0240
Computationally tractable high resolution non-rigid motion compensated 3D abdominal image reconstruction1Department of Radiotherapy, University Medical Center Utrecht, Utrecht, Netherlands, 2Computational Imaging Group for MR Therapy and Diagnostics, University Medical Center Utrecht, Utrecht, Netherlands
Synopsis
Respiratory and bulk organ motion remains a significant problem in abdominal 3D MRI. Motion compensated image reconstruction is a potential generic solution, but requires solving a large computational problem. In this work we propose to split the image reconstruction into sagittal planes to correct for the majority of respiratory and bulk organ motion. We demonstrate that the proposed method reconstructs high quality free-breathing T1 gradient echo images that are qualitatively comparable to breathhold scans. Future work will assess the feasibility of the method for dynamic contrast enhanced MRI and MR cholangiopancreatography.
Introduction
Respiratory motion remains a significant problem in abdominal 3D MRI examinations that leads to a large number of failed exams or unnecessary lengthy exams. To manage respiratory motion, current clinical protocols are often acquired with respiratory triggering or breathholds, which either have a low scanning efficiency, limit the maximal achievable spatial resolution and reduce patient comfort. Emerging methods to overcome these limitations include continuous acquisitions with motion-resolved image reconstructions1 and their extension to motion-compensated image reconstructions2.The quality of motion-compensated image reconstructions relies on the precision of the motion estimates, where previous works have shown that using up to 20 respiratory motion states can be beneficial3. However, motion-compensated image reconstruction necessitates the inclusion of 3D motion fields and therefore forms a large computational problem. In this work we propose to split the motion-compensated image reconstruction problem into multiple sagittal planes, where we assume the motion to be negligible in the left-right direction, to enable computational tractable reconstructions with a large number of motion states.
The three key innovations include: 1) The splitting of the respiratory motion compensation reconstruction problem in the sagittal plane, by positioning the readout direction in left-right interleaved with self-navigation in feet-head. 2) A dual density Cartesian spiral(CASPR)4 scheme with data driven sampling density estimation, which improves motion resolved image reconstructions. 3) The inclusion of both respiratory motion fields and bulk motion fields in the iterative image reconstruction. We show that the proposed motion-compensated imaging pipeline provides a computational tractable method reconstruct high resolution 3D abdominal images in free-breathing from a high number of motion states from respiratory and time-resolved dimensions.
Methods
Image acquisition: Two healthy volunteers were scanned on a 1.5T MR system (Philips Ingenia, Best, the Netherlands) with a 12 channel posterior and a 16 channel anterior receive coil. In both volunteers we acquired 3D T1 SPGR with CASPR sampling scheme in free breathing with readout direction left-right, except for the self-navigator which was rotated to feet-head(Fig.1-A). Relevant sequence parameters were FOV=350mm3,resolution=2mm3,TE/TR =1.6/3.6ms,FA=15° and scan time=200s. Code to generate the dual density CASPR sampling schemes is available here: https://github.com/tombruijnen/rscaspr. For comparison, a 3D T1 SPGR with an 18s breathhold with conventional cartesian sampling (Compressed sense factor=4), was acquired. In addition we acquired coronal/sagittal cine scans (1 min, same sequence parameters) to validate the motion estimates.Image reconstruction: Prior to the scans a coil sensitivity reference scan was acquired and the multi-channel projections were used for self-navigation. The k-space data were retrospectively reordered across 20 respiratory phases using soft-weighted amplitude binning5 and reconstructed using XD-GRASP($$$\in\!C^{x\cdot\,y\cdot\,z\cdot\,20}$$$)(eq.1) with the BART toolbox6. The images were non-rigidly registered with optical flow7 and the resulting motion fields were truncated to one singular rank and made inverse consistent. The motion fields were subsequently used for three different type of reconstructions. 1)Respiratory motion compensated image reconstruction (RESP-MOCO$$$\in\!C^{x\cdot\,y\cdot\,z}$$$) (eq.2); 2)Respiratory motion compensated dynamic image reconstructions(RESP-MOCO-4D$$$\in\!C^{x\cdot\,y\cdot\,z\cdot\,20}$$$)(eq.1); 3) Respiratory and dynamic motion compensated image reconstructions(RESP-DYN-MOCO$$$\in\!C^{x\cdot\,y\cdot\,z}$$$)(eq.2):
$$x_t=\min\limits_{x_t}\;||FSU^Hx_t - y||_2+\lambda_t||TV x_t||_1,\;eq(1)$$
$$x\;=\min\limits_{x}\;||FSU^Hx - y||_2+\lambda_w||\Psi x||_1,\;eq(2)$$
With Fourier operator(F), coil operator(S), motion operator(U), exhale image(x), k-space data(y), wavelet transform($$$\Psi$$$) and temporal-finite-difference operator(TV). The optimization problem was solved with L-BFGS in Matlab on a GPU8.
