0148
The diagnostic performance of modified BI-RADS using high-resolution diffusion weighted images (HR-DWI), T1WI and T2WI1Department of Diagnostic Imaging and Nuclear Medicine, Kyoto University graduate school of medicine, Kyoto, Japan, 2Department of Diagnostic Radiology, Kyoto Katsura Hospital, Kyoto, Japan, 3Department of Diagnostic Radiology, Kansai Electric Power Hospital, Osaka, Japan, 4Department of Diagnostic Pathology, Kyoto University Hospital, Kyoto, Japan, 5Department of Breast Surgery, Kyoto University Hospital, Kyoto, Japan
Synopsis
This study aimed to evaluate the diagnostic performance of non-contrast protocol combining high-resolution diffusion weighted images (HR-DWI) with rs-EPI, T1WI and T2WI, using modified BI-RADS. In total, 98 breast lesions (60 malignant and 38 benign lesions) were categorized and compared to the pathological diagnosis. Area under the ROC curve (AUC)s of the non-contrast protocol were 0.90 (95% confidence interval (95%CI) : 0.82-0.95) for both readers. When excluding cases in which ADC value could not be measured, the AUC values were improved. Non-contrast protocol with modified BI-RADS can be used to evaluate breast lesions.
Introduction:
High-resolution DWI (HR-DWI) using rs-EPI (abbreviated as HR-DWI hereafter) demonstrated excellent agreement with DCE-MRI in morphology and lesion extent [1, 2]. This evidence implies the potential use of BI-RADS based descriptors for non-contrast MRI. However, HR-DWI alone may not be sufficient to achieve reasonable diagnostic performance. Adding information from other non-contrast sequences may be useful [3]. The purpose of this study is to evaluate the diagnostic performance of non-contrast protocol combining HR-DWI, T1WI and T2WI, using modified BI-RADS 2013-based assessment (Modified BI-RADS).Materials & Methods:
Study populationStudy population consisted of 98 females (mean age 56, range 20–87 years old) with 108 lesions (pathologically confirmed as 63 malignant and 45 benign lesions) who were scanned with MRI including HR-DWI from April 2017 and September 2019. Lesions for which ADC values could not be measured were excluded (n=10), leaving 98 lesions (60 malignant and 38 benign) for final analysis.
MRI protocol
A 3T MRI system (MAGNETOM Prisma: Siemens Healthcare, Erlangen, Germany) with a dedicated 18-channel breast coil was used for image acquisition. Our routine protocol for breast lesions included fat-suppressed (FS) T1-weighted images (T1WI), T2-weighted images (T2WI), HR-DWI using rs-EPI. Apparent diffusion coefficient (ADC) maps were automatically created from DWI at b = 0 and 850 s/mm2.
Image analysis
Modified BI-RADS with decision tree
Based on previous studies [4], a diagnostic decision tree was constructed using imaging findings of T1WI/T2WI and HR-DWI (Figure 1) to categorize the lesions into 5 categories. Category 4 lesions were subclassified into three subcategories 4A, 4B and 4C depending on the likelihood of malignancy. Two experienced readers, blinded to the final pathological diagnosis, independently categorized the lesions according to modified BI-RADS with diagnostic decision tree. One rank higher category (or subcategories) is allocated if the lesion showed “Large size”, ”low ADC value” ,edema (high signal intensity on T2WI), and a few other associated features suggesting malignancy listed in figure 1. The lesions were categorized as category 2, 3, 4A, 4B, 4C and 5. If the lesion could not be recognized, the lesion was classified as Category 1. Category 5 and 4C are grouped as malignant and category 2, 3, 4A and 4B as benign, and these groups were compared with pathological diagnosis.
ADC measurement
Both readers measured the values on ADC maps by placing a maximum of three regions of interest (ROI) of 3mm on each lesion. ADC values were calculated only from the lesions in which ROIs could be placed. In each ROI, the average ADC values were calculated and the lowest of the average ADC values was used as the representative ADC value in each lesion.
Statistical analysis
The diagnostic performance of modified BI-RADS in discriminating benign and malignant lesions was assessed using a receiver operating characteristic (ROC) analysis. The ADCs of the benign and malignant lesions were compared using a Mann-Whitney test.
Results:
The modified BI-RDAS categories of the two readers were in agreement for 60 lesions (54.1%) with a kappa value of 0.65 (95% confidence interval (95%CI): 0.57–0.73), suggesting substantial agreement.A statistically significant difference of the mean ADC value was observed between the malignant and the benign lesions for both readers (p < 0.001). ROC analysis showed an area under the ROC curve (AUC) of 0.90 (95% CI: 0.82-0.95) for both readers (Figure 2). The sensitivity and specificity were 83.3% and 86.8% for reader 1, 75.0% and 92.1% for reader 2, respectively.
Images of representative cases were shown in Case 1 (malignant lesion) and 2 (benign lesion).
Discussion & Conclusion:
Combining DWI, T1/T2WI, and ADC values provides increased accuracy for differentiation between benign and malignant lesions, comparable to the accuracy with DCE-MRI[5]. The strengths of the current analysis can be the use of high-resolution DWI that enabled detailed morphological evaluation of malignant lesions. Among associated features, lesion size and ADC values were proved to be useful features. In addition, edema on T2WI contributed to the diagnosis of malignancy. Another strength is the use of decision tree that helped in summarizing these key findings to predict the probability of malignancy, as well as clarifying diagnostic process.The drawback of the current method is the exclusion of lesions with difficulty in measuring ADC value or even difficulty in detection. In that sense, accurate diagnoses for small and non-mass lesions are challenging with non-contrast protocol. Further development of HR-DWI allowing the ADC measurement of these challenging lesions is awaited. In conclusion, non-contrast protocol including HR-DWI, T1/T2WI with modified BI-RADS and decision tree can be used to evaluate breast lesions with excellent diagnostic performance.
Acknowledgements
No acknowledgment was found.References
- Kishimoto, A.O., et al., The comparison of high-resolution diffusion weighted imaging (DWI) with high-resolution contrast-enhanced MRI in the evaluation of breast cancers. Magn Reson Imaging, 2020. 71: p. 161-169.
- Kishimoto, A.O., et al., Evaluation of Malignant Breast Lesions Using High-resolution Readout-segmented Diffusion-weighted Echo-planar Imaging: Comparison with Pathology. Magn Reson Med Sci, 2021. 20(2): p. 204-215.
- Trimboli, R.M., et al., Breast cancer detection using double reading of unenhanced MRI including T1-weighted, T2-weighted STIR, and diffusion-weighted imaging: a proof of concept study. AJR Am J Roentgenol, 2014. 203(3): p. 674-81.
- Lee, S.H., H.J. Shin, and W.K. Moon, Diffusion-Weighted Magnetic Resonance Imaging of the Breast: Standardization of Image Acquisition and Interpretation. Korean J Radiol, 2021. 22(1): p. 9-22.
- Kim, K.W., et al., Diagnostic Usefulness of Combination of Diffusion-weighted Imaging and T2WI, Including Apparent Diffusion Coefficient in Breast Lesions: Assessment of Histologic Grade. Acad Radiol, 2018. 25(5): p. 643-652.
Figures
