0819
Impact of motion correction on in-vivo assessment of Placenta Adhesion Abnormality (PAA) disorders using IVIM method1IADI, Inserm U1254, Université de Lorraine, Nancy, France, 2CIC-IT 1433, Inserm, CHRU Nancy, Nancy, France, 3Siemens Healthineers, Nancy, France, 4MR Applications Predevelopment, Siemens Healthcare GmbH, Erlangen, Germany, 5Women's Division, Nancy Regional and University Hospital Center (CHRU), Université de Lorraine, Nancy, France, Nancy, France
Synopsis
Placenta adhesion abnormality (PAA) is the consequence of an excessive invasion of the placenta within the myometrium. Due to its severe maternal pregnancy outcomes, screening of subjects with suspicions of PAA are very important. The utilisation of intra voxel incoherent motion (IVIM) technique may help to improve the diagnosis. But its stability and robustness need to be improved and analysed. Here we aim to evaluate the impact and address the importance of motion correction technique to assess PAA disorders in-vivo using IVIM method in order to establish a robust and stable pipeline for PAA patient screening.
Introduction
Placenta adhesion abnormalities (PAA) are the consequence of an excessive invasion of the placenta within the myometrium. PAA is related to severe maternal pregnancy outcomes, especially in cases of incidental discovery during delivery that increases the risk of intraoperative massive bleeding, hysterectomy, and even maternal death. Ultrasound is the standard modality for diagnosing PAA, but Magnetic Resonance Imaging (MRI) has been increasingly performed in the case of inconclusive sonographic findings [1]. The Intravoxel Incoherent Motion (IVIM) imaging method introduced in [2] has been shown with great potential in placenta abnormalities such as IUGR [1] but has not been much addressed explored in the case of PAA. The clinical use of the IVIM imaging method in obstetrics is still limited due to many confounding factors among which the presence of maternal and fetal motion is one of the most disturbing. These motions are unpredictable and can potentially downgrade the model fitting results, therefore affecting the final use of the IVIM parameters in terms of differentiating between the physiological group and PAA group. In this work, we present our preliminary results on assessing the impact of the motion correction technique on IVIM model parameters extraction in a dedicated cohort of placenta adhesion abnormality patients.Materials and Methods
Protocol: 9 patients (gestational age between 30-38 weeks, 35+/-6.4 years old) were currently recruited under the ongoing clinical study DIANE (NCT04328532, ethic approval received). Among the 9 patients, 5 are diagnosed with PAA and 4 are normal (control group).Imaging: The patients were all scanned with a 3T clinical scanner (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany) between October 2020 and September 2021 with a finely tuned MRI protocol. A 18 channel body coil and a 32 channel spine matrix were used for signal reception. The overall acquisition time was 30 minutes, and a dedicated prototype DWI sequence from Siemens was used to extract IVIM parameters (f, the fractional perfusion related to microcirculation, D the true diffusion coefficient and D* the pseudo diffusion coefficient)[2,3]. Relevant IVIM imaging settings are TR/TE 6000ms/60ms, and voxel resolution 1.56 x 1.56x 5mm, acquisition matrix 128x128 and FoV around 430 mm varying between patients. Overall, 11 b values (0, 15, 45, 80, 115, 205, 245, 345, 470, 700, 1000 s/mm2) are chosen. Different averaging strategies were used in order to balance the SNR which may impact images in particular for high b values. Only monopolar diffusion gradients are used for the consideration of SNR, SAR and time. No acceleration options are used in this case. IVIM sequences were scanned in three orthogonal directions.
