0533
Accelerating IVIM and DTI for assessing microstructural changes after acute hamstring injury
Susanne Rauh1, Jithsa Monte2, Melissa Hooijmans2, Joep Suskens3, Oliver Gurney-Champion2, Johannes Tol3, Mario Maas2, Aart Nederveen2, and Gustav Strijkers1
1Department of Biomedical Engineering and Physics, Amsterdam UMC, Amsterdam, Netherlands, 2Department of Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 3Department of Orthopedic Surgery, Amsterdam UMC, Amsterdam, Netherlands
1Department of Biomedical Engineering and Physics, Amsterdam UMC, Amsterdam, Netherlands, 2Department of Radiology and Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 3Department of Orthopedic Surgery, Amsterdam UMC, Amsterdam, Netherlands
Synopsis
DTI and IVIM are sensitive to hamstring injuries, but suffer from long scan times. Using b-values above a certain threshold only (high-b DTI) or a simplified IVIM approach (sIVIM-DTI), which estimates the perfusion fraction and diffusion tensor, can reduce the scan time while inherently correcting DTI-indices for IVIM effects. We showed in this work that those methods provide similar sensitivity to hamstring injuries in comparison to a full IVIM-DTI fit while reducing acquisition time up to 42%. Since no difference in perfusion fraction was found between injury states, we suggest high-b DTI is the method of choice in this application.
Introduction
Hamstring injuries are amongst the most common injuries in elite athletes and show high recurrence rates1,2. Diffusion tensor imaging (DTI) and intravoxel incoherent motion (IVIM) are sensitive to muscle micro damage3,4 and may be able to assess acute muscle injury recovery and predict return-to-play (RTP). IVIM-corrected DTI has an improved reproducibility compared to conventional DTI5. A downside of IVIM-correction is the substantial increase in scan time. Applying the DTI fit only to high b-values above a certain threshold or using a simplified IVIM-DTI approach may significantly reduce scan time while inherently correcting DTI indices for IVIM effects. The goal of this work was to evaluate the sensitivity of accelerated DTI and IVIM-DTI to acute hamstring injuries compared to a full IVIM-DTI fit.Methods
MRI datasets were acquired in 41 elite athletes (2 female, mean age 27.3 years) with acute hamstring injury using a 3T-MRI (Philips Ingenia) at three time points (Figure 1). The scan protocol included an anatomical Dixon scan (1.5x1.5x2.5mm³, 80 slices, 6 echoes) and a DTI-IVIM scan (duration 11:08min, SE-EPI; 3x3x5mm³, 40 slices, TE/TR=55ms/5914ms, SPAIR and gradient-reversal fat suppression, SENSE=1.5) with 10 b-values (range 0-600s/mm², 8x b=0s/mm²) and 56 diffusion directions. The DTI data was PCA-denoised and registered to the anatomical scan using QMRTools6. The diffusion tensor was calculated using three different fitting methods:- IVIM-corrected DTI (in the following called ‘conventional’), consisting of four steps:
a. IVIM fit the mean data.
b. Voxel-wise IVIM fit with fixed pseudo-diffusion coefficient D* obtained from step a.
c. IVIM-component subtraction from signal: $$$ S_{DTI} = S - S_{0,IVIM}\cdot f\cdot e^{-b\cdot D^{*}} $$$
d. DTI fit to SDTI using all b-values. - High-b DTI. The data was retrospectively undersampled, discarding all b-value<200s/mm², resulting in b=200,400,600s/mm² and 32 diffusion directions. Then a DTI fit was applied.
- sIVIM-DTI: The same high-b-values and directions as in high-b DTI were used (32 directions) and b=0s/mm² data (8 scans) were included to estimate the perfusion fraction f, yielding 40 b-value/direction combinations. A simplified IVIM-DTI approach was applied:
$$$S(b) = S_0\cdot (f\cdot\delta(b) + (1-f)\cdot e^{-b\underline{g}^T \underline{\underline{D}}\underline{g}}$$$
Manual segmentation of the injured and contralateral muscle was performed in ITK-snap (www.itksnap.org). ROIs consisted of 7 slices overlaying the origin of the injury and a closely matching region in the contralateral muscle. The mean and standard deviations of the DTI parameters (tensor eigenvalues (λ1–λ3), mean diffusivity (MD), fractional anisotropy (FA), perfusion fraction (f)) were calculated within the segmentation for the injured and contralateral muscle and for each method and time point. A repeated measures Anova was used to evaluate the three methods (SPSS). The sensitivity of the methods to injury was assessed by comparing the difference between the injured and contralateral muscle (Δ injured-healthy). The stability of the methods was evaluated by comparing the standard deviations of the DTI parameters in the healthy muscle. The difference between the methods and injury states was assessed for both injury states separately.
