0495
4D free-breathing variable density stack-of-stars functional MR urography in young children without sedation: A clinical feasibility study1Department of Diagnostic and Interventional Radiology, University Hospital Tuebingen, Tuebingen, Germany, 2Philips GmbH Market DACH, Hamburg, Germany
Synopsis
High-quality magnetic resonance urography (MRU) is clinically valuable to provide a comprehensive evaluation of the renal function and urinary tract in children without ionizing radiation. However, respiration-related patient motion remains a major challenge that impairs diagnostic image quality and hampers an accurate quantitative analysis. In this study, we adopt a novel high temporospatial resolution dynamic-contrast-enhanced (DCE) MRI technique based on 3D radial stack-of-stars gradient-echo sequence acquisition in combination with elliptical variable density k-space scheme for morphological and quantitative MRU and demonstrate its motion robustness in small children in free breathing without sedation.
Introduction
Magnetic resonance urography (MRU) is a valuable imaging modality allowing comprehensive evaluation of the kidneys and urinary tract in children by providing both morphologic and functional information without exposing the patient to ionizing radiation 1. However, in very young children general anesthesia or conscious sedation is typically required to prevent artifacts related to patient motion 2. This complicates the entire procedure and leads to increased total exam time and potential risks to the child, which has recently drawn particular attention in the community 3. On the other hand, a newly introduced 4D high spatiotemporal resolution dynamic-contrast-enhanced (DCE) MRI based on variable density elliptical centric radial stack-of-stars sharing technique 4 has shown superb image quality against motions. In this work we adopted the same concept and aimed to investigate the clinical feasibility applying this method for functional MRU in young pediatric patients in free breathing without sedation.Methods
For high temporospatial DCE-MRI, 4D free-breathing radial stack-of-stars imaging was applied. Several important technical components were detailed as follows:· Pseudo-golden angle sampling order in the kxy plane 5.6 that has a more homogeneous distribution of the consecutively acquired radial spokes in space and time. This leads to a lower correlation of variations in terms of phase errors caused by motion or hardware imperfections such as trajectory delay.
· Variable density sampling scheme with a high-density radial grid at central k-space and lower densities at peripheral k-space 7
· Respiratory soft gating based on weighting of the k-space data depending on the respiratory displacement measured by the respiratory belt signals 8,9
· Keyhole and view sharing with temporal domain k-space weighted image contrast (KWIC) 10
· Bulk motion compensation across dynamics with Flexible Elastic Registration (FEIR) 11,12
· Perspective sampling and online reconstruction and visualization on the MR console
A schematic overview of the approach is shown in Figure 1. T1-weighted radiofrequency (RF)-spoiled gradient-echo, aka turbo-field-echo (TFE), pulse sequence was employed with spectral adiabatic inversion recovery (SPAIR) for fat suppression. For 3D dynamic elliptical centric keyhole, the k-space center is acquired with higher sampling density and the k-space peripheries is sampled with quadratically reduced radial density for an efficient imaging time acceleration 4.
For clinical feasibility 4D free-breathing variable density stack-of-stars (4D FB) was studied in two patients (3 month-old with horseshoe kidneys and 4-year-old with duplex right kidney, respectively) on a 1.5T whole-body clinical system (Ingenia, Philips Healthcare, Best, the Netherlands) without sedation. A coronal 3D imaging volume was acquired covering both kidneys, ureters, and the bladder. Typical scan parameters were summarized in Table 1. A radial density referring to the Nyquist theorem for a corresponding image matrix size in the kxy plane was applied, while a SENSE (SENSitivity Encoding) factor was used in the kz direction for scan time reduction. The obtained images were transferred to the workstation and analyzed as previously described by Khrichenko and Darge using the “CHOP-fMRU” tool 11.
