0733
Abnormal Brain Activation in Post-acute Sequelae of COVID-191Diagnostic Radiology and Nuclear Medicine, University of Maryland School of Medicine, Baltimore, MD, United States, 2Neurology, Johns Hopkins University School of Medicine, Baltimore, MD, United States, 3Neurology, University of Maryland School of Medicine, Baltimore, MD, United States, 4Program in Neuroscience, University of Maryland School of Medicine, Baltimore, MD, United States, 5Medicine, Division of Infectious Disease, University of Maryland School of Medicine, Baltimore, MD, United States, 6Medicine, Critical Care Medicine, University of Maryland School of Medicine, Baltimore, MD, United States
Synopsis
Post-acute sequelae of COVID-19 is highly prevalent after the acute infection. Neuropsychiatric symptoms are particularly common; however, the pathophysiology of how the brain is affected remains unclear. This study aimed to evaluate whether convalescent COVID-19 participants have abnormal brain activation that is related to quantitative neurobehavioral measures. 21 COVID-19 participants and 20 healthy controls were evaluated with the NIH-Toolbox® and blood-oxygenation level dependent-functional MRI (BOLD-fMRI), using the N-back tasks. Despite similar performance on the NIH-Toolbox-cognitive battery, COVID-19 participants had greater brain activation than controls in the precuneus and dorsal anterior cingulate cortex, which also predicted poorer dexterity, endurance, and locomotion.
Introduction
Post-acute sequelae of COVID-19 (PASC) are highly prevalent (~30-80%) among COVID-19 survivors, especially in those with more severe illness, and may last for one year or longer after the acute infection.1-3 Neuropsychiatric symptoms are particularly common, including fatigue, the inability to concentrate or “brain fog”, headaches, loss or change of smell and/or taste sensations, sleep disorders, anxiety, and depression.2,4 The pathophysiology or mechanisms underlying these persistent symptoms remain unclear. The goal of this study is to evaluate whether convalescent COVID-19 participants have abnormal brain activation and deficits on quantitative neurobehavioral measures. We hypothesized that on blood-oxygenation level dependent (BOLD)-functional MRI (fMRI), convalescent COVID-19 participants will have greater brain activation (i.e., greater usage of brain