0491
Smaller MRgFUS lesions that overlap patient-fit normative VIM—Precentral tracts improve Quality-of-Life outcomes in Essential Tremor1Stanford University, Stanford, CA, United States
Synopsis
While Focused-Ultrasound thalamotomy has proven effective at reducing tremor, traditional targeting methods can be suboptimal at balancing primary tremor-reduction outcomes against undesired side-effects. The traditional “canonical” technique involves an indirect method which applies a non-individualized stereotactic coordinate atlas towards identifying the presumed approximate location of VIM thalamus, the ablation target; the canonical lesion is empirically grown in size based-on dynamic intraoperative feedback from an awake patient, until the surgeon judges that an appropriate balance of tremor-reduction and side-effect risk has been achieved. We propose optimized methods to define and monitor the ideal anatomical ablation for optimized tremor-reduction/Quality-of-Life balancing.
Introduction
Essential Tremor (ET) resulting in intention-based trembling of the hand can limit Quality-of-Life (QoL). While tremor reduction is the prima-facie goal of MRI-guided Focused-Ultrasound (MRgFUS) treatment, symptomatic improvement aims to improve QoL. If treatment results in tremor reduction, but worsens QoL, then the patient has not been well-served.MRgFUS VIM-thalamotomy is established for reducing tremor in ET.1–3 However, possible side-effects may compromise post-MRgFUS QoL. The traditional “canonical” MRgFUS thalamotomy technique is arguably suboptimal towards QoL outcomes; it involves population-averaged atlas-defined stereotactic coordinates approximately referenced relative to landmarks identifiable on preoperative structural MRI (i.e. a line connecting the anterior and posterior commissure); treatment subsequently proceeds by initially approximating the ablation target, followed by empirically adjusting and growing the lesion over repeated sonications in an awake interactive patient until the surgeon judges that tremor control is balanced against expected side-effects.4–7 More optimized and patient-specific preoperative targeting techniques are desired to enable more accurate and precise lesion targeting, in order to optimize QoL outcomes while achieving efficacious tremor-reduction.