Results and Discussion
Representative images of arterial and urographic phases are shown in Figure 2. In general, 4D FB achieved comparable image quality to standard Cartesian with breath hold. When comparing to Cartesian without breath hold, e.g., in sedation or general anesthesia, 4D FB showed improved image quality with less motion artifacts in comparison to conventional Cartesian. Figure 3 shows representative maximum-intensity-projection (MIP) images of 4D FB images in different phases. The kidneys remained at the same position without motion artefacts, which was deemed as one of the key criteria for analysis with CHOP-fMRU.Enhancement curves are shown in Figure 4, comparing 4D FB and conventional Cartesian, where the latter was performed during general anesthesia. Note that the hopping enhancement curves in the conventional Cartesian urography were caused by renal movement due to respiration between minute 3 and 6 after the initial apnoeic phase. In contrast, 4D FB presented smooth curves due to minimized motion effect despite free breathing, which potentially resulted in improved fitting of the model to the measured signal and a more reliable estimation of kidney function 14. Table 2 reports the split renal function by CHOP-fMRU using 4D FB. Due to improved image quality the evaluation was found easier and faster with more confidence, although more systematic investigations are needed to study its performance and accuracy 15.
Conclusion
We demonstrated the feasibility of applying 4D free-breathing variable density stack-of-stars imaging for functional MRU in young pediatric patients with improved image quality and motion robustness. While initial results have shown promise for clinical routine application without sedation for assessing disorders of the pediatric urinary tract and renal function, further investigations are needed to study its performance and accuracy against clinical standard of care.Acknowledgements
No acknowledgement found.References
1. Dickerson EC, et al. Pediatric MR Urography: Indica tions, Techniques, and Approach to Review. RadioGraphics 2015;35:1208.
2. Dillman JR, et al. MR urography in children and adolescents: techniques and clinical applications. Abdom Radiol 2016;41:1007.
3. FDA review results in new warning about using general anesthetics and sedation drugs in young children and pregnant women. Safety Announcement. US Food and Drug Administration, Drug Safety Communication. 2016.12.14.
4. Beck GM et al. High spatial and temporal free breathing T1 contrast enhanced imaging using a novel 4D variable density, elliptical centric radial stack-of-stars sharing approach. Proc Int Soc Magn Reson Med 2018;26;1000.
5. Wuelbern JH, et al. Dixon Imaging with Golden Angle Stack of Stars Acquisition. Proc Int Soc Magn Reson Med 2015;23:3648.
6. Hedderich DM, et al. Clinical Evaluation of Free-Breathing Contrast-Enhanced T1w MRI of the Liver using Pseudo Golden Angle Radial k-Space Sampling. RoFo 2018;190:601.
7. Peters D, et. al. Radial Undersampling that is Variable in kz. Proc Int Soc Magn Reson Med-ESMRMB 2007;15:0304.
8. Forman C, et al. Reduction of respiratory motion artifacts for free-breathing whole-heart coronary MRA by weighted iterative reconstruction. Magn Reson Med 2015;73:1885.
9. Menini A, et al. Self-calibrated soft gating for respiratory resolved 3D+ time lung ZTE. Proc ISMRM-ESMRMB 2018, Paris, France.
10. Song HK and Dougherty L. k-space weighted image contrast (KWIC) for contrast manipulation in projection reconstruction MRI Magn Reson Med 2000;44:825.
11. Kabus S and Lorenz C. Fast elastic image registration. Proc Med Image Comput Computerassisted Intervention (MICCAI) 2010;13:81.
12. Zhang S, et al. Cardiac magnetic resonance T1 and extracellular volume mapping with motion correction and co‑registration based on fast elastic image registration. MAGMA 2018;31:115.
13. Khrichenko D, et al. Functional analysis in MR urography - made simple. Pediatr Radiol 2010;40:182.
14. Kurugol S, et al. Reliable estimation of kidney filtration rate with DCE-MRI using motion-robust high spatiotemporal resolution Radial VIBE. Proc Int Soc Magn Reson Med 2017;25:3289.
15. Kurugol S, et al. Prospective pediatric study comparing glomerular filtration rate estimates based on motion-robust dynamic contrast-enhanced magnetic resonance imaging and serum creatinine (eGFR) to 99mTc DTPA. Pediatr Radiol 2020;50:698.