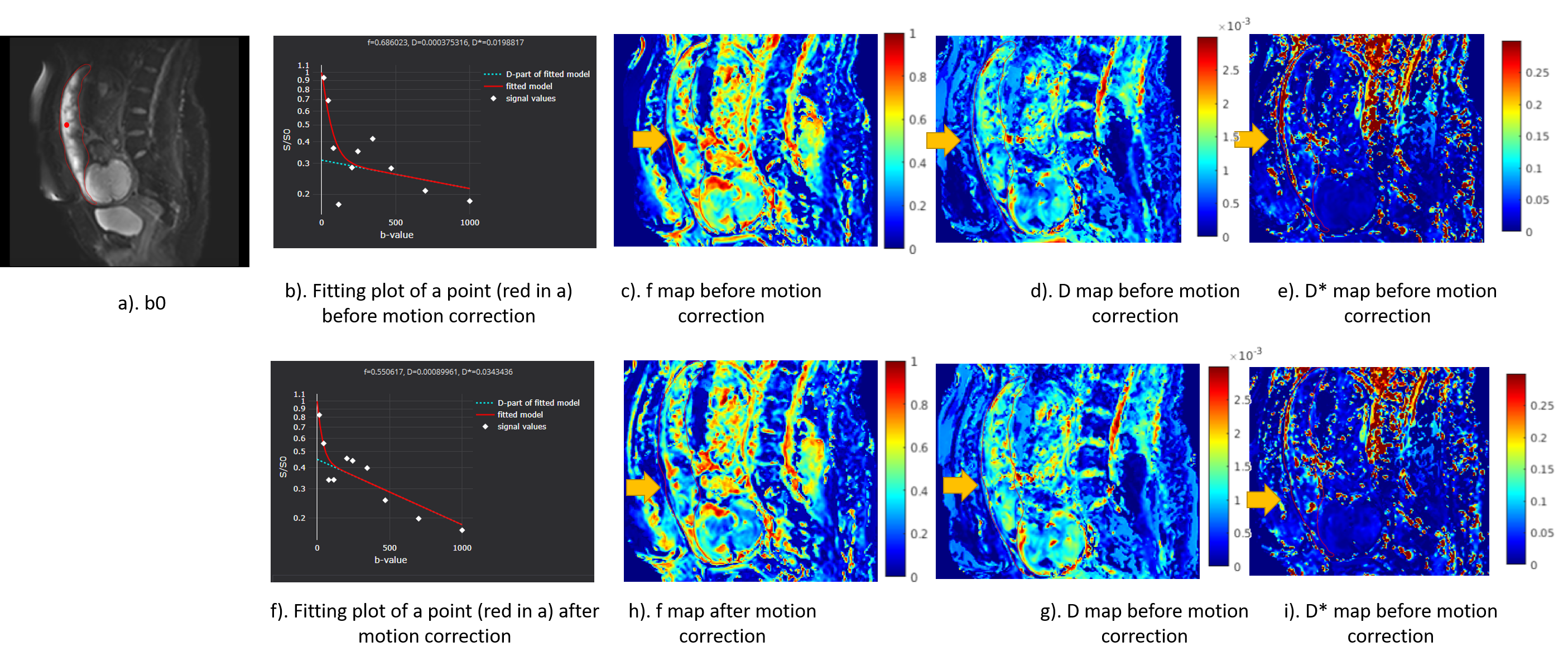
Image processing and data analysis: Motion correction was performed within the scanner integrated image reconstruction of the employed prototype. The algorithm consists of two parts: motion correction between averages of single images and motion correction between b-values with the averaged images. The similarity measures are local cross correlation and mutual information respectively. Both motion-corrected images and non-motion-corrected IVIM images were analyzed with the IVIM module in MITK-DIFFUSION software [5], using a joint mapping of f, D and D*. 3D placenta ROIs were manually drawn on all the subjects for a ROI based analysis. Parametric maps were visually compared and fitting curves were obtained for every subject. Mean values of f, D and D* were compared between control.
