0919
Rapid and High Resolution Pelvic MRI Using Deep Learning Reconstruction1Radiology, Fairfax Radiological Consultants, Arlington, VA, United States, 2GE Healthcare, Boston, MA, United States, 3GE Healthcare, Lynchburg, VA, United States, 4Fairfax Radiological Consultants, Fairfax, VA, United States, 5GE Healthcare, Waukesha, WI, United States, 6GE Healthcare, Houston, TX, United States
Synopsis
MRI plays an important role in pelvic assessment. For instance, it is the modality of choice for rectal cancer staging, gynecologic cancer staging, uterine fibroid evaluation and ovarian tumor characterization. Due to the complex nature of the anatomy and clinical demands of these protocols, high resolution thin slice volumetric scans are desired but low SNR, prolonged scan times and motion artifacts remain problematic. In this work, we deploy a combination of recent technical advances in particular high density flexible coils, compressed sensing, and deep learning reconstruction to tackle these challenges and report our feasibility results.
Introduction
Pelvic area cancers such as in urogenital system remain a leading cause of cancer related morbidity and mortality [1]. In addition, MRI is deemed mandatory and preferred choice for both primary staging and restaging of rectal cancer, with the exception of staging for early tumors [2-3]. MRI evaluation is also modality of choice for characterization of uterine and ovarian masses including preoperative imaging prior to procedures such as uterine fibroid