1040
Pulmonary imaging Using 3D Dual-Echo FID Ultra-short Echo Time MRI with Rosette k-space Pattern: Introduction and Feasibility.1School of Health Sciences, Purdue University, West Lafayette, IN, United States, 2Weldon School of Biomedical Engineering, Purdue University, West Lafayette, IN, United States, 3Radiology, Medical Center- University of Freiburg, Freiburg, Germany, 4Welcome Centre for Integrative Neuroimaging, University of Oxford, Oxford, United Kingdom
Synopsis
Pulmonary imaging traditionally uses techniques utilizing ionizing radiation such as x-rays and CT. Pediatrics, pregnant patients, and patients who will be exposed multiple times over long periods of time would benefit from a non-ionizing modality. MRI does not use ionizing radiation but suffers from low signal from the lungs and breathing motion artifact. We are proposing a novel MRI technique to combat these issues: a 3-dimensional Dual-Echo FID Ultra-short Echo Time (3D DE UTE) sequence utilizing Rosette k-space acquisition. Preliminary results demonstrated better pulmonary artery segmental branches and pleural wall definition compared to other commercially available MRI sequences.
Purpose
Pulmonary imaging has traditionally been performed using X-rays, Computed Tomography (CT), and Positron Emission Tomography PET (often fused with CT). All of these imaging techniques require and exposure to ionizing radiation. Magnetic Resonance Imaging (MRI) is an imaging technique that does not require ionizing radiation making it an ideal modality for pediatrics, pregnant patients, patients requiring multiple imaging studies over long periods of time, and patients looking for an alternative to ionizing radiation. However, MRI has often struggled with low signal in lung parenchyma and long acquisition times resulting in breathing motion artifacts. We propose a novel MRI technique: a 3D Dual-Echo FID Ultra-short Echo Time (3D DE UTE) sequence utilizing Rosette k-space acquisition patterns capable of mitigating these issues.Method
MR images were acquired on a 3T Magnetom Prisma (Siemens, Germany). Transverse and Coronal Volumetric Interpolated Breath-hold Examination (VIBE) T1 Weighted Images (WI) were acquired for comparison to the 3D DE UTE Sequence. Furthermore, non-breath-hold VIBE sequences were acquired using Long-Term Averaging to compare to the 3D DE UTE Sequence. VIBE is a Siemens T1 weighted gradient echo sequence commercially available on most systems and therefore serves as a good comparison. A 3D DE UTE sequence with rosette k-space sampling sequence was performed with parameters: field of view (FOV)=240×240×240mm, matrix size=120×120×120, readout dwell time=10 μs, flip angle=7-degree, TR=7 readout duration=2.1 ms, total acquisition duration without any acceleration= 4.2 minutes (TE1 = 20 us and TE2= 2 ms).Image reconstruction and post-processing steps for 3D DE UTE Sequence were performed in MATLAB (MathWorks, USA) platform. The non-uniform fast Fourier transform (NUFFT) was used to calculate the forward encoding transform of the acquired k-space data 11. A compressed sensing approach was used for image reconstruction, using total generalized variation (TGV) as the sparsifying penalty.
Results
Using the above sequences and methods, pulmonary imaging utilizing 3D DE UTE MRI was able to demonstrate better resolution while still maintaining good SNR compared to the VIBE sequence. 2D VIBE images at 2mm slice thickness (voxel size 1x1x2) demonstrated low SNR, resulting in mottling and poor visualization of pulmonary structures. Adjusting for low SNR by lowering the matrix size while maintaining a slice thickness of 2mm (voxel Size 2x2x2) resulted in more signal through the center of the image but lower resolution. Demonstration of the left and right Pulmonary arteries and their subsequent segmental branches were better visualized in 3D DE UTE while maintaining voxel size and slice thickness (Figure 1).Pleural linings were visualized in 3D DE UTE high- and low-resolution images for both echoes and poorly visualized in VIBE imaging (Figure 2). By utilizing dual echo imaging, the 3D DE UTE sequence is able to acquire both T2* and UTE-weighted images with one acquisition. UTE sequences have already shown to be a promising method for imaging Cystic Fibrosis, pulmonary nodules, parenchymal abnormalities, and ground glass opacities associated with COVID-19. 1,2 T2* WI and Gradient Echo imaging is useful for evaluation of iron deposition, microbleeds, and microdamage from osteoarthritis. 3 With the ability to collect both weightings and concurrently acquire 3-dimensional datasets, the potential reduction in overall examination time is far superior to the single T1 Weight 2-Dimensional VIBE.
