1123
DTI-defined structural integrity metrics of the functionally-defined dentatothalamocortical pathway are related to disability
Jacqueline Chen1, Ajay Nemani1, Xuemei Huang1, Xin Li1, Kyle O'Laughlin1, Ela Plow1, Kenneth B Baker1, Mark J Lowe1, Stephen E Jones1, and Andre G Machado1
1Cleveland Clinic, Cleveland, OH, United States
1Cleveland Clinic, Cleveland, OH, United States
Synopsis
Prior to the implantation of brain stimulating electrodes, it would be valuable to have an estimation of the severity of pre-existing injury to the pathways of interest. In chronic stroke patients, we used resting-state functional MRI and transcranial magnetic stimulation (TMS) to identify functionally connected regions of the dentatothalamocortical pathway. We found that diffusion tensor imaging metrics of the tract connecting thalamus to the hand-motor hotspot were significantly correlated with hand function. These results suggest that this non-invasive functional/structural MRI/TMS approach can provide pathway-specific injury metrics that may be useful as part of a pre-surgical evaluation.
Introduction
Before considering implanting stimulation electrodes, it is useful to know the severity of existing injury to the pathways of interest. Our objective is to investigate a non-invasive method for measuring pathway-specific injury in chronic stroke patients who were candidates for stimulation of the dentatothalamocortical pathway. Resting-state functional MRI (rs-fMRI) and transcranial magnetic stimulation (TMS) were used to identify the functionally connected elements of the dentatothalamocortical pathway. Structural MRI and diffusion tensor imaging (DTI) metrics within the pathway were evaluated for significant correlation with hand function to identify metrics of pathway-specific injury.Methods
For 5 chronic stroke patients who were candidates for stimulation of the dentatothalamocortical pathway, baseline evaluations included upper-extremity Fugl-Meyer (UEFM) to measure upper-extremity function, TMS to identify the cortical location (“ipsilesional hand motor hotspot”) associated with electromyographic activity in the stroke-affected hand, and 7-tesla T1-weighted (T1w), DTI and rs-fMRI.T1w MRI was acquired using a 2 rapid acquisition variant with 208 0.75mm thick slices (TE=3ms; TR=6000ms; TI1=700ms; TI2=2700ms; FA1=4°; FA2=5°; FOV=192x192mm2; matrix=256x256; in-plane resolution=0.75x0.75mm2). Rs-fMRI were acquired while patients were awake and looking at a fixation cross, using a simultaneous multi-slice EPI with 81 contiguous 1.5mm thick axial slices (TE=21ms; TR=2800ms; FA=70°; anterior to posterior phase encode; FOV=192x192mm2; matrix=160x160; in-plane resolution=1.2x1.2mm2; multi-band factor=3; 128 volumes). High angular resolution diffusion imaging was acquired using a multi-slice EPI with 94 contiguous 1.3mm thick axial slices (TE=52.8ms; TR=11700ms; FA=180°; anterior to posterior phase encode; FOV=192x192mm2; matrix=148x148; in-plane resolution=1.3x1.3mm2; 8 b=0 volumes and 71 non-collinear diffusion-weighting gradients with b-value=1000s/mm2).
Rs-fMRI was used to define the functionally connected elements of the dentatothalamocortical pathway. Hand motor and thalamic regions of interest (ROIs) were defined using a previously published method,1 as the voxels with the highest correlation between the ipsilesional hand motor hotspot and ipsilesional thalamus. Based on the rs-fMRI z-map generated from using the thalamic ROI as a seed, the dentate ROI was defined as the contralesional dentate voxel with the highest correlation with the thalamic ROI. Figure 1 shows example ROIs.
DTI was used to define the structure of the dentatothalamocortical pathway and estimate tract integrity. Our probabilistic tractography method,2 incorporates both local and global information to improve accuracy, and specialized partial differential equation solvers for fast results. Tracking was performed independently for the two tract segments: from the dentate ROI to the thalamic ROI, and from the thalamic ROI to the hand motor ROI. The average fractional anisotropy (FA), transverse diffusivity (TD), mean diffusivity (MD) and longitudinal diffusivity were calculated independently for each tract segment and the total volume of the dentatothalamocortical pathway was estimated from the segmented tracts. Figure 1 shows example tracking.
T1w MRI was used to estimate the stroke volume and the percentage of lesion within the dentatothalamocortical pathway.
Statistical analyses calculated the individual correlations of UEFM-Hand with the DTI metrics, stroke volume within the tract and percentage of the tract containing stroke lesion.