embolization. Given MR’s already prominent role in pelvic assessment, we set to explore the potential benefits of novel deep learning based reconstruction in combination with high density flexible coils and compressed sensing. Our clinical feasibility results are summarized in this work.Methods
3T Signa Premier scanner (GE Healthcare, WI) equipped with 30ch AIR Anterior Array and 60ch AIR Posterior Array was used for imaging. 2D acquisitions of the protocol were reconstructed online using commercially available AIR Recon DL deep learning reconstruction [4-5]. 3D scans utilized commercially available 2D ARC [6] parallel imaging and HyperSense [7] compressed sensing for speed up. 3D datasets are reconstructed twice: first with the commercially available conventional reconstruction then followed by an offline reconstruction with a prototype AIR Recon DL 3D module [4]. 2D T2w contrast images have 0.4x0.5x3.0 mm resolution with 0 gap and scan time varies with the coverage. A typical coverage of 42 slices took 218 seconds to acquire and 3D post-contrast LAVA T1w scans were 0.8x1.2x1.2 mm3 acquisitions with sub-millimeter voxel reconstructions in 17 to 19 seconds depending on the coverage. A board-certified radiologist provided qualitative assessment of the image quality. Since the conventional reconstruction and deep learning reconstruction results look significantly different, radiologist was not blinded to the reconstruction type.Results
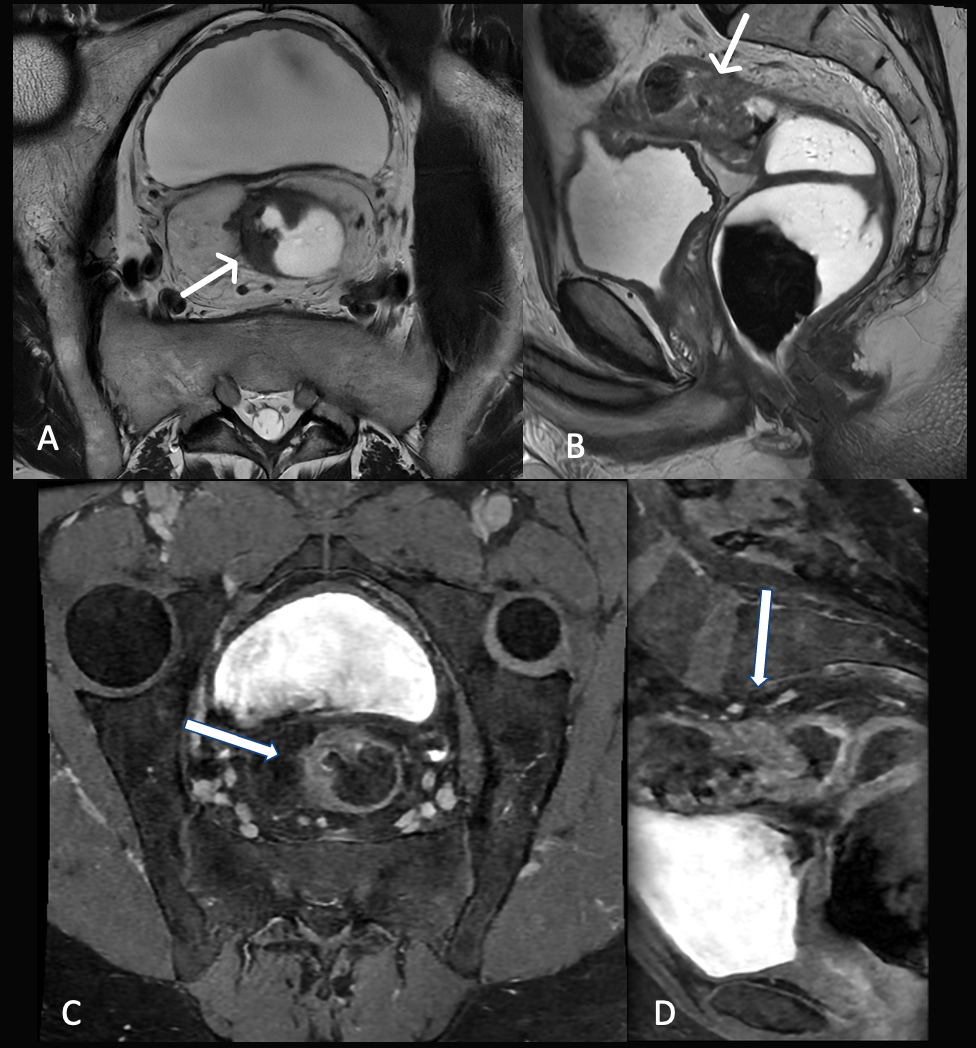
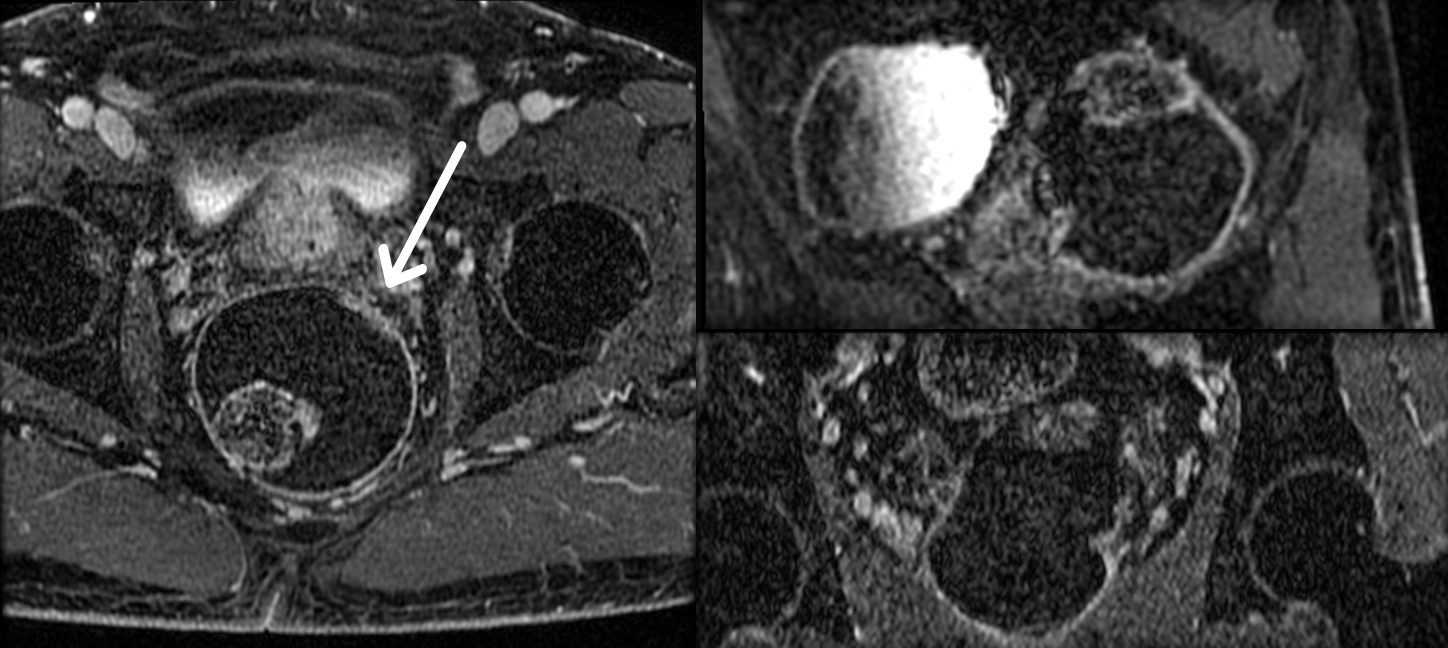