reserve) than uninfected controls due to residual brain injury and past or ongoing peripheral or brain immune activation, and that greater brain activation will normalize with longer duration of convalescence. Furthermore, COVID-19 participants with greater brain activation were expected to have poorer behavioral measures.Methods
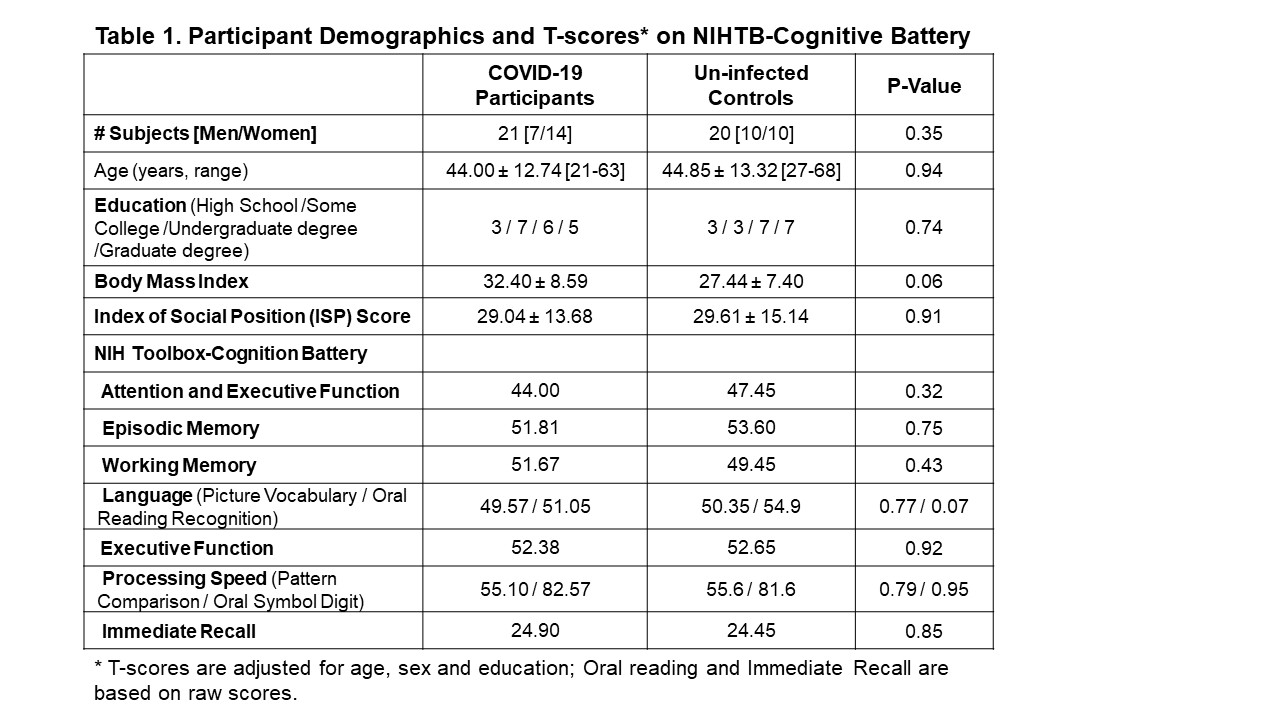
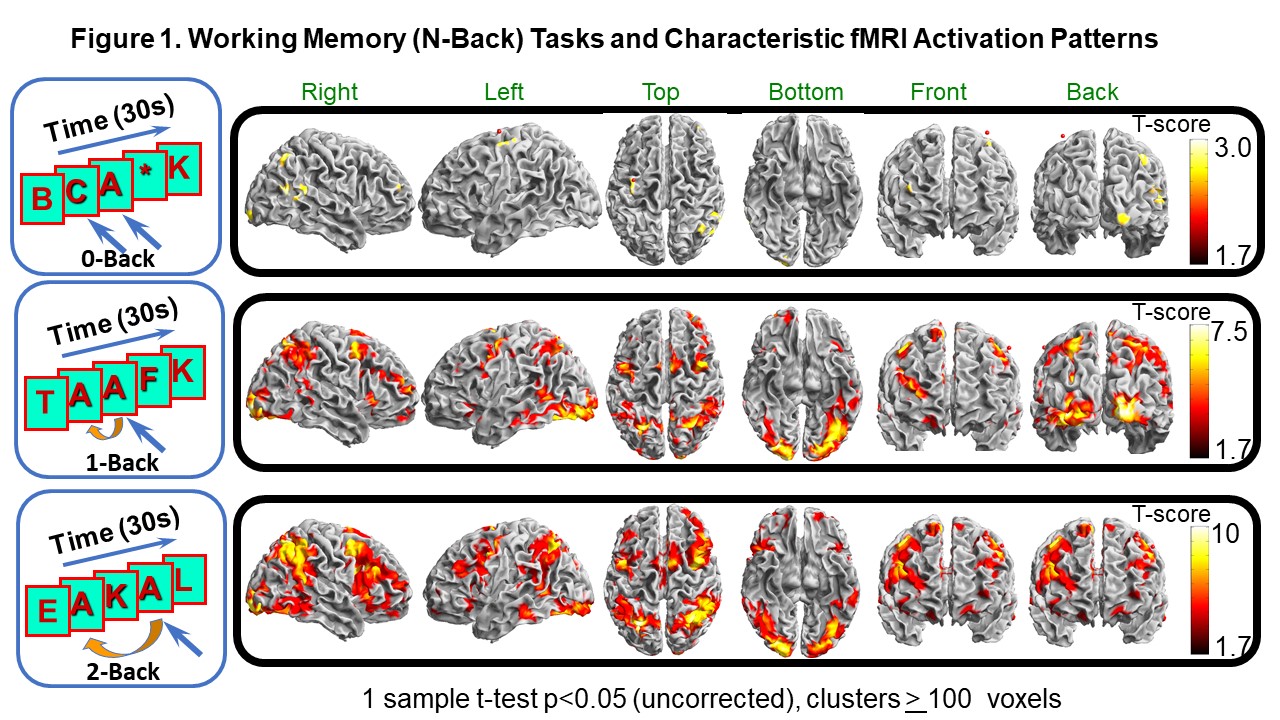
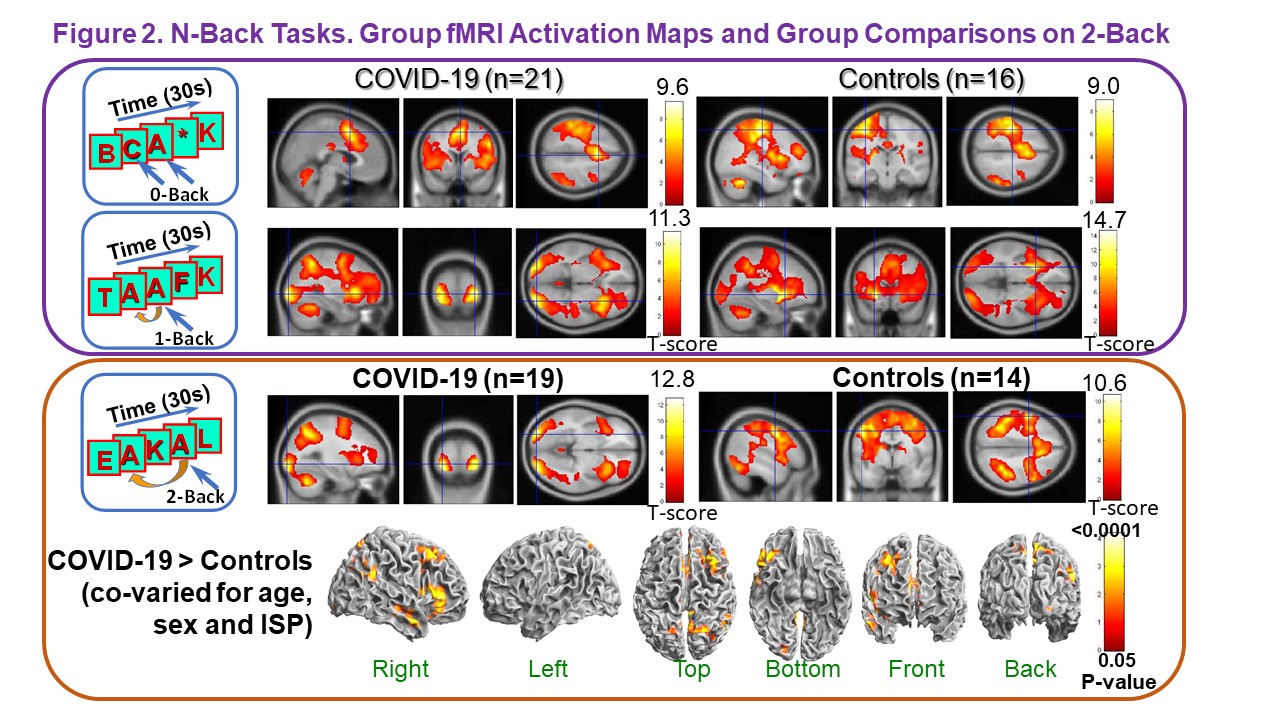
21 patients diagnosed with COVID-19 and 20 healthy uninfected healthy controls were evaluated with the NIH-Toolbox® (NIHTB), including the Cognition Battery (CB),5-7 Emotional Battery (EB)8 and Motor Battery (MB).9 Each participant performed three N-back working memory tasks (0-back, 1-back, 2-back) during a BOLD-fMRI scan on a 3T MR Scanner (Siemens Prisma scanner); see Figure 1. Single-shot gradient-echo echo-planar MRI (TE/TR=30/3000ms, ~42 axial 3-mm slices, 3-mm resolution, 80 NEX) was performed with real-time motion correction. Data were processed using SPM12.10 Only fMRI data with <1.5mm translations and <1.5º rotations, and 75% performance accuracy during the N-back tasks were included in the final analyses (See Figure 2). Analyses of co-variance were used to compared group differences on behavioral and fMRI measures, covarying for age, sex and education or index of social position (ISP).Results
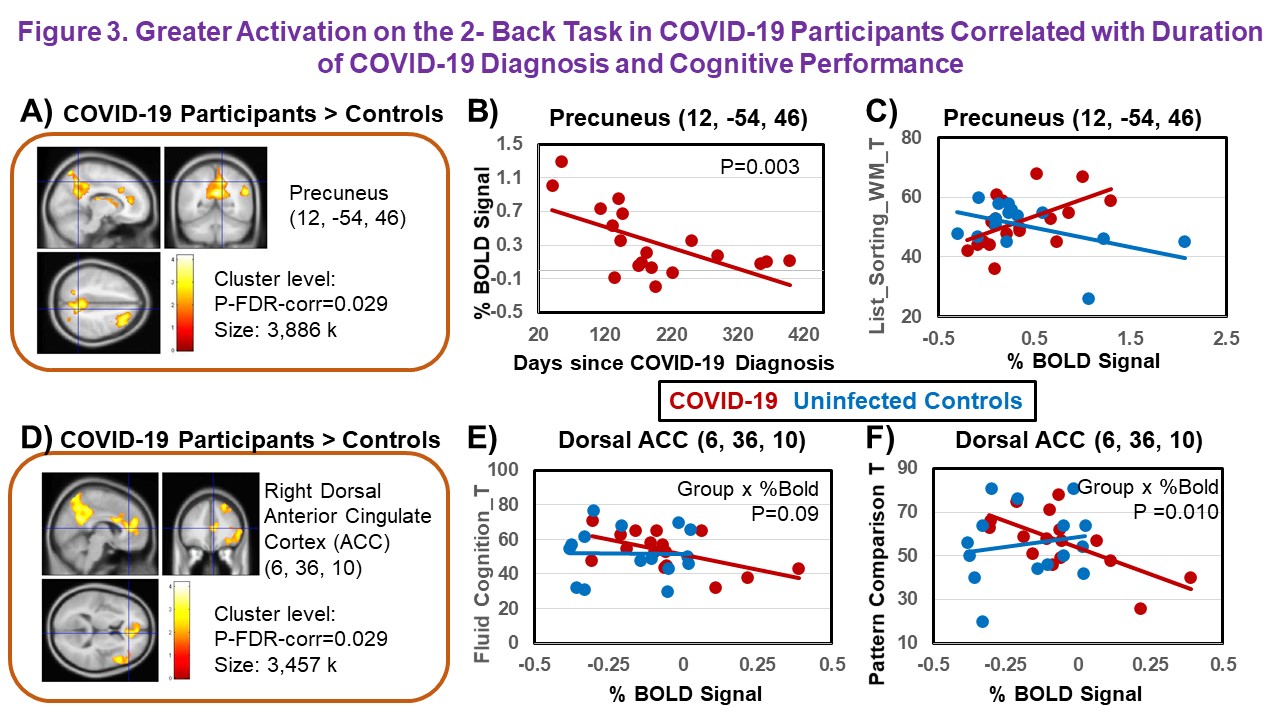
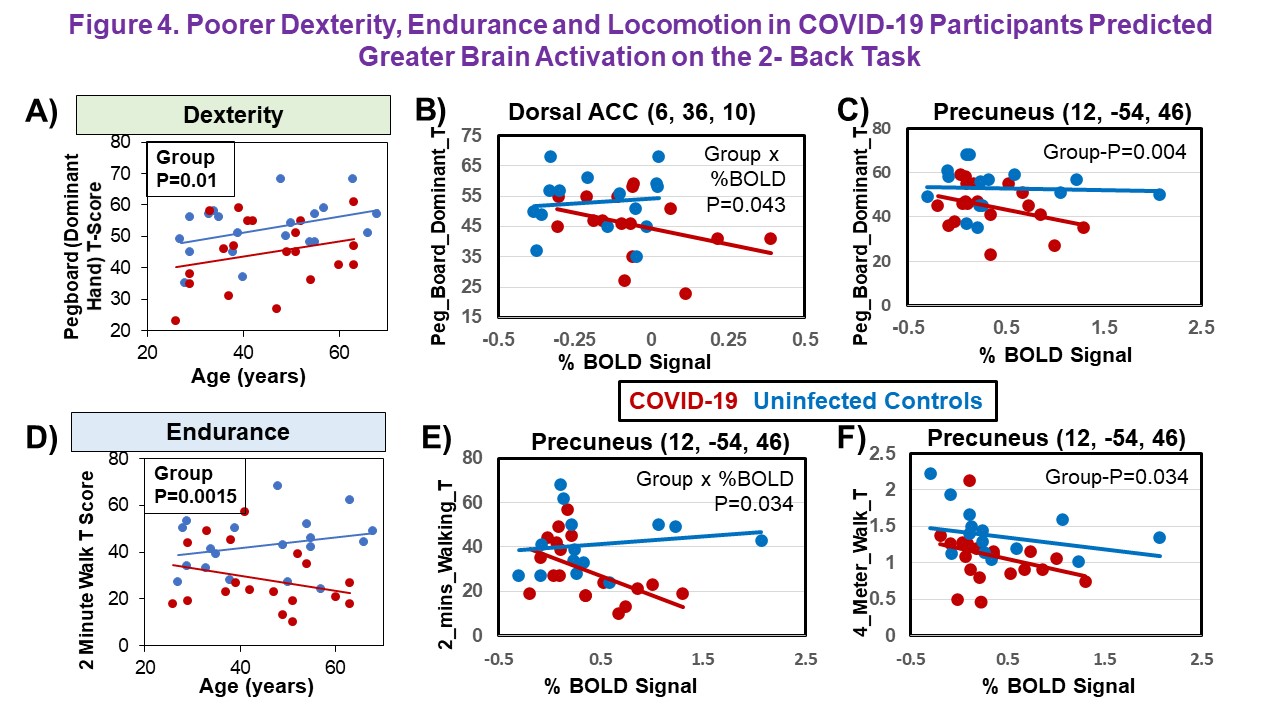
COVID-19 participants (duration of diagnosis 186±98 days) had similar age, sex-proportion, education, and ISP as healthy uninfected controls (Table 1). However, COVID-19 participants tended to have higher body mass indices (p=0.055). Although COVID-19 participants reported high prevalence of cognitive complaints [memory (90%) and concentration (90%) problems, fatigue (90%), confusion (80%)], they performed similarly to controls on the NIH Toolbox-CB on all seven target domains (Table 1).In contrast, on BOLD-fMRI, while COVID-19 participants and controls showed no group differences on brain activation during the 0-back and 1-back tasks (Figure 2, top panel), COVID-19 participants had greater brain activation in right prefrontal (dorsal and inferior regions), posterior parietal and occipital regions on the 2-back task (Figure 2, bottom panel). Furthermore, activation in the precuneus on the 2-back task was greater in COVID-19 participants than controls (FDR-corrected-p=0.029, Figure 3A), and correlated with days since COVID-19 diagnosis (Figure 3B) and with disease severity during the acute phase of the illness (p=0.0035, data not shown). Although COVID-19 subjects had normal performance on NIHTB-CB, those with greater BOLD signals in precuneus on the 2-back task performed better on the List-Sort Working Memory task (Figure 3C). In contrast, greater brain activation in the dorsal anterior cingulate cortex (ACC) of COVID-19 participants than controls (Figure 3D) correlated with poorer performance on Fluid Cognition and Pattern Comparison (Figures 3 E-F). On the NIHTB-MB, COVID-19 participants had poorer dexterity than controls across the age spectrum (Pegboard dominant hand, p=0.01, Figure 4A), which was predicted by the greater brain activation (Figures 4B-C). COVID-19 participants also had poorer endurance (2-Minute Walk, group-p=0.0015), especially in the older participants, and slower locomotion (4-Meter Walk, group-p=0.034) than the uninfected controls; these measures were also predicted by greater brain activation in the precuneus (Figures 4E-F).
