0540
Normative Baseline Analysis of Carpal Bone Kinematic Profiles Using 4D MRI1Radiology, Medical College of Wisconsin, Milwaukee, WI, United States
Synopsis
4D-dynamic MRI were collected and utilized to track unconstrained movement of individual wrist carpal bones in 31 asymptomatic volunteer subjects. Rotational and translational trajectories of the scaphoid, lunate, and capitate bones were collected and processed using a novel multi-subject profile registration and analysis engine. Morphological images were analyzed by an expert radiologist to identify asymptomatic abnormalities within the cohort. Statistical parametric mapping of each profile was performed to identify normative variances of each profile metric and correlation with identified abnormalities. The study presents methodological approaches and normative baseline profile metrics of value to future studies of symptomatic wrists.
Introduction
Dynamic imaging of moving joints offers new and substantially useful information to assessments of orthopaedic injuries and degeneration1-6. Our team has recently developed and demonstrated a 4D MRI approach for dynamic imaging and profiling of unconstrained wrist motion.7 In the present analysis, this new kinematic profiling approach was deployed on an asymptomatic subject cohort to develop baseline normative profile estimates for rotational and translational trajectories of the scaphoid, lunate, and capitate carpal bonesMethods
Subject Cohort and MRI Methods: A GE Premier 3T MRI scanner using a 16-channel large flex coil was used to capture dynamic and static images of the wrist of 31 healthy asymptomatic subjects that provided written consent into a locally approved IRB protocol. 19 female and 12 male subjects were analyzed, aged 32 +/- 9 years.The subject’s arm was fixed with padding to give sufficient range of motion for the radial/ulnar-deviation and flexion-extension movements analyzed in this study. No physical motion constraints were utilized to guide subject motion.
