1169
Dissolved 129Xe spectroscopy in the lungs of preterm-born children
Ho-Fung Chan1, Guilhem J Collier1, Laurie J Smith1, Alberto M Biancardi1, Jody Bray1, Helen Marshall1, Paul J.C Hughes1, Madhwesha Rao1, Graham Norquay1, Andrew J Swift1, Kylie Hart2,3, Michael Cousins2,3, Sailesh Kotecha2,3, and Jim M Wild1
1Infection, Immunity and Cardiovascular Disease, University of Sheffield, Sheffield, United Kingdom, 2Child Health, Cardiff University School of Medicine, Cardiff, United Kingdom, 3Neonatal Unit, Cardiff and Vale University Health Board, Cardiff, United Kingdom
1Infection, Immunity and Cardiovascular Disease, University of Sheffield, Sheffield, United Kingdom, 2Child Health, Cardiff University School of Medicine, Cardiff, United Kingdom, 3Neonatal Unit, Cardiff and Vale University Health Board, Cardiff, United Kingdom
Synopsis
Ventilation defects and increased alveolar heterogeneity have been observed previously with 129Xe MRI in preterm-born children. We hypothesised that reduced gas exchange in preterm-born children could be measured with dissolved 129Xe whole lung spectroscopy. The ratio of red blood cells (RBC) to tissue/plasma (TP) signals (RBC/TP) was significantly elevated in the lungs of 34 preterm-born children compared with 16 term-born children. This trend was unexpected and we hypothesise that in preterm-born children a reduced number of alveolar septa due to birth at an early stage of lung development can lead to decreased TP signal and thus increased RBC/TP ratio.
Introduction
Babies born preterm (<37 weeks’ gestation) are at risk of decreased lung function in childhood and beyond due to a combination of birth at an early stage of lung development and exposure to antenatal and postnatal factors that can lead to the development of bronchopulmonary dysplasia (BPD)1. Hyperpolarised 129Xe MRI is safe and well-tolerated in paediatric subjects and could play a role in phenotyping different lung diseases resulting from preterm-birth. Previously, ventilation defects and increased alveolar heterogeneity were demonstrated in the lungs of preterm-born children with 129Xe MRI2. However, the sensitivity of dissolved 129Xe MRI to gas transfer limitations has not yet been explored in these children. Transfer factor of the lung for carbon monoxide (TLCO) has been demonstrated to be lower in preterm-born children compared with healthy term-born controls3,4, and we hypothesised that similar differences could be measured with hyperpolarised dissolved 129Xe spectroscopy.Methods
50 children aged 9-13 years, including 34 preterm-born (≤34 weeks’ gestation) and 16 term-born controls, were imaged with hyperpolarised 129Xe MRI on a 1.5T GE HDx scanner using a transmit/receive quadrature vest coil as part of the Respiratory Health Outcomes in Neonates study (RHiNO, EudraCT: 2015-003712-20). Dissolved 129Xe whole lung spectroscopy was acquired after inhalation of a gas mixture of 129Xe and N2 from functional residual capacity (FRC) and a 15 second breath-hold. Gas mixture volume and 129Xe doses5 (300-500 mL) were adjusted according to the subjects’ heights to account for differences in lung volume and 129Xe concentration. Sequence parameters were: BW=8 kHz, 512 pts, 200 averages, TR=74 ms, and 22° flip angle. A double Lorentzian fit of the whole lung spectroscopy data in the frequency domain was performed6 to derive T2* values of the tissue/plasma (TP) and red blood cell (RBC) peaks, and the ratio of RBC to TP signals (RBC/TP). A single Lorentzian fit was also performed on the gas peak to determine the reference gas frequency to calculate the RBC and TP frequency shifts.The RHiNO study groupings were defined as: preterm with low lung function (PTLow, percent predicted FEV1≤85%), preterm with normal lung function (PTNorm, %FEV1>85%) and term-born controls. The 34 preterm-born children were also grouped based upon their diagnosis of BPD (supplemental oxygen dependency at 28 days of age in the neonatal period) (PTBPD) or into preterm without BPD (PTnBPD). Kruskal-Wallis tests with post-hoc Dunn’s correction for multiple comparisons were performed to assess differences across the stratified %FEV1 or BPD groups against the term-born controls for all 129Xe spectroscopy metrics and subject demographics. Non-parametric Spearman’s correlation was used to assess correlations between 129Xe spectroscopy metrics and demographics across all subjects.