Experiments: The coronal 2D cine scan was used to quantify the left-right motion in two regions of interest using template matching. The sagittal 2D cine scan was used to determine a cut-off frequency for the dual density CASPR scheme to oversample the k-space that change most due to motion. The sagittal 2D cine scan was compared to the respiratory resolved 4D-MRIs. Finally, multiple image reconstruction strategies were qualitatively compared to the breathhold acquisition.
Results and discussion
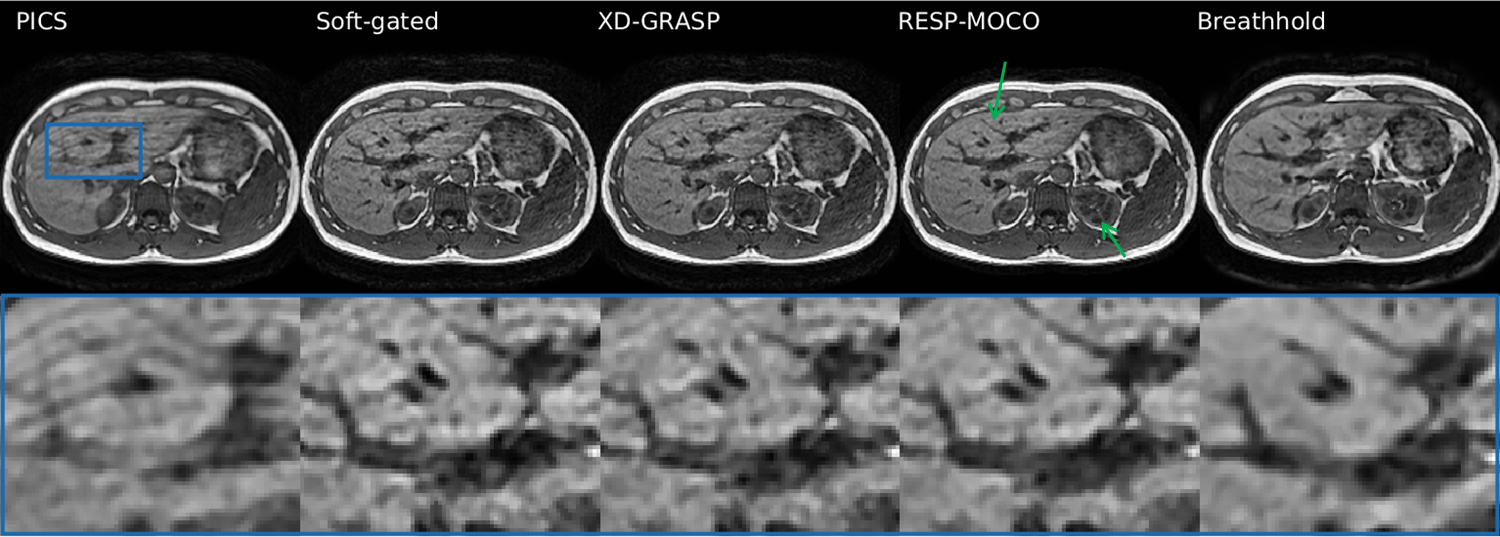
Fig.1.B-C shows the template matching result of the coronal 2D cine scan, where maximum left-right motion is <3mm for both features and feet-head motion >20mm. Fig.2.A-B shows the sagittal 2D cine scan and the corresponding temporal standard deviation of the coil combined k-space, which was compressed to a radial spectrum plot (Fig.2.C). Here a 70% cut-off frequency was (1cm resolution) was selected as the dual density CASPR low-resolution region. Fig.3 shows two slices of the respiratory resolved 2D cine versus the 4D CASPR. The third column shows the RESP-MOCO-4D reconstruction that visualizes residual dynamics. Fig.4 shows the comparison of the different respiratory motion compensated image reconstruction techniques versus the single breathhold acquisition. Note that RESP-MOCO shows a reduction in aliasing artefacts compared to soft-gated PICS/XD-GRASP. Fig.5 shows the comparison of RESP-MOCO vs RESP-DYN-MOCO. Note that RESP-DYN-MOCO slows slightly sharper edges in the zoom image compared to RESP-MOCO. However, further not all motion is corrected due to through-plane effects. Reconstruction times per slice were <1s for PICS/soft-gated PICS, <10s for XD-GRASP, <20s for RESP-MOCO and <2min for RESP-MOCO-4D & RESP-DYN-MOCO.Conclusion and future work
In this work we proposed a novel non-rigid motion compensated imaging pipeline that offers computational advantages that allows the inclusion of high dimensional motion information for high quality image reconstructions to compete with breathhold acquisitions. In addition, the proposed methods provides means to simultaneously study respiratory and gastro-intestinal motion. In future work we will evaluate the proposed method for dynamic contrast enhanced liver MRI, respiratory-resolved 4D-MRI for radiotherapy treatment planning and extend the proposed method to T2-weighted 3D turbo spin echo9 for magnetic resonance cholangio-pancreatography10.Acknowledgements