Figure 1 demonstrates a rectal staging examination with T3b rectal mass along the right anterior and lateral aspect of the high rectum at the level of the rectosigmoid junction. T2w images in Figures 1A and 1B are reconstructed with AIR Recon DL and demonstrates excellent image quality while subtle blurring due to motion. On the other hand, 3D post-contrast Axial T1w scan AIR Recon DL in Figure 1C and Sagittal reconstruction in 1D show blurry images due to motion artifacts (readout anterior/posterior direction) arising from free breathing 90 second scan time.Figure 2 demonstrates that faster breath-held scan with readout right/left direction is feasible and results in sharper images but due to high resolution and aggressive acceleration factors images suffer from low SNR with conventional reconstruction. The subtle rectal tumor is visible along the left anterolateral 1’oclock position (arrow).
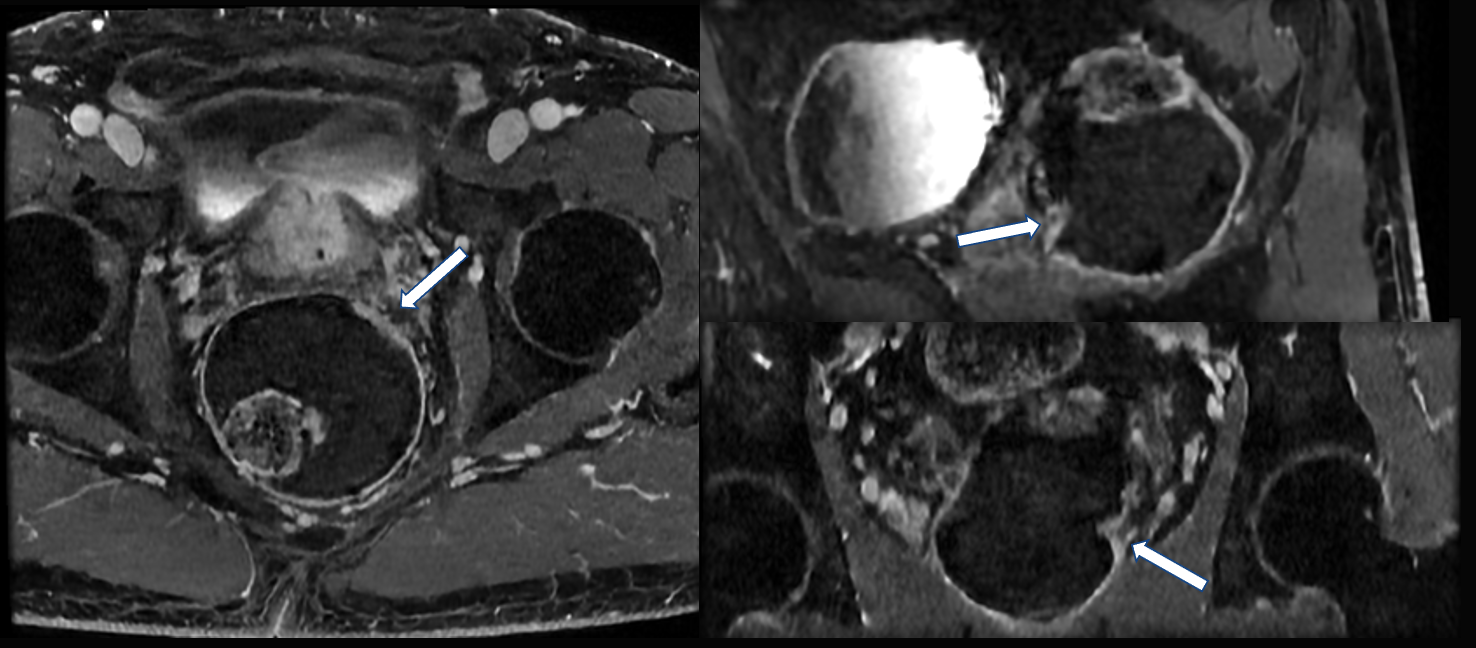
Figure 3 captures the AIR Recon DL reconstruction of the same post contrast Volumetric T1w scan that was shown in Figure 2 for the same slice as well as reformat locations. Markedly improved SNR is obtained with the help of deep learning reconstruction despite a very rapid scan time of 19 seconds for 0.8x1.2x1.2 mm3 acquired voxel resolution and sub-millimeter resolution reconstructions. High in-plane resolution and thin slices affords high quality reformats. The improved SNR allows for better visualization of the T2 rectal cancer along the anterior and lateral rectum.