Results
The proposed methods yield a scan time reduction of 42% (high-b DTI) and 28% (sIVIM-DTI) compared to the conventional method. Parameter maps are shown in Figure 2. Sensitivity: At baseline, a larger Δ injured-healthy was found with high-b DTI and sIVIM-DTI for λ1–λ3 and MD compared to the conventional method. No difference was found for FA or between sIVIM-DTI and high-b DTI. The difference between the methods disappeared at 2-weeks and RTP. After 2-weeks, Δ injured-healthy of FA was higher for sIVIM-DTI than high-b DTI (Figure 3). Stability: The standard deviations of λ2, λ3, MD, FA and f were significantly higher in high-b DTI and sIVIM-DTI compared to the conventional fit at baseline and 2-weeks. No differences were found for λ1 (Figure 4). The standard deviation for FA was higher in sIVIM-DTI than high-b DTI. No differences were found at RTP. Injury sensitivity and method differences: At baseline and 2-weeks, the injured muscle had higher MD and eigenvalues than the healthy muscle for all methods. No effect for injury was found in FA and f. The difference disappeared at RTP. An offset between conventional fitting and accelerated fit outcome measures was found (Figure 5). λ1–λ3 and MD were highest with conventional fitting and higher in high-b DTI than sIVIM-DTI. The opposite effect held for FA and f.Discussion
Our data showed that the sensitivity to hamstring injuries is preserved with our accelerated high-b DTI and sIVIM-DTI methods. The increased Δ injured-healthy values at baseline might indicate improved sensitivity. The higher standard deviation with accelerated methods could be a result of higher noise contribution in the high b-value data. The overall offset between the conventional and accelerated approaches at all time points might be due to more noise at high b-values, reduced data used for the fit or a suboptimal fixed D* value in the conventional fit which might result in remaining IVIM signal in SDTI. With both conventional IVIM-DTI and sIVIM-DTI methods, no difference was observed in f between injury states. This might indicate that f is not sensitive to hamstring injuries.Conclusion
High-b DTI and sIVIM-DTI reduce scan time and preserve sensitivity to hamstring injuries. Since f shows no sensitivity to injury, the high-b DTI method may be considered the best method for this application.Acknowledgements
The authors would like to thank Martijn Froeling for help with the scan protocol and the pre-processing pipeline. The study was partly funded by a grant from ‘NBA & GE Orthopedics and Sports Medicine Collaboration’, USA.References
1. Koulouris G, Connell DA, Brukner P, Schneider-Kolsky M. Magnetic resonance imaging parameters for assessing risk of recurrent hamstring injuries in elite athletes. Am J Sports Med. 2007;35(9):1500-1506. doi:10.1177/03635465073012582. Slavotinek JP, Verrall GM, Fon GT. Hamstring injury in athletes: Using MR imaging measurements to compare extent of muscle injury with amount of time lost from competition. Am J Roentgenol. 2002;179(6):1621-1628. doi:10.2214/ajr.179.6.1791621
3. Hooijmans MT, Monte JRC, Froeling M, et al. Quantitative MRI Reveals Microstructural Changes in the Upper Leg Muscles After Running a Marathon. J Magn Reson Imaging. 2020. doi:10.1002/jmri.27106
4. Froeling M, Oudeman J, Strijkers GJ, et al. Muscle changes detected with diffusion-tensor imaging after long-distance running. Radiology. 2015;274(2):548-562. doi:10.1148/radiol.14140702
5. Monte JR, Hooijmans MT, Froeling M, et al. The repeatability of bilateral diffusion tensor imaging (DTI) in the upper leg muscles of healthy adults. Eur Radiol. 2019. doi:10.1007/s00330-019-06403-5
6. Froeling M. QMRTools: a Mathematica toolbox for quantitative MRI analysis. J Open Source Softw. 2019;4(38):1204. doi:10.21105/joss.01204
Figures
Figure 1: Workflow of the MRI measurements of patients with acute hamstring injury. The patients were scanned within 7 days after the injury (Visit 1, baseline scan), 2 weeks after visit 1 (Visit 2, 2-weeks scan) and within 7 days after Return-to-Play (Visit 3, RTP). 41 patients were included and completed the baseline and 2-weeks follow-up scan. 12 patients completed the RTP scan. For 12 patients 2-weeks follow-up coincided with RTP. 17 patients had no RTP scan.
Figure 2: Parameter maps of Mean Diffusivity (MD) and Fractional Anisotropy (FA) from all three fitting methods of one representative patient at baseline. Segmentations of the injury (red) and the healthy contralateral muscle (green) are overlaid. No clear difference between the parameter maps obtained from the different fitting methods can be observed.