We investigate relationships between QoL outcomes, tremor-control, and neuroanatomical ablation-characteristics utilizing patient-fit normative tractography. Overall, we seek improved MRgFUS targeting techniques and intraoperative ablation guidelines to optimize QoL after MRgFUS thalamotomy for ET.
Methods
An institutional database of 82 ET patients treated with MRgFUS was retrospectively studied. Subjects with <3mo follow-up were excluded, leaving 62 subjects. Analysis occurred as follows:1) Patients were categorized by postoperative QoL (“better”, “same”, or “worse”), determined from last available follow-up clinical visit.
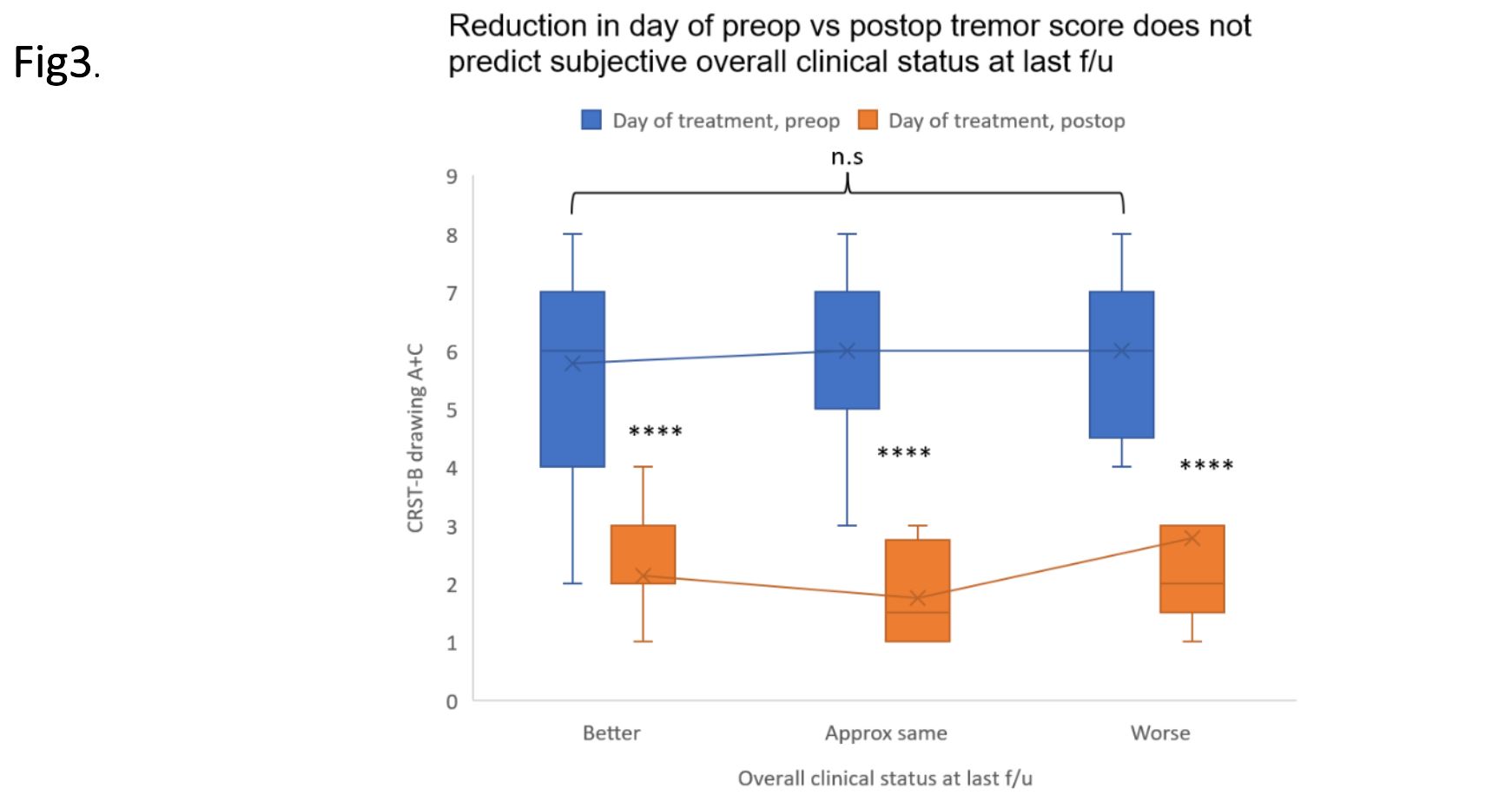
2) Immediate pre/post MRgFUS CRST (Clinical Rating Scale for Tremor) hand tremor scores were compared for the “better”, “same”, and “worse” groups. (Kruskal Wallis)
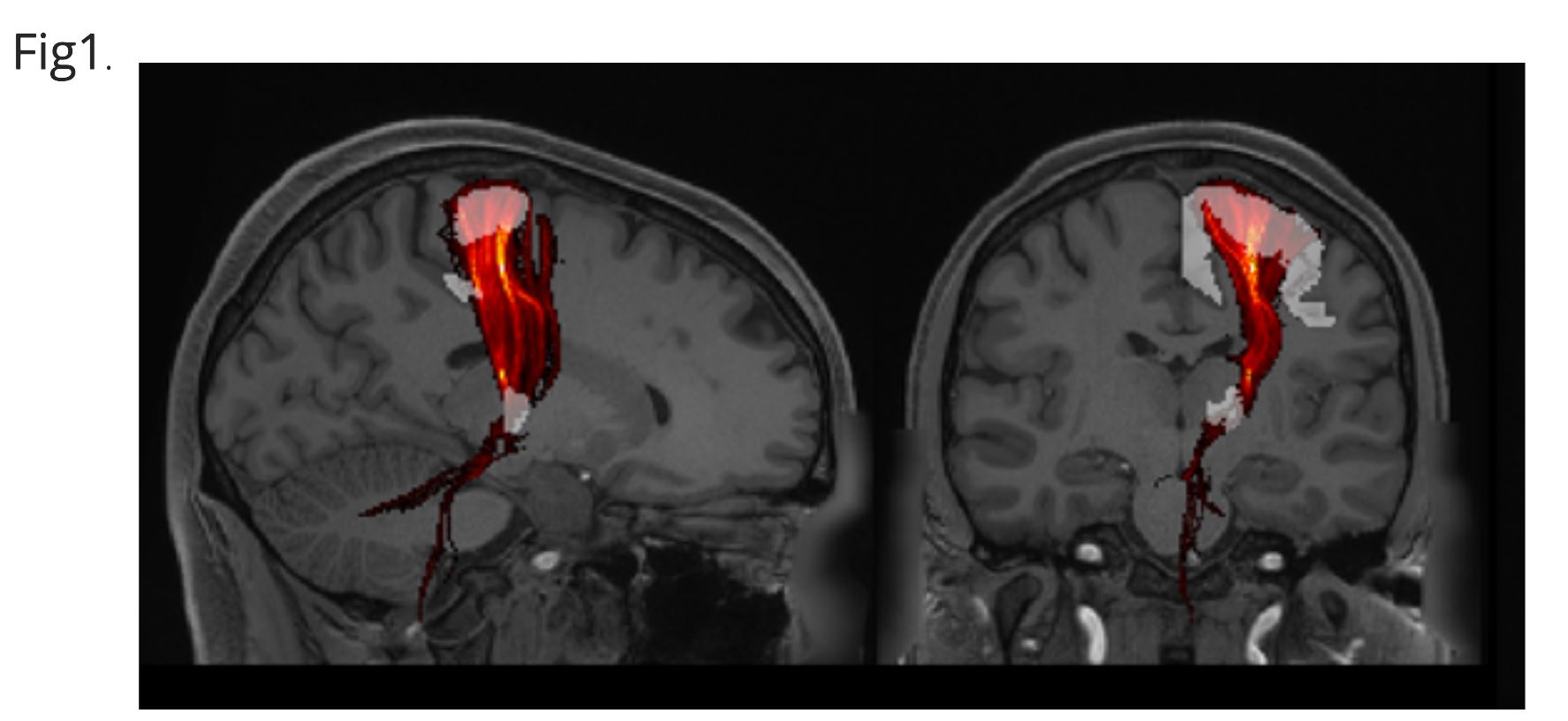
3) Patient-specific thalamic maps were determined through patient-fit normative tractography (Fig.1). Based on normative probabilistic tractography using the Human Connectome Project’s (HCP) dataset8, streamlines probability maps were co-registered to each subject’s pre-operative T1-weighted MRI: VIM(seed)—precentral-gyrus(“M1”, target). The VIM mask was derived from the DISTAL-atlas9, while the M1 mask from the Harvard-Oxford Atlas10–13. Streamlines probability maps were determined using FMRIB