Static fixed images were acquired using LAVA-Flex 3D SPGR sequence with 0.6mm isotropic voxel size. Dynamic volumes with temporal resolution of 2.3s were acquired using a highly undersampled LAVA-Flex 3D acquisition (1.6×1.6×2.5 mm3 resolution). 40 dynamic volumes were acquired for each motion, with the subject visually cued to make 3 cycles of the indicated motion. Along with the static LAVA-Flex 3D-SPGR, static fat-suppressed 3D FSE images (0.5 mm isotropic resolution) were also captured for identification of carpal abnormalities in the asymptomatic cohort.
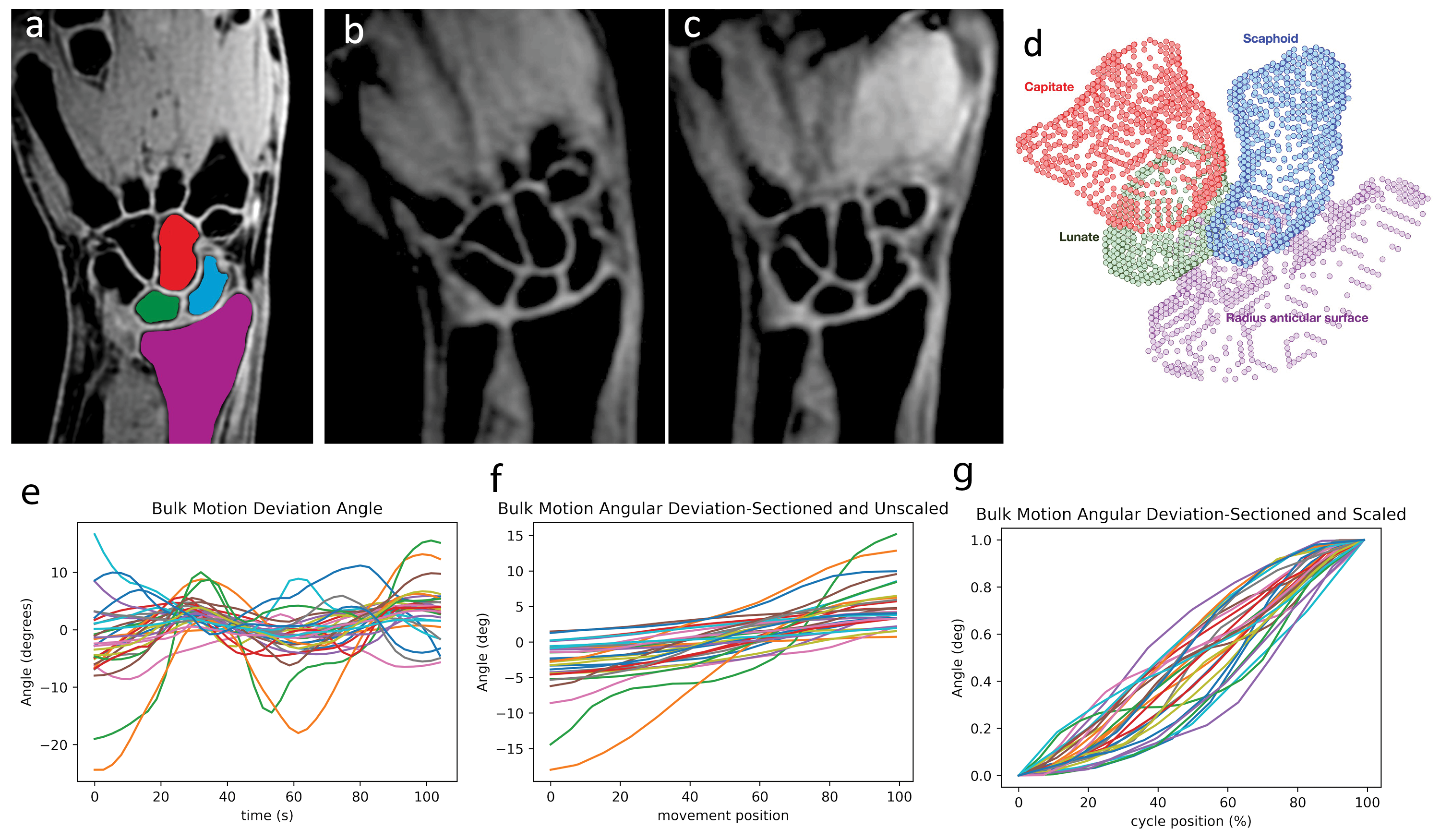
Segmentation: A 3D deep-neural network was to automatically segment the scaphoid, lunate, and capitate bones in the static and dynamic LAVA-Flex water-composition series. Manual quality inspection was performed to correct failed or flawed segmentations. Figure 1 provides sample LAVA Flex water-composition images for the static (a) and dynamic (b,c) series, along with segmentations (d) of the static images for the scaphoid, lunate, and capitate bones.
Dynamic Registration: Using these segmentations, individual carpal bone rotational angles, axes of rotation, and center of mass translations were independently derived for each of the acquired 3D time frames using a point-cloud registration of the dynamic carpal bones to the static bone model7.
Pre-Processing of Kinematic Profiles: Figure 1 (e) provides radial/ulnar deviation angles for the composite scaphoid/lunate/capitate bone group. Using these bulk angular deflection profiles, an automated algorithm found the largest half-cycle of motion (i.e. max radial to max ulnar deviation or max flexion to max extension), which were then interpolated to a common time domain grid (Figure 1f). Finally, for the purposes of normative analysis, these max cycle movements were normalized (Figure 1g). The remaining variation in Figure 1g is largely explained by nonlinear angular velocity movements between subjects. This variation was then removed by performing a transform of the time (x) axis such that each subject moved at a constant angular velocity through the bulk deflection movement. The bulk deviation and flexion movements were utilized to develop the aforementioned scaling and time-domain normalization calibrations for the individual carpal bone profiles. In addition to the rotational and translational displacement measures, ratios between the rotational and translational measures across the 3 carpal bones were also derived.