Results
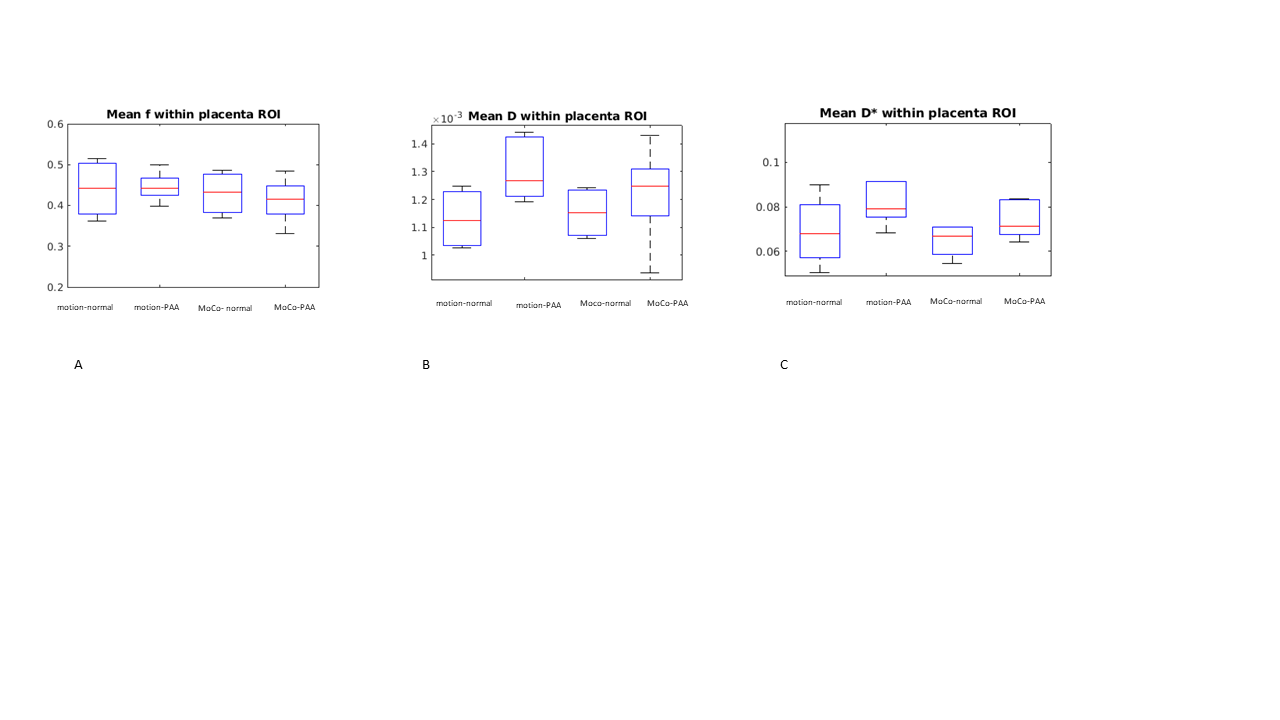
Parametric maps generated by images without/with motion correction are illustrated in Figure 1. Comparison of average f, D and D* values within the placenta ROIs between the control and PAA groups were shown in Figure 2 using box plots. Although differences between the two groups exist, due to the current small number of either group no statistical conclusion can be drawn. It is also interesting to notice that the degree of dispersion were reduced in the box plots of all the three parameters extracted from the control group after applying motion correction as compared to those before applying motion correction (Figure 2). While in the PAA group, no such trends were discovered.Discussion and Conclusion
We have illustrated in this preliminary work that motion correction can impact the IVIM model fitting and related quantitative parameter extraction. The difference of parameters between the control and PAA groups exists. However, due to the current small number of patients, it is difficult to conclude to what extent motion correction can improve the characterization between the groups. The different trends of box plot dispersion change between the control and PAA groups before and after motion correction applied may be relevant to the fact that the placentas in PAA are structurally heterogeneous due to the placenta's local invasion into the myometrium, whereas normal placentas tend to be homogeneous globally.The protocol DIANE plans to recruit more patients and it would be clearer at the end of the study to assess more comprehensively the method. It also has to be pointed out that motion correction is not the only factor that affects the characterisation of PAA using IVIM, other factors such fitting methods would also be considered in the future work.
Acknowledgements
No acknowledgement found.References
[1] Srinivasan V, Melbourne A, Oyston C, James JL, Clark AR: Multiscale and multimodal imaging of utero-placental anatomy and function in pregnancy. Placenta 2021; 112:111–122. *
[2] Le Bihan D, Breton E, Lallemand D, Grenier P, Cabanis E, Laval-Jeantet M: MR imaging of intravoxel incoherent motions: application to diffusion and perfusion in neurologic disorders. Radiology 1986;161:401– 407.
[3] Shi H, Quan X, Liang W, Li X, Ai B, Liu H. Evaluation of Placental Perfusion Based on Intravoxel Incoherent Motion Diffusion Weighted Imaging (IVIM-DWI) and Its Predictive Value for Late-Onset Fetal Growth Restriction. Geburtshilfe Frauenheilkd [Internet]. 2019 [cited 2021 Nov 10];79(4):396. Available from: /pmc/articles/PMC6461467/
[4] MITK diffusion https://github.com/MIC-DKFZ/MITK-Diffusion/
[5] Jolly MP, Guetter C, Guehring J: Cardiac segmentation in MR cine data using inverse consistent deformable registration. 2010 7th IEEE Int Symp Biomed Imaging From Nano to Macro, ISBI 2010 - Proc 2010:484–487.
Figures