Figures
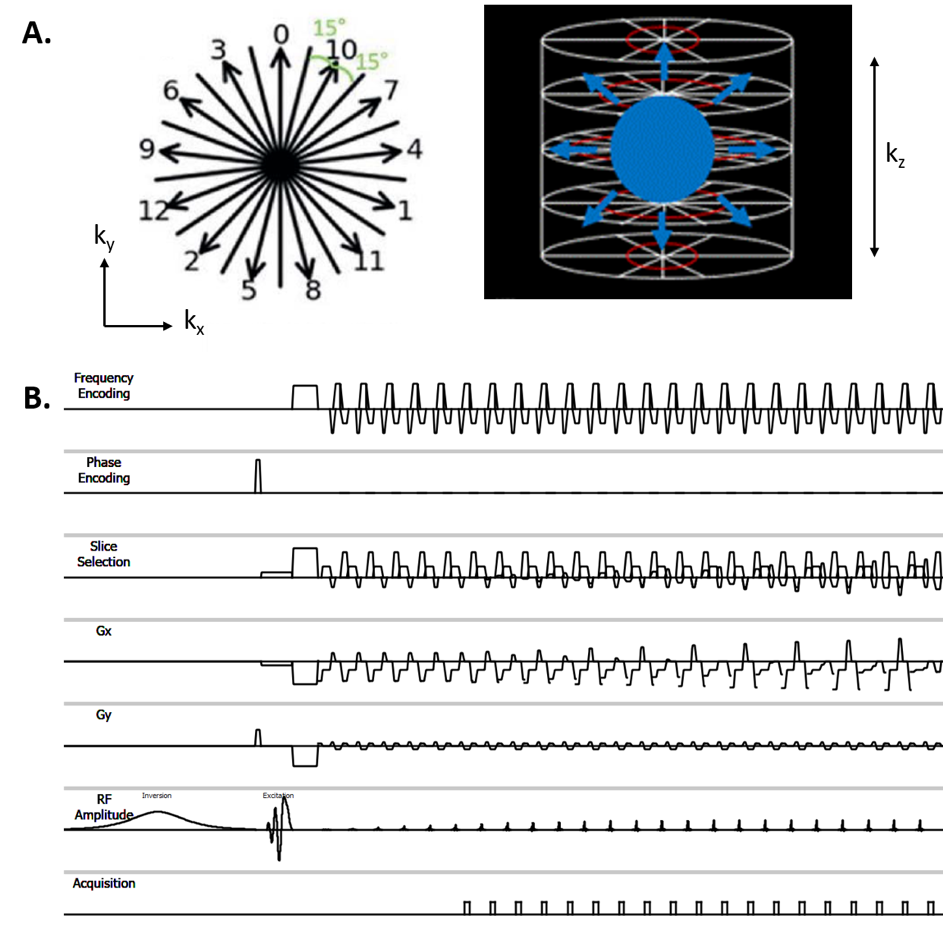
Figure 1: Schematic overview of 4D free-breathing variable density radial stack-of-stars used in this study. (A) Sampling order of the pseudo-golden angle radial spokes in the kxy plane (left) and variable density with elliptical centric scheme (right) combined with keyhole in the k-space trajectory. (B) Simplified pulse sequence diagram of stack-of-stars. This allows for a more homogeneous distribution of the consecutively acquired radial k-space spokes within a defined Nyquist ellipsoid close in time.