Asymptomatic Abnormality Detection: A radiologist with subspecialized training in musculoskeletal imaging interpreted the morphological images to identify asymptomatic abnormalities. For analysis purposes, these abnormalities were categorized as 1) triangular fibrocartilage complex wear/degeneration (TFC), 2) intrinsic ligament degeneration/wear, 3) carpal misalignment, and 4) presence of ganglion cysts.
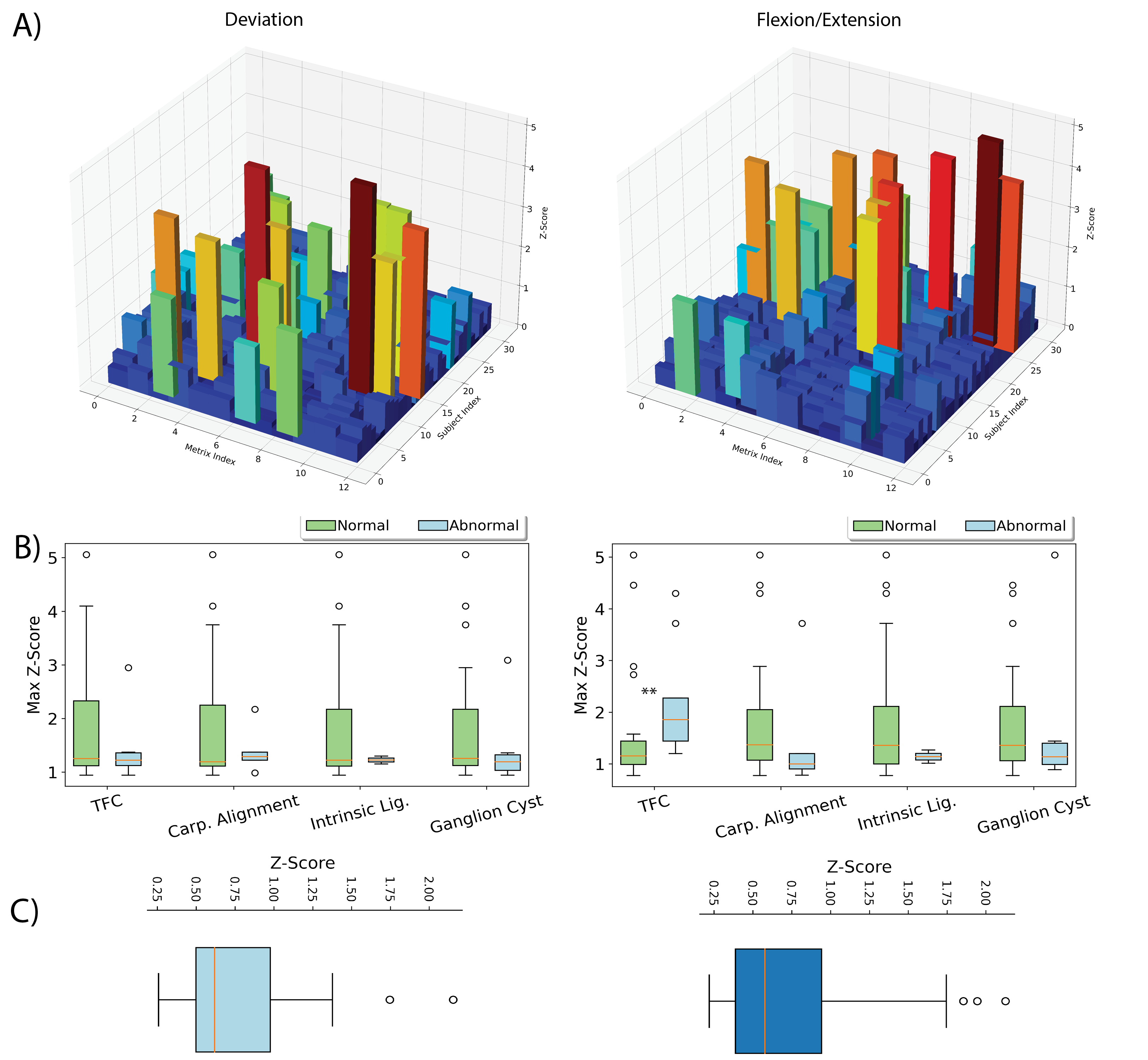
Statistical Parametric Mapping: Z-scores were computed at each normalized profile point and then collapsed via averaging to a single z-score for each subject, for each profile. Further z-score collapsing was performed by taking the maximum z-score across the profile metrics for each subject.
