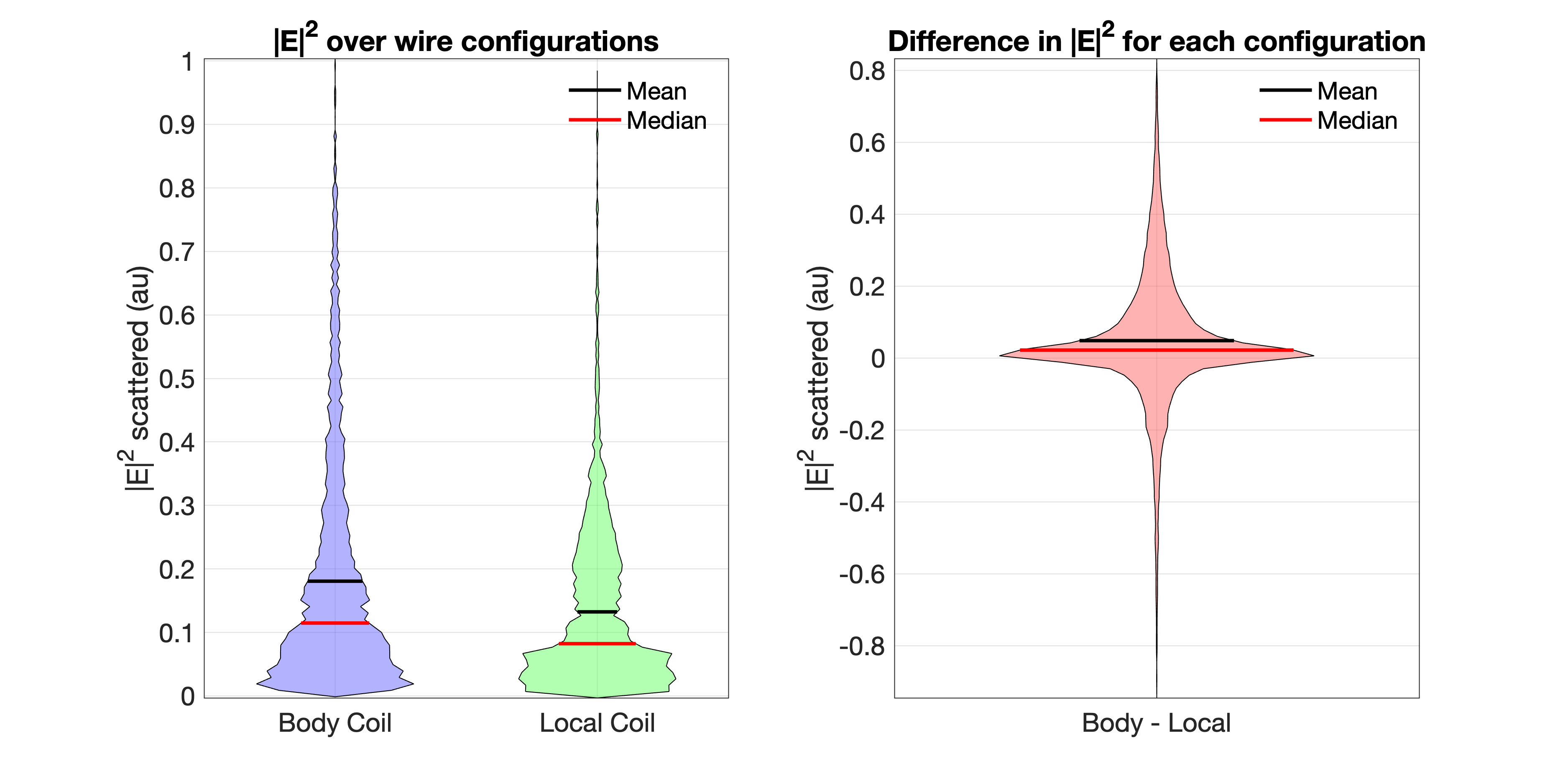
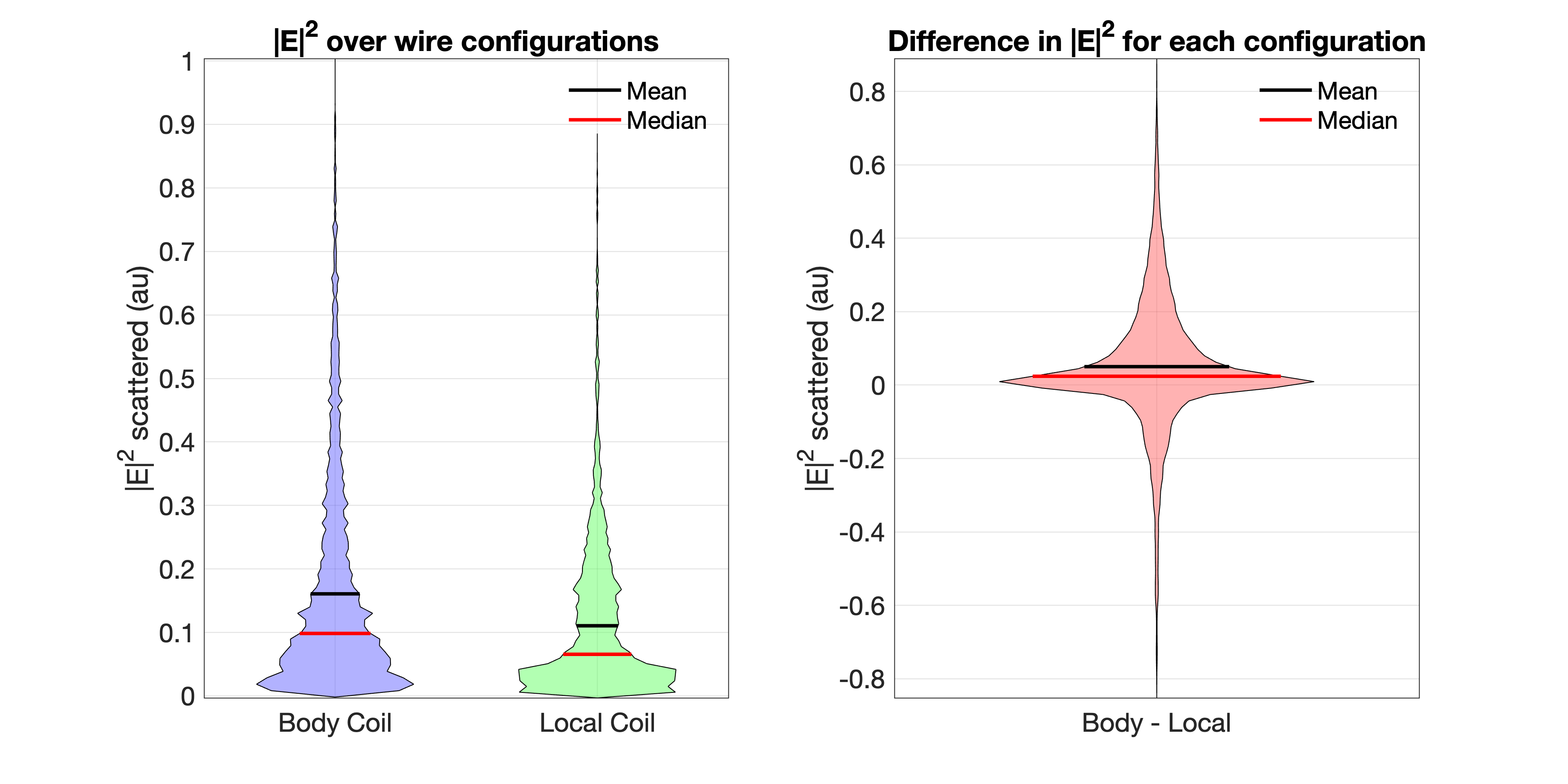
The B1 maps are shown in figure 2. In figure 3, a violin plot shows the scattered electric field produced by the local and body coil across all trajectories for the 44cm long wire. The same is shown in figure 4 for the 1m long wire. The difference between the body coil and local coil array is also shown in figure 3 and 4. For the 1m long wire, the body coil to local coil array ratio for the 50th , 95th, and 99th percentile values were 1.5, 1.6, and 1.26, respectively. This means that the median scattered field is 50% higher, while the 99th percentile (close to worst case) is 26% higher for the body coil.Discussion
The local coil array produces less scattered field at the guidewire tip on average, 20-34% less, compared to the body coil, when the B1 field in a region of interest is matched. However our results imply that unsafe conditions can exist in both coil types since there are trajectories for which the local coil array may perform worse (differences are both positive and negative). We note however that this approach is not exact and cannot properly characterize a condition in which a wire is partially withdrawn from the body, which is often the case for interventional MRI. This initial work helps to provide a general understanding of the complexity of the problem but further work on generation and validation of transfer functions is needed.Conclusion
We have compared a body coil with a local transmit coil array and numerically evaluated the heating risks that each can pose on many different guidewire trajectories in a dielectric medium. In most cases the local coil array was the safer coil.Acknowledgements
This work was supported by core funding from the Wellcome/EPSRC Centre for Medical Engineering [WT203148/Z/16/Z] and by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Guy’s and St Thomas’ NHS Foundation Trust and King’s College London and/or the NIHR Clinical Research Facility. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care.References
1. Godinez, F. et al. An 8 channel parallel transmit system with current sensor feedback for MRI-guided interventional applications. Physics in Medicine & Biology (2021) doi:10.1088/1361-6560/ac2fbe.
2. Etezadi-Amoli, M., Stang, P., Kerr, A., Pauly, J. & Scott, G. Controlling radiofrequency-induced currents in guidewires using parallel transmit. Magnetic Resonance in Medicine 74, 1790–1802 (2015).
3. Eryaman, Y., Turk, E. A., Oto, C., Algin, O. & Atalar, E. Reduction of the radiofrequency heating of metallic devices using a dual-drive birdcage coil. Magnetic resonance in medicine : official journal of the Society of Magnetic Resonance in Medicine / Society of Magnetic Resonance in Medicine 69, 845–52 (2013).
4. Campbell-Washburn, A. E. et al. Right heart catheterization using metallic guidewires and low SAR cardiovascular magnetic resonance fluoroscopy at 1.5 Tesla: First in human experience. Journal of Cardiovascular Magnetic Resonance 20, 1–9 (2018).
5. Godinez, F., Scott, G., Hajnal, J. v. & Malik, S. J. Is a Local Tx Coil Sufficient for Guidewire Safety in MRI? in Proc. Intl. Soc. Mag. Reson. Med. 29 2310 (ISMRM, 2021).
6. Steensma, B. R. et al. Effect of transmit frequency on RF heating of metallic implants. in Proc. Intl. Soc. Mag. Reson. Med. 29 0357 (2021).
7. Park, S. M., Kamondetdacha, R. & Nyenhuis, J. A. Calculation of MRI-induced heating of an implanted medical lead wire with an electric field transfer function. Journal of Magnetic Resonance Imaging 26, 1278–1285 (2007).
8. Christ, A. et al. The Virtual Family - Development of surface-based anatomical models of two adults and two children for dosimetric simulations. Physics in Medicine and Biology 55, (2010).
Figures