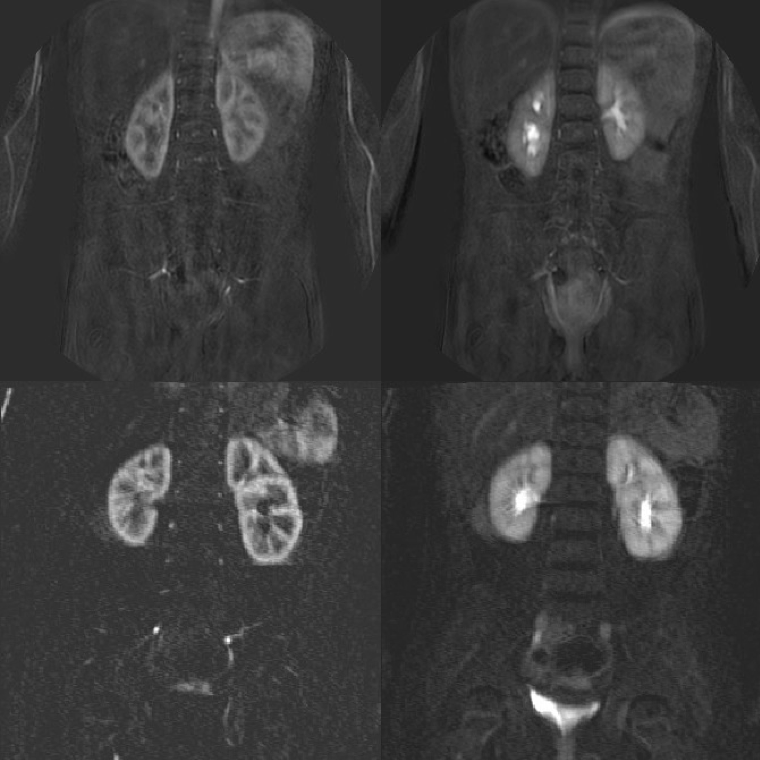
Figure 2. MRU images acquired using 4D FB (top) in comparison to standard Cartesian (bottom). Top: Arterial and urographic phases of a 4-year-old patient using 4D FB. Image quality remains stable throughout the whole examination. Bottom: A age-matched patient with duplex kidney on the left side examined under general anesthesia with conventional Cartesian. Note the motion artefacts on the right image due to respiration.
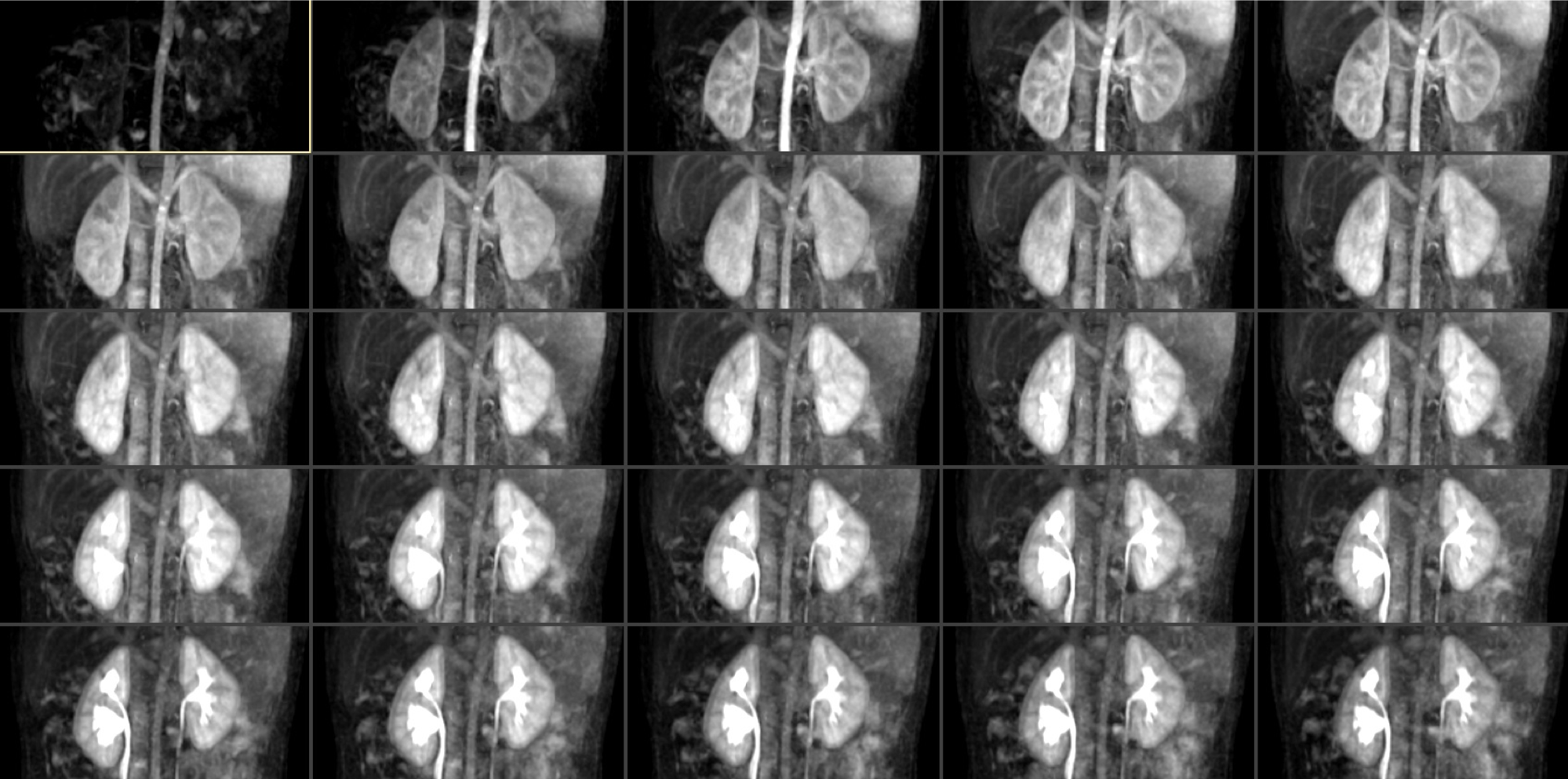
Figure 3. 4D FB MRU with the maximum-intensity-projection (MIP) images of a 4-year-old patient. The image quality is excellent for all sequences despite free breathing and respiratory motion. The duplex kidney on the right side can be easily depicted.