Software Library (FSL) probabilistic tractography toolbox (FDT)14–16. The normative VIM—M1 tract map was co-registered and warped onto each subject’s preoperative MRI using Advanced Normalization Tools (ANTs).17 This workflow was based on a previously published method.4
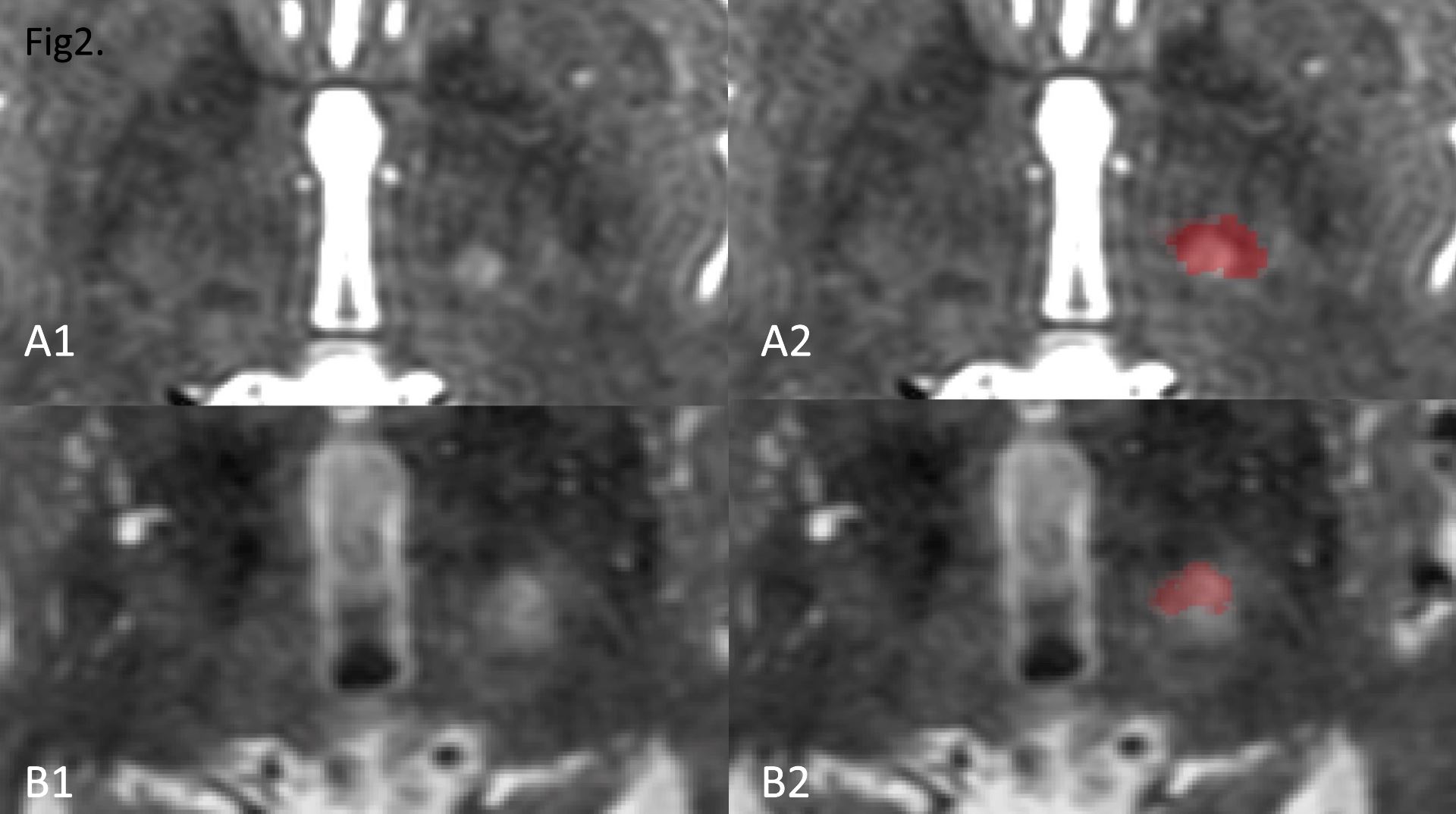
4) Ablations (“lesions”) were manually segmented from immediate postoperative T2 weighted-MRI, utilizing ITK-SNAP18; segmentations included Zone I+II (correlating to the true ablation), excluding Zone III (representing vasogenic edema).19 Lesion-segmentations were subsequently also co-registered with the patient-fit VIM—M1 tract maps, again using ANTs (Fig.2).
5) Normative tractography coefficients (NTC) were calculated for each subject as the number of target voxels overlapping with HCP group-averaged streamlines probability map (weighted by number of streamlines with overlapping voxels) divided by the target volume. NTCs are linearly related to degree of lesion-to-map overlap and inversely related to lesion size.
6) “Better” and “Same” groups were combined to form a single “better/same” group, for performing two-group comparison testing with the “worse” group.