Conclusion
3D DE UTE sequences are promising for time efficient and non-ionizing imaging of the pulmonary structures and surrounding tissues. Segmental branches of the pulmonary arteriovenous system are often sub mm thickness. Therefore, good SNR and high resolution is imperative in MR imaging of said structures, which this sequence can achieve. By implementing a dual echo acquisition, UTE and T2* gradient echo images are acquired during a single scan. 3-dimensional data acquisition reduces the total acquisition time required for volumetric imaging with isotropic resolution. Further reduction in breathing motion can be achieved by using respiratory gating and post-processed propagation.Acknowledgements
Data acquisition was supported in part by NIH grant S10 OD012336- 3T MRI Scanner dedicated to Life Sciences Research.
References
1. Hiroto Hatabu, MD, PhD, Yoshiharu Ohno, MD, PhD, Warren B. Gefter, MD, Grace Parraga, PhD, Bruno Madore, PhD, Kyung Soo Lee, MD, PhD, Talissa A. Altes, MD, David A. Lynch, MB, BCh, John R. Mayo, MD, Joon Beom Seo, MD, PhD, Jim M. Wild, PhD, Edwin J. R. van Beek, MD, PhD, Mark L. Schiebler, MD, Hans-Ulrich Kauczor, MD. Expanding Applications of Pulmonary MRI in the Clinical Evaluation of Lung Disorders: Fleischner Society Position Paper, 2020.
2. Shuyi Yang PhD, MD, Yunfei Zhang PhD, Jie Shen B.S., Yongming Dai PhD, Yun Ling MD, Hongzhou Lu PhD, MD, Rengyin Zhang B.S., Xueting Ding B.S., Huali Qi B.S., Yuxin Shi PhD, MD, Zhiyong Zhang PhD, MD, and Fei Shan PhD, MD. Clinical Potential of UTE-MRI for AssessingCOVID-19: Patient- and Lesion-BasedComparative Analysis. J Magn Reason. Imaging 2020.
3. Meng Yue Tang, Tian Wu Chen, Xiao Ming Zhang, and Xiao Hua Huang. GRE T2∗-Weighted MRI: Principles and Clinical Applications. Sichuan Key Laboratory of Medical Imaging, Department of Radiology, Affiliated Hospital of North Sichuan Medical College, Nanchong, Sichuan 637000, China, 2014.
Figures
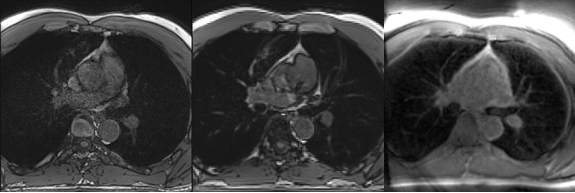
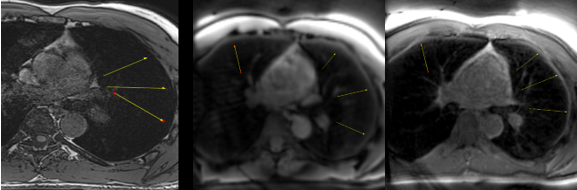
Non-breath holding VIBE (Left) and 3D DE UTE sequences (T2* Weighted Middle (TE2=2ms and UTE (TE1 =20 us) Right). Pleural lining is well visualized on the 3D DE UTE Sequence and poorly visualized on the VIBE.