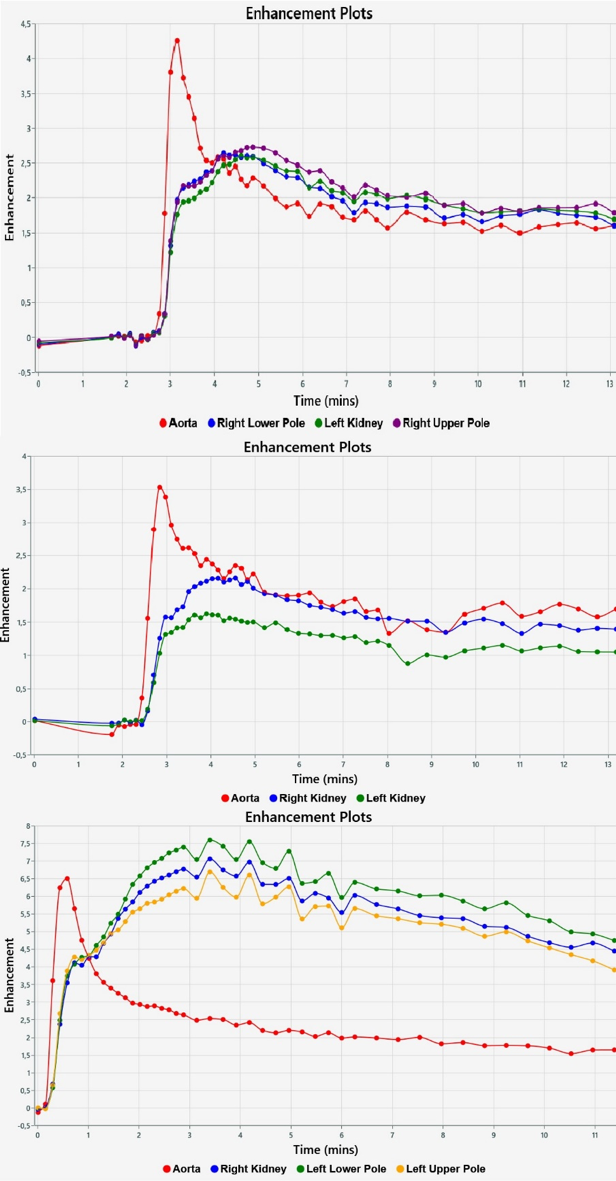
Figure 4. MRU tissue enhancement curves for 4D FB (top and middle) and standard Cartesian (bottom). Whereas in 4D FB the enhancement curves are smooth due to minimized motion effect, in conventional Cartesian hopping curves are seen between minute 3 and 6 due to severe respiratory motions and different kidney positions in the examination volume after the initial apnoeic phase. Top: a 4-year-old patient. Middle: a 3-month patient. Bottom: the same age-matched patient as in Figure 2. Curves were generated by the CHOP tool.