Results
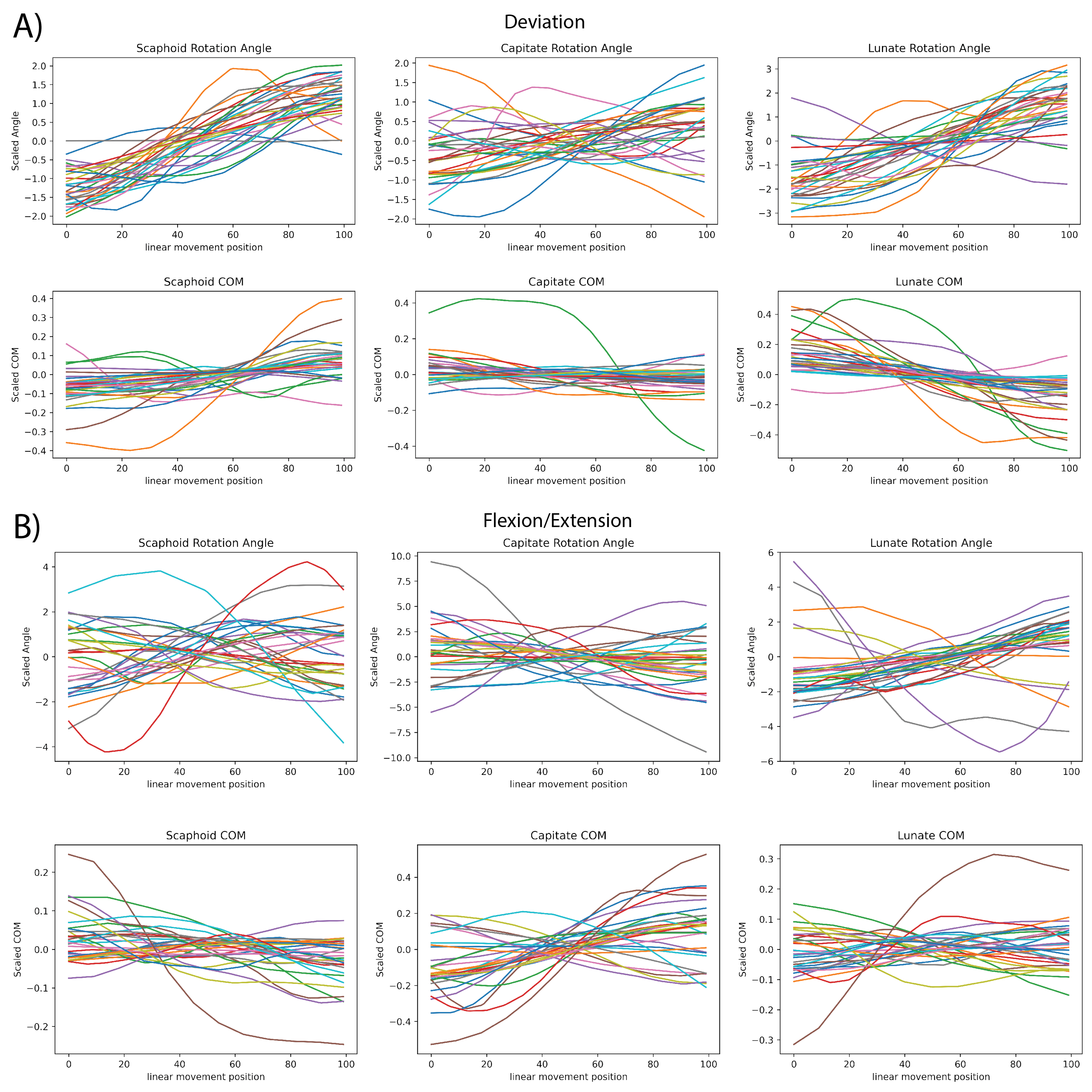
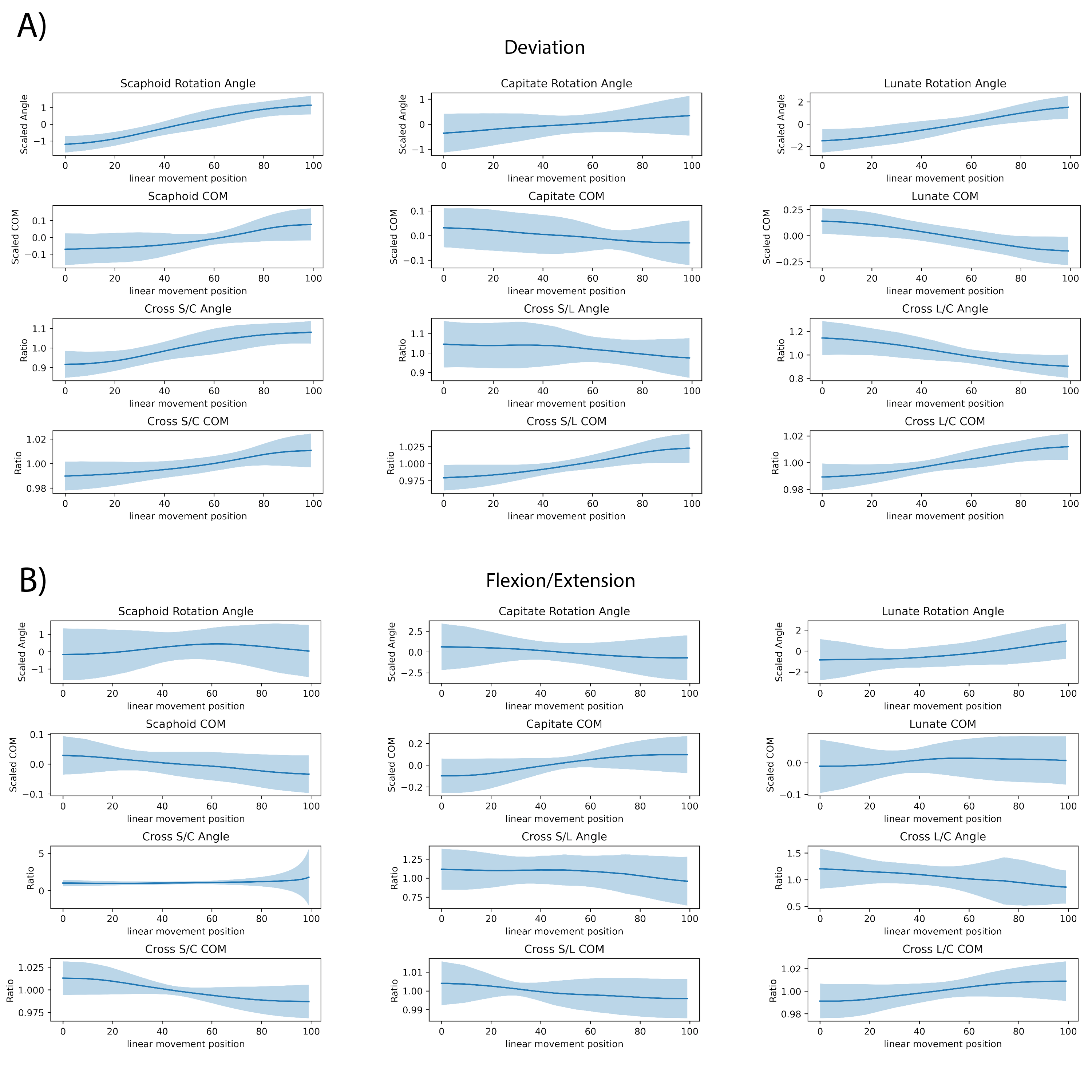
Figure 2 provides sample normalized kinematic profiles for each group after pre-processing.Figure 3 re-packages the group profiles, also including the relative bone measures, as mean profiles with variance ranges.