Figure 4 and 5 represent a female patient sent for evaluation of a cervical mass. Figure 4 utilizes conventional image reconstruction of the post contrast Volumetric T1 scan demonstrating SNR staved axial images and poor-quality coronal and sagittal reformats limiting evaluation of the endocervical mass.
Figure 5 demonstrates AIR Recon DL reconstruction of the same post contrast Volumetric T1w scan with excellent image quality. Again, excellent SNR and high quality reformats are achieved in a 17 second scan time with 0.8x1.2x1.2 mm3 acquired voxel resolution and sub-millimeter resolution reconstructions.
Discussion
High resolution pelvic imaging requires a combination of pre and post contrast imaging for adequate diagnosis. While 2D sequences provide excellent image quality with occasional slice blurring due to motion, 3D scans suffer adversely from motion artifacts contaminating the entire volume. Since the AIR Recon DL is geared towards SNR improvement and truncation artifact removal, motion artifacts could become more visible when noise is removed. We circumvent this problem with 3D post-contrast T1w scans by creating a highly accelerated high resolution scan that can be done in under a 20 second breath hold. One limitation of this study is a small sample size. Further data collection is warranted with different indications for high resolution pelvic imaging, which we plan to do.Acknowledgements
No acknowledgement found.References
1. Ferlay J, Ervik M, Lam F, Colombet M, Mery L, Piñeros M, et al. Global Cancer Observatory: Cancer Today. Lyon: International Agency for Research on Cancer; 2020 (https://gco.iarc.fr/today, accessed November 2021).
2. MERCURY Study Group. Diagnostic accuracy of preoperative magnetic resonance imaging in predicting curative resection of rectal cancer: prospective observational study. Bmj. 2006 Oct 12;333(7572):779.
3. Beets-Tan RGH, Lambregts DMJ, Maas M, Bipat S, Barbaro B, Curvo-Semedo L, Fenlon HM, Gollub MJ, Gourtsoyianni S, Halligan S, Hoeffel C, Kim SH, Laghi A, Maier A, Rafaelsen SR, Stoker J, Taylor SA, Torkzad MR, Blomqvist L. Magnetic resonance imaging for clinical management of rectal cancer: Updated recommendations from the 2016 European Society of Gastrointestinal and Abdominal Radiology (ESGAR) consensus meeting. Eur Radiol. 2018 Apr;28(4):1465-1475. doi: 10.1007/s00330-017-5026-2.
4. Lebel RM. Performance characterization of a novel deep learning-based MR image reconstruction pipeline. arXiv preprint arXiv:2008.06559. 2020 Aug 14.
5. Wang X, Ma J, Bhosale P, Rovira JJ, Qayyum A, Sun J, Bayram E, Szklaruk J. Novel deep learning-based noise reduction technique for prostate magnetic resonance imaging. Abdominal Radiology. 2021 Jul;46(7):3378-86.
6. Beatty P, Brau A, Chang S, et al. A method for autocalibrating 2-D accelerated volumetric parallel imaging with clinically practical reconstruction times. In: Proc 15th Annual Meeting ISMRM, Berlin; 2007. p 1749.
7. King K, Xu D, Brau A, Lai P, Beatty P, Marinelli L. A new combination of compressed sensing and data driven parallel imaging. In: Proc 18th Annual Meeting ISMRM, Stockholm; 2010. p 4881
Figures