No acknowledgement found.References
1 Feng, L., Axel, L., Chandarana, H., Block, K. T., Sodickson, D. K., & Otazo, R. (2016). XD-GRASP: Golden-angle radial MRI with reconstruction of extra motion-state dimensions using compressed sensing. Magnetic Resonance in Medicine, 75(2), 775–788. https://doi.org/10.1002/mrm.25665
2 Batchelor, P. G., Atkinson, D., Irarrazaval, P., Hill, D. L. G., Hajnal, J., & Larkman, D. (2005). Matrix description of general motion correction applied to multishot images. Magnetic Resonance in Medicine, 54(5), 1273–1280. https://doi.org/10.1002/mrm.20656
3 Rank, C. M., Heußer, T., Buzan, M. T. A., Wetscherek, A., Freitag, M. T., Dinkel, J., & Kachelrieß, M. (2017). 4D respiratory motion-compensated image reconstruction of free-breathing radial MR data with very high undersampling. Magnetic Resonance in Medicine, 77(3), 1170–1183. https://doi.org/10.1002/mrm.26206
4 Prieto, C., Doneva, M., Usman, M., Henningsson, M., Greil, G., Schaeffter, T., & Botnar, R. M. (2015). Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. Journal of Magnetic Resonance Imaging, 41(3), 738–746. https://doi.org/10.1002/jmri.24602
5 Zhang, T., Cheng, J. Y., Potnick, A. G., Barth, R. A., Alley, M. T., Uecker, M., Lustig, M., Pauly, J. M., & Vasanawala, S. S. (2015). Fast pediatric 3D free-breathing abdominal dynamic contrast enhanced MRI with high spatiotemporal resolution. Journal of Magnetic Resonance Imaging, 41(2), 460–473. https://doi.org/10.1002/jmri.24551
6 Uecker, M., Ong, F., Tamir, J. I., Bahri, D., Virtue, P., Cheng, J., Zhang, T., & Lustig, M. (2015). Berkeley Advanced Reconstruction Tools. Proc. Intl. Soc. Mag. Reson. Med., 73(2), 828–842. https://doi.org/10.5281/zenodo.12495
7 Zachiu, C., Papadakis, N., Ries, M., Moonen, C., & Denis De Senneville, B. (2015). An improved optical flow tracking technique for real-time MR-guided beam therapies in moving organs. Physics in Medicine and Biology, 60(23), 9003–9029. https://doi.org/10.1088/0031-9155/60/23/9003
8 Becker, S. (2019). L-BFGS-B, converted from Fortran to C, with Matlab wrapper. https://github.com/stephenbeckr/L-BFGS-B-C
9 Bruijnen T, Schakel T, Akdag O, Bruel C V M and Lagendijk J J W 2020 in ‘Proc. ISMRM 28’
10 Bruijnen T, Schakel T, Lagendijk J, Geerts L, Johannes P, Blanken N, Veldhuis W and van den Berg,CAT, 2021 in Proc. ISMRM 29
Figures