7) Optimal between-QoL-group segmented lesion volume thresholds were statistically identified based on bootstrapped maximization of Youden’s Index (YI). Univariate logistic regression assessed predictiveness of lesion volume and NTC in predicting QoL.
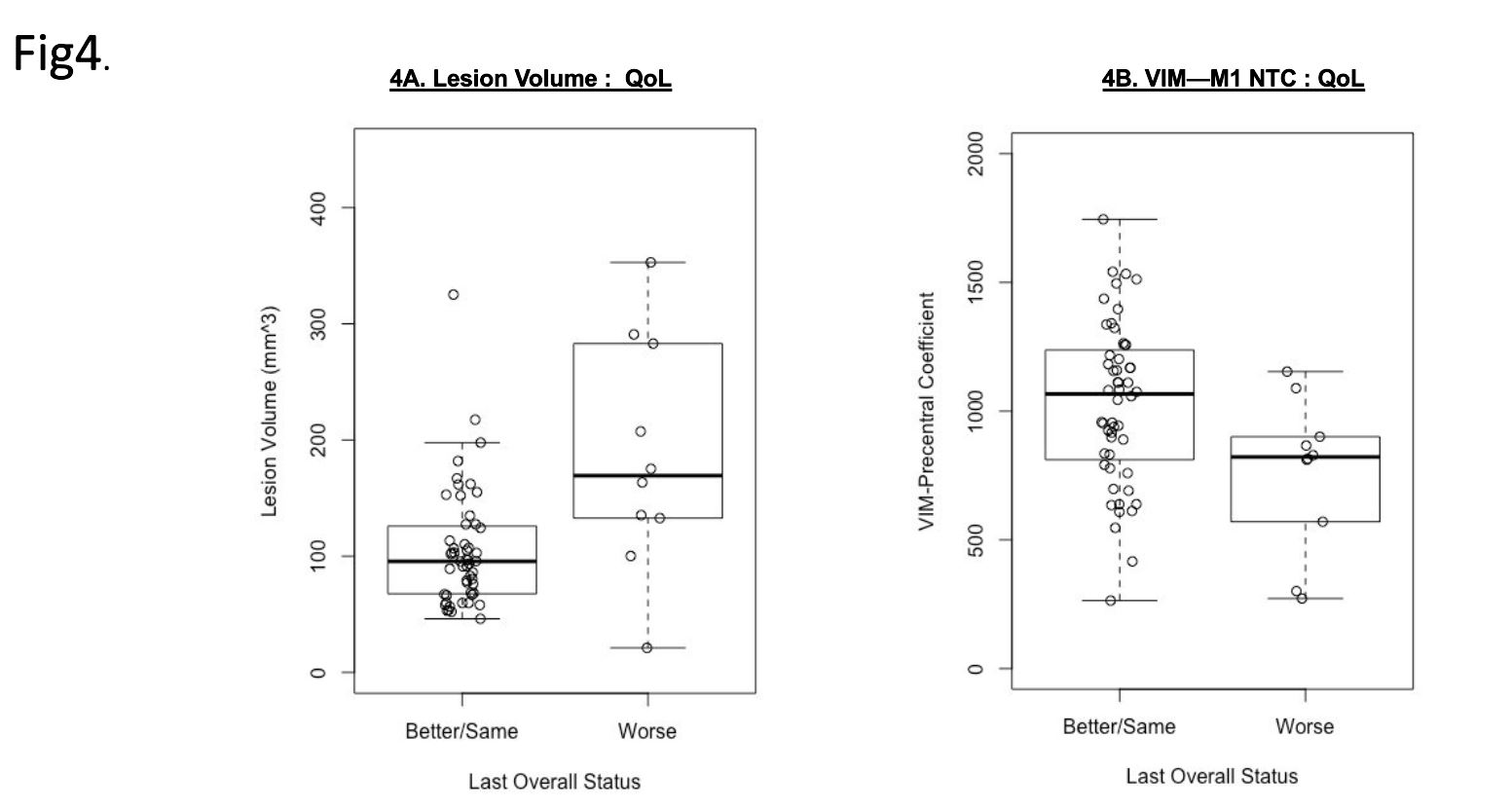
8) The “worse” versus “better/same" groups were compared for each of the variables of (i) Lesion-volume, and (ii) NTC. (Mann-Whitney)
Results
37 patients (59.7%) reported “better” QoL; 15 (24.2%) had “same” QoL; 10 (16.1%) reported “worse” QoL at latest follow-up (range 3-38mo; median 4.5 mo). All three groups had substantial tremor reduction which did not differ between the three groups (p=0.45076), therefore tremor reduction alone failed to predict QoL outcomes (Fig.3).The “worse” versus “better/same” QoL groups differed when comparing each variable: (i) lesion volume (U=109, p=0.0040), and (ii) lesion:VIM—M1 NTC (U=383, p=0.019)(Fig.4). Cutoff points for each variable were calculated from ROC-curve points that maximized YI (balancing sensitivity & specificity). The following thresholds correlated with better QoL outcomes: Lesion-volume <143mm3 (AUC 0.79, YI 0.41, Sensitivity 60%, Specificity 81%); VIM—M1 NTC >895.4 (AUC 0.77, YI 0.48, Sensitivity 69%, Specificity 80%).