Figure 4 provides graphical depictions of the normative analysis. Columns represent the deviation (left) and flexion/extension (right) motions. Row A) provides bar plots of mean z-score across the 12 metrics and 31 subjects. Row B) depicts the relationship of collapsed (max) z-score for each subject as a function of radiologist-identified abnormalities. The only coherent finding from this analysis is the TFC abnormalities in the flexion/extension motion, which yielded a u-test result of p=0.01,u=44. Finally, row C) provides the collapsed subject z-score distributions for each of the motions. Of the 5 outliers in the displayed boxplots (outside of the interquartile range), only 2 of the deviation motion cases were subjects without identified abnormalities. There were no statistically significant trends between collapsed subject z-scores and age or gender.
Discussion
The results of the study clearly demonstrate the importance of normative benchmarking of kinematic profiles. The present study cohort consisted of 31 subjects with no known carpal issues and a mean age of 31 years. Of this healthy normative study cohort, 19 (61%) still had an asymptomatic abnormality that was identified on morphological MRI. Therefore, it is clear that asymptomatic and clinically-insignificant variations can and will occur within the measured profiles. Future studies will leverage this newly established normative baseline-variance to assess profiles within symptomatic wrists with radiologically-verified pathology.Acknowledgements
This study was supported by NIH R21AR075327. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.References
- A. J. Schnorenberg, B. A. Slavens, M. Wang, L. C. Vogel, P. A. Smith, and G. F. Harris. Biomechanical model for evaluation of pediatric upper extremity joint dynamics during wheelchair mobility. Journal of Biomechanics, 47(1):269–276, January 2014.
- G. Wu, F. C. T. van der Helm, H. E. J. DirkJan Veeger, M. Makhsous, P. Van Roy, C. Anglin, J. Nagels, A. R. Karduna, K. McQuade, X. Wang, F. W. Werner, and B. Buchholz. ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion—Part II: shoulder, elbow, wrist and hand. Journal of Biomechanics, 38(5):981–992, May 2005.
- C. Muhle, J. Brossmann, and M. Heller. Kinematic CT and MR imaging of the patellofemoral joint. European Radiology, 9(3):508–518, 1999.
- J. E. Johnson, P. Lee, T. E. McIff, E. B. Toby, and K. J. Fischer. Scapholunate ligament injury adversely alters in vivo wrist joint mechanics: An MRI-based modeling study. Journal of Orthopaedic Research, 31(9):1455–1460, April 2013.
- G. Li, T. H. Wuerz, and L. E. DeFrate. Feasibility of using orthogonal fluoroscopic images to measure in vivo joint kinematics. Journal of biomechanical engineering, 126(2):313–318, 2004.
- Foster B H, Shaw C B, et al. A principal component analysis-based framework for statistical modeling of bone displacement during wrist maneuvers. Journal of Biomechanics 2019; pages 1–9.
- Zarenia et al, Unconstrained Kinematic MRI Tracking of Wrist Carpal Bones, arXiv, 2021, 2111.04582
Figures