Discussion
A high proportion (~60%) of COVID-19 survivors develop either incident or persistent symptoms, including fatigue, “brain fog”, concentration problems, anxiety, depression and other neuropsychiatric symptoms within 6 months.3 The pathophysiology or mechanism(s) for PASC remain unclear, but may result from residual or ongoing brain injury from micro-thrombotic events, autoimmune dysregulation, or microglial activation without chronic neuroinflammation, as observed in some postmortem neuropathological studies.11,12 Surprisingly, despite the high prevalence (80-90%) of subjective complaints for concentration and memory problems, our COVID-19 participants had normal performance on the NIH-CB. However, BOLD-fMRI demonstrated reorganized brain activation patterns that primarily reflect greater attentional modulation in two major nodes within the working memory network, the precuneus and the dorsal ACC, as well as several other brain regions within or adjacent to the working memory network, suggesting usage of the brain reserve. These altered brain activation patterns were only observed on the more difficult task (2-back), demonstrating that the parametric design with increasing cognitive load is useful for detecting subclinical brain abnormalities in participants with PASC. Longitudinal evaluations are needed to assess whether the altered brain activation pattern will normalize. Future and ongoing evaluations will assess the relationships between brain activation, immune markers in the peripheral and in the cerebrospinal fluid, as well as with quantitative psychiatric symptoms on the NIHTB-EB.Conclusions
Altered brain activation persist even 6 months after recovery from COVID-19. BOLD-fMRI is a sensitive and objective measure to evaluate PASC since it can detect subclinical abnormalities in the brain. A parametric design with increasing cognitive load is needed to detect these brain abnormalities (i.e., brain stress test).Acknowledgements
This work was supported by a grant from NIH (R21NS121615). We also thank our research participants for their participation.References
1. Carfi A, Bernabei R, Landi F, Gemelli Against C-P-ACSG. Persistent Symptoms in Patients After Acute COVID-19. JAMA. 2020;324(6):603-605.
2. Proal AD, VanElzakker MB. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front Microbiol. 2021;12:698169.
3. Taquet M, Dercon Q, Luciano S, Geddes JR, Husain M, Harrison PJ. Incidence, co-occurrence, and evolution of long-COVID features: A 6-month retrospective cohort study of 273,618 survivors of COVID-19. PLoS Med. 2021;18(9):e1003773.
4. Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More Than 50 Long-Term Effects of COVID-19: A Systematic Review and Meta-Analysis. Res Sq. 2021.
5. Weintraub S, Dikmen SS, Heaton RK, et al. Cognition assessment using the NIH Toolbox. Neurology. 2013;80(11 Suppl 3):S54-64.
6. Weintraub S, Dikmen SS, Heaton RK, et al. The cognition battery of the NIH toolbox for assessment of neurological and behavioral function: validation in an adult sample. J Int Neuropsychol Soc. 2014;20(6):567-578.
7. Akshoomoff N, Beaumont JL, Bauer PJ, et al. VIII. NIH Toolbox Cognition Battery (CB): composite scores of crystallized, fluid, and overall cognition. Monogr Soc Res Child Dev. 2013;78(4):119-132.
8. Babakhanyan I, McKenna BS, Casaletto KB, Nowinski CJ, Heaton RK. National Institutes of Health Toolbox Emotion Battery for English- and Spanish-speaking adults: normative data and factor-based summary scores. Patient Relat Outcome Meas. 2018;9:115-127.
9. Reuben DB, Magasi S, McCreath HE, et al. Motor assessment using the NIH Toolbox. Neurology. 2013;80(11 Suppl 3):S65-75.
10. 12 S. 2012; https://www.fil.ion.ucl.ac.uk/spm/software/spm12/.
11. Matschke J, Lutgehetmann M, Hagel C, et al. Neuropathology of patients with COVID-19 in Germany: a post-mortem case series. Lancet Neurol. 2020;19(11):919-929.
12. Schwabenland M, Salie H, Tanevski J, et al. Deep spatial profiling of human COVID-19 brains reveals neuroinflammation with distinct microanatomical microglia-T-cell interactions. Immunity. 2021;54(7):1594-1610 e1511.
Figures