Discussion
We observe that tremor reduction alone failed to predict QoL improvement after thalamotomy. Patients achieving substantial tremor improvement but who nevertheless had worsened QoL experienced postoperative side-effects that outweighed benefit experienced from tremor-reduction. The intuitive premise in functional stereotactic neurosurgery is that a tiny lesion precisely placed at a patient’s neuroanatomic target will best accomplish functional therapeutic goals with minimal side-effects. Nevertheless, despite the obvious limitations of the canonical method, lacking patient specificity and valuing larger lesions to achieve tremor reduction, it remains the standard MRgFUS thalamotomy technique. Our results indeed support the fundamental functional neurosurgical premise that ideally-targeted smaller lesions are associated with better QoL. In our study, the lesions that optimized QoL were smaller lesions that highly overlapped with patient-fit VIM—M1 normative tractography. These results suggest QoL optimized MRgFUS techniques may be accomplished by going beyond the decades old indirect canonical targeting technique, and instead using direct patient-fit combined atlas-based/normative-tractography methods to better guide smaller MRgFUS ablations.Conclusion
Beyond tremor-improvement alone, QoL post-MRgFUS for ET should be emphasized. Utilizing patient-specific thalamic-mapping techniques (i.e. patient-fit VIM—M1 normative-tractography) during MRgFUS planning could help optimize QoL outcomes. Invoking such patient-specific image-based targeting-techniques may also eventually facilitate patient-asleep MRgFUS, enabling more comfortable and efficient procedures while optimizing outcomes.Acknowledgements
No acknowledgement found.References
1. Elias WJ, Huss D, Voss T, et al. A pilot study of focused ultrasound thalamotomy for essential tremor. N Engl J Med. 2013;369(7):640-648.
2. Elias WJ, Lipsman N, Ondo WG, et al. A randomized trial of focused ultrasound thalamotomy for essential tremor. N Engl J Med. 2016;375(8):730-739.
3. Halpern CH, Santini V, Lipsman N, et al. Three-year follow-up of prospective trial of focused ultrasound thalamotomy for essential tremor. Neurology. 2019;93(24):e2284-e2293.
4. Tian Q, Wintermark M, Elias WJ, et al. Diffusion MRI tractography for improved transcranial MRI-guided focused ultrasound thalamotomy targeting for essential tremor. NeuroImage Clin. 2018;19:572-580.
5. Akram H, Dayal V, Mahlknecht P, et al. Connectivity derived thalamic segmentation in deep brain stimulation for tremor. NeuroImage Clin. 2018;18:130-142.
6. Ghanouni P, Pauly KB, Elias WJ, et al. Transcranial MRI-guided focused ultrasound: a review of the technologic and neurologic applications. Am J Roentgenol. 2015;205(1):150-159.
7. Kincses ZT, Szabó N, Valálik I, et al. Target identification for stereotactic thalamotomy using diffusion tractography. PloS One. 2012;7(1):e29969.
8. Yeh FC, Panesar S, Fernandes D, et al. Population-averaged atlas of the macroscale human structural connectome and its network topology. Neuroimage. 2018;178:57-68.
9. Ewert S, Plettig P, Li N, et al. Toward defining deep brain stimulation targets in MNI space: a subcortical atlas based on multimodal MRI, histology and structural connectivity. Neuroimage. 2018;170:271-282.
10. Makris N, Goldstein JM, Kennedy D, et al. Decreased volume of left and total anterior insular lobule in schizophrenia. Schizophr Res. 2006;83(2-3):155-171.
11. Frazier JA, Chiu S, Breeze JL, et al. Structural brain magnetic resonance imaging of limbic and thalamic volumes in pediatric bipolar disorder. Am J Psychiatry. 2005;162(7):1256-1265.
12. Desikan RS, Ségonne F, Fischl B, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. 2006;31(3):968-980.
13. Goldstein JM, Seidman LJ, Makris N, et al. Hypothalamic abnormalities in schizophrenia: sex effects and genetic vulnerability. Biol Psychiatry. 2007;61(8):935-945.
14. Jenkinson M, Beckmann CF, Behrens TE, Woolrich MW, Smith SM. Fsl. Neuroimage. 2012;62(2):782-790.
15. Smith SM, Jenkinson M, Woolrich MW, et al. Advances in functional and structural MR image analysis and implementation as FSL. Neuroimage. 2004;23:S208-S219.
16. Woolrich MW, Jbabdi S, Patenaude B, et al. Bayesian analysis of neuroimaging data in FSL. Neuroimage. 2009;45(1):S173-S186.
17. Avants BB, Tustison N, Song G. Advanced normalization tools (ANTS). Insight J. 2009;2(365):1-35.
18. Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: significantly improved efficiency and reliability. Neuroimage. 2006;31(3):1116-1128.
19. Wintermark M, Druzgal J, Huss DS, et al. Imaging findings in MR imaging–guided focused ultrasound treatment for patients with essential tremor. Am J Neuroradiol. 2014;35(5):891-896.Figures