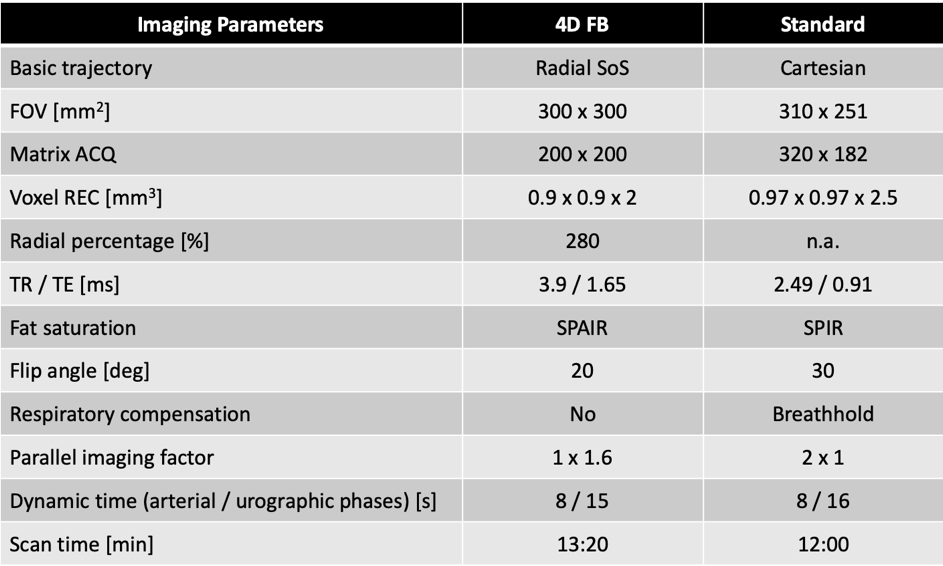
FB = free-breathing; SoS = stack-of-stars; FOV = field of view; ACQ = acquired; REC = reconstructed; TR = repetition time; TE = echo time
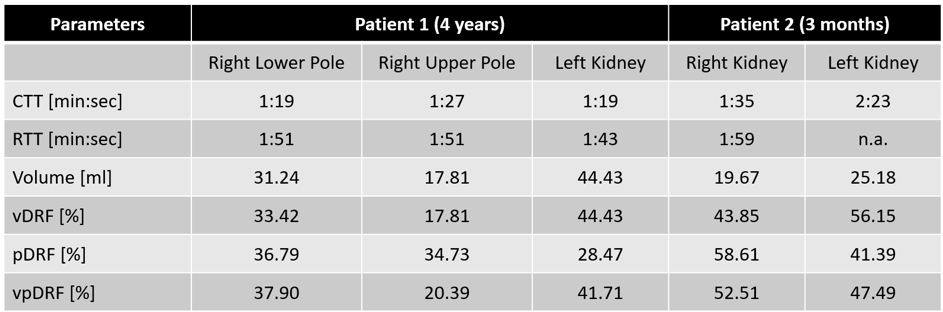
Table 2: Split renal function of the studied patients. RTT of the left kidney in patient 2 could not be determined because the contrast media did not reach the proximal ureter due to obstruction. CTT: Calyceal transit time; RTT: Renal transit time; Volume: Renal parenchymal volume; vDRF: Volumetric split renal function; pDRF: Patlak split renal function; vpDRF: Volumetric and Patlak split renal function.