Results and Discussion
Subject demographics and 129Xe spectroscopy metrics are shown in Table 1. 129Xe RBC/TP in the healthy term-born children (mean age=11yrs; RBC/TP=0.42) was smaller than the reported ratio in healthy adults (mean age=41yrs; RBC/TP=0.56) using the same spectroscopy sequence (Figure 1)7. The mechanism behind this trend is likely to be due to increased haematocrit in adults resulting in increased 129Xe RBC signal8. This trend in RBC/TP also matches the changes in predicted TLCO with age where TLCO increases throughout childhood and slowly declines with advancing age in adults9.129Xe RBC/TP was significantly different for both %FEV1 (P=0.002) and BPD (P<0.001) stratified groups (Figure 2). No significant differences were observed between %FEV1 and BPD groups for the other 129Xe spectroscopy metrics. Significantly increased RBC/TP ratio was observed for preterm groups compared with term-born controls: PTLow (P=0.008), PTNorm (P=0.007), PTnBPD (P<0.001). Differences in RBC/TP between term-born and preterm-born children suggests that these differences are due to underlying preterm birth regardless of low FEV1 and/or BPD diagnosis. This is further supported by significant correlations of gestational age (P=0.014, r=0.344) and birthweight with RBC/TP (P=0.016, r=0.340) (Figure 3).
The increased 129Xe RBC/TP observed for preterm-born children, with respect to term-born controls, appears to be directly opposite to the expectation of decreased RBC/TP due to reduced gas transfer as a result of immature lungs having simplified alveoli geometry and reduced surface area1,3,4. While 129Xe RBC/TP has been shown to strongly correlate with gas transfer or exchange in a range of pulmonary diseases6,7,10, this biomarker is highly representative of the alveolar-capillary gas exchange surface. We hypothesise that in these preterm-born children the increased 129Xe RBC/TP is due to a decreased TP component resulting from simplified alveolar geometry with reduced alveolar septation1. Fewer alveolar septa leads to regions of enlarged alveoli and increased alveolar heterogeneity has been detected previously with 129Xe diffusion-weighted MRI2. A negative correlation between 129Xe mean alveolar dimension (LmD) and TP T2*, but no correlation between LmD and RBC T2* (Figure 4), further supports the fewer alveolar septa hypothesis by demonstrating that heterogeneity in the TP component (low TP T2*) is related to increased alveolar dimensions.
Conclusion
129Xe RBC/TP, derived from dissolved 129Xe spectroscopy, was significantly elevated in 34 preterm-born children compared with 16 term-born controls. We hypothesise that in preterm-born children simplification and reduced number of alveolar septa can result in decreased TP signal and thus increased RBC/TP ratio.Acknowledgements
This work was supported by the Medical Research Council (MR/M008894/1 and MR/M022552/1) and National Institute for Health Research grant (NIHR-RP-R3-12-027).References
- Moschino, L., L. Bonadies, and E. Baraldi, Lung growth and pulmonary function after prematurity and bronchopulmonary dysplasia. Pediatr Pulmonol, 2021. 56(11):3499-3508.
- Wild, J.M., et al., Imaging functional and microstructural changes in the lungs of children born prematurely. European Respiratory Journal, 2019. 54(suppl 63):PA3171.
- Arigliani, M., et al., Lung function between 8 and 15 years of age in very preterm infants with fetal growth restriction. Pediatr Res, 2021. 90(3):657-663.
- Hakulinen, A.L., et al., Diffusing capacity of the lung in school-aged children born very preterm, with and without bronchopulmonary dysplasia. Pediatric Pulmonology, 1996. 21(6):353-360.
- Norquay, G., et al., ^{129}Xe-Rb Spin-Exchange Optical Pumping with High Photon Efficiency. Phys Rev Lett, 2018. 121(15):153201.
- Kaushik, S.S., et al., Measuring diffusion limitation with a perfusion-limited gas--hyperpolarized 129Xe gas-transfer spectroscopy in patients with idiopathic pulmonary fibrosis. J Appl Physiol (1985), 2014. 117(6):577-85.
- Collier, G.J., et al., Dissolved (129) Xe lung MRI with four-echo 3D radial spectroscopic imaging: Quantification of regional gas transfer in idiopathic pulmonary fibrosis. Magn Reson Med, 2021. 85(5):2622-2633.
- Fulgoni, V.L., 3rd, et al., Establishing Pediatric and Adult RBC Reference Intervals With NHANES Data Using Piecewise Regression. Am J Clin Pathol, 2019. 151(2):128-142.
- Stanojevic, S., et al., Official ERS technical standards: Global Lung Function Initiative reference values for the carbon monoxide transfer factor for Caucasians. Eur Respir J, 2017. 50(3).
- Wang, Z., et al., Using hyperpolarized (129)Xe gas-exchange MRI to model the regional airspace, membrane, and capillary contributions to diffusing capacity. J Appl Physiol (1985), 2021. 130(5):1398-1409.
Figures

Table 1: Summary of
subject demographics, and dissolved 129Xe spectroscopy metrics for
each grouping of preterm-born children based on either %FEV1 or
diagnosis of BPD and term-born controls. P-values are shown for Kruskal-Wallis
tests between term-born controls and stratified %FEV1 and BPD
groups, respectively. All values are given as mean (standard deviation).