Figure 3: Difference between the injured–healthy parameters (Δ) for all three methods and time points. For all methods, Δ injured–healthy values lie in a similar range without obvious outliers, indicating preserved sensitivity to injury of accelerated DTI and IVIM-DTI methods compared to the conventional fit. A significantly higher Δ injured–healthy was found at baseline for high-b DTI and sIVIM in λ1, for high-b DTI in λ3 and after 2-weeks for sIVIM compared to high-b DTI in FA. (conv. = conventional)
Figure 4: Standard deviations of λ1 and λ3 in the contralateral healthy muscle for all three time points and methods. No difference was found for λ1. For λ3, standard deviations were significantly higher with the accelerated methods, however, the absolute differences were small (mean difference λ3 between conventional and high-b DTI/sIVIM: 0.23/0.23, 0.22/0.22, 0.20/0.21, for baseline, 2-week follow-up and RTP respectively). (conv. = conventional)
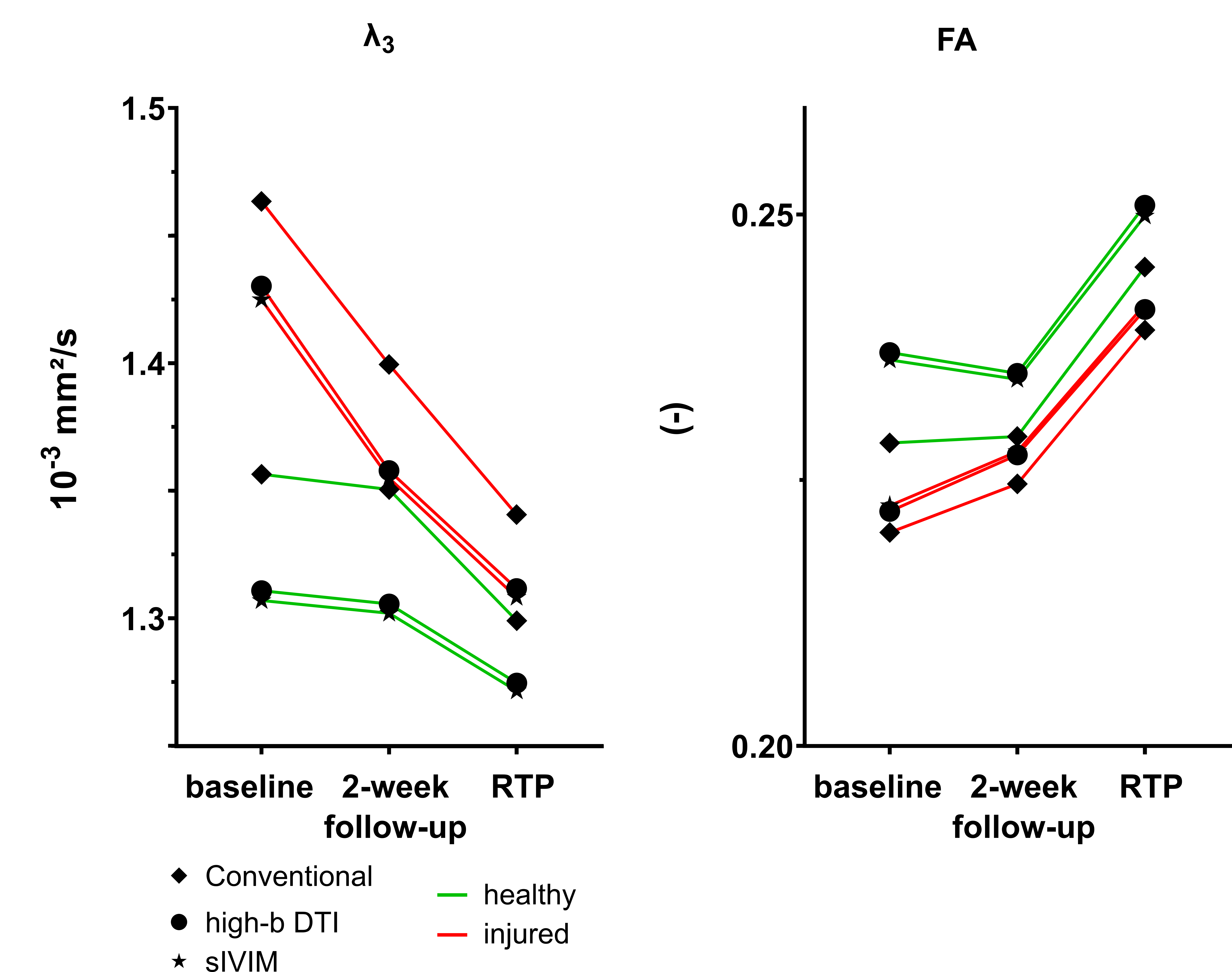
Figure 5: Time course of λ3 and FA for the injured and healthy muscle for all fitting methods (mean values plotted). The healthy values stay almost constant between baseline and 2-week follow-up for all methods, while the injured values converge towards the healthy. The change in the healthy values at RTP might be explained by less data (N=12 at RTP). An offset between the conventional and proposed methods can be observed for both, injured and healthy muscle at all three time points. Only a minor difference is visible between high-b DTI and sIVIM-DTI.
DOI: https://doi.org/10.58530/2022/0533