Results
The patient demographics, baseline stroke volume and upper-extremity function scores are shown in the Table. Significant correlations with UEFM-Hand were found for: average FA (r=0.92, p=0.03), MD (r=-0.98, p=0.004) and TD (r=-0.97, p=0.007) of the tract segment from thalamic ROI to hand motor ROI (Fig. 2).Discussion
This analysis strives to assist in the choosing of ideal candidates for brain stimulation treatment. A candidate may not be ideal if the pathway to be stimulated has sustained substantial injury. For subject-specific accuracy, the dentatothalamocortical pathway was functionally defined using TMS and rs-fMRI. We show that in this bisynaptic pathway, only the structural integrity of the tract connecting the thalamus to the hand motor hotspot was significantly associated with hand disability. This supports and extends our earlier observations that anatomic connectivity as measured by transverse diffusivity is related to functional connectivity in monosynaptic pathways.3Conclusion
We used MRI and TMS to identify the functionally connected elements of the dentatothalamocortical pathway and found significant correlations between DTI metrics of the structural integrity of the tract connecting thalamus to the hand-motor hotspot with hand function. These findings suggest that this functional/structural MRI/TMS approach can provide pathway-specific injury metrics.Acknowledgements
This work was supported by the National Institutes of Health – [UH3-NS100543] and Enspire DBS Therapy, Inc.References
- Nemani A and Lowe MJ. Seed-based test-retest reliability of resting state functional magnetic resonance imaging at 3T and 7T. Med Phys. 2021 Oct;48(10):5756-5764.
- Zhang M, Sakaie KE, Jones SE. Logical foundations and fast implementation of probabilistic tractography. IEEE Trans Med Imaging. 2013 Aug;32(8):1397-1410.
- Lowe MJ, Koenig K, Beall EB, et al. Anatomic connectivity assessed using pathway radial diffusivity is related to functional connectivity in monosynaptic pathways. Brain Connect. 2014 Sep;4(7):558-565.
Figures
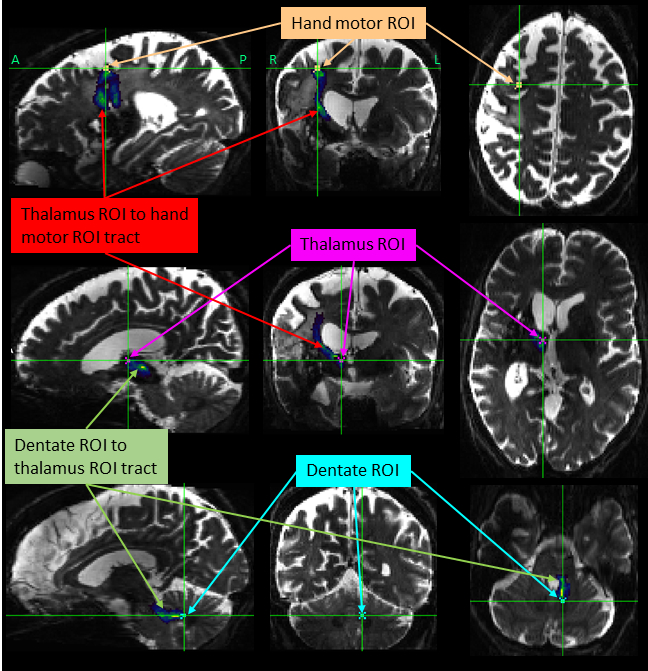
Figure 1:
The dentatothalamocortical pathway. MRI (b=0) from 58 year-old female, 11
months after stroke. Three functionally-defined ROIs of the
dentatothalamocortical pathway are shown with DTI-derived tracking.
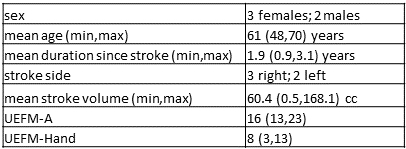
Table:
Patient demographics, baseline stroke volume and upper-extremity function.
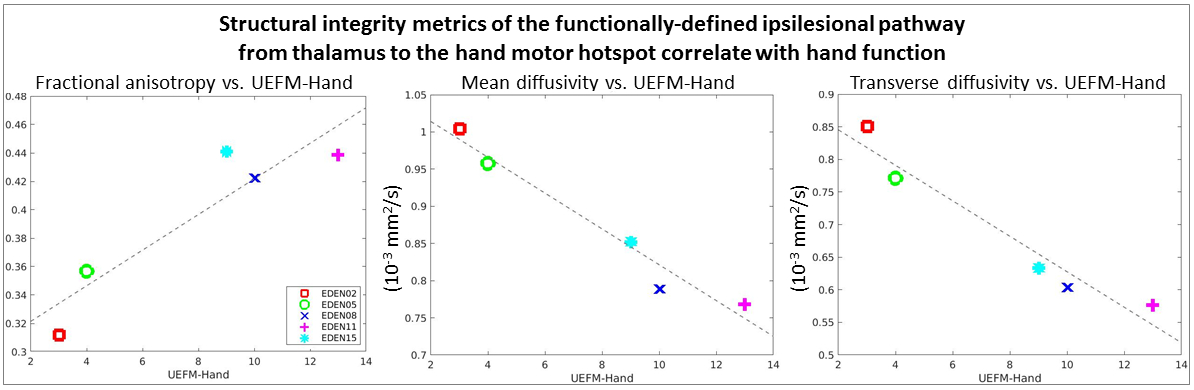
Figure 2: Statistically
significant correlations between DTI metrics of the structural integrity of the
tract connecting the thalamus ROI to the hand motor ROI with UEFM-Hand.
DOI: https://doi.org/10.58530/2022/1123