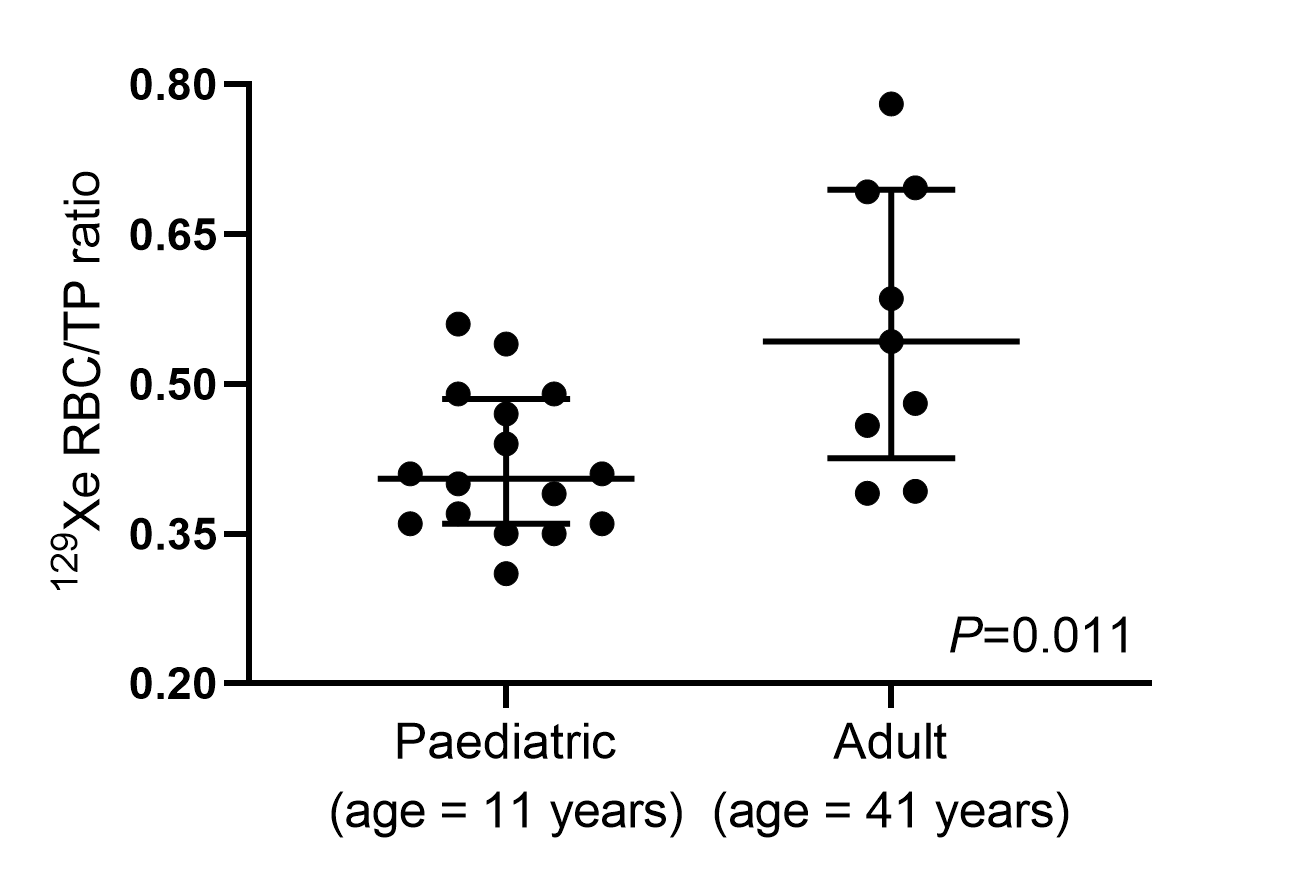
Figure 1: Plots of 129Xe
RBC/TP ratio calculated from dissolved 129Xe whole lung spectroscopy
in the term-born controls (mean age=11yrs) and healthy adults (mean age=41yrs)
reproduced from Collier et al.7. 129Xe
RBC/TP ratio was significantly decreased (P=0.011) in the paediatric subjects.

Figure 2: Plots of 129Xe RBC/TP ratio for term-born children and
preterm-born children either grouped by %FEV1 (a) or BPD diagnosis (b). P-values from Kruskal-Wallis tests (boxed p-value is for Dunn’s
multiple comparison tests between groups).

Figure 3: Plots demonstrating
significant correlations for 129Xe RBC/TP ratio with gestational age
(a) and birthweight (b) for the 50 children. The line of best fit with 95%
confidence bands are shown.

Figure 4: Plots of global 129Xe mean alveolar
dimension (LmD), acquired previously in Wild et al.2, with 129Xe TP (a) and RBC (b) T2*
value. A significant correlation between LmD and TP T2* values
suggests heterogeneity in the TP component is related to increased alveolar
dimensions.
DOI: https://doi.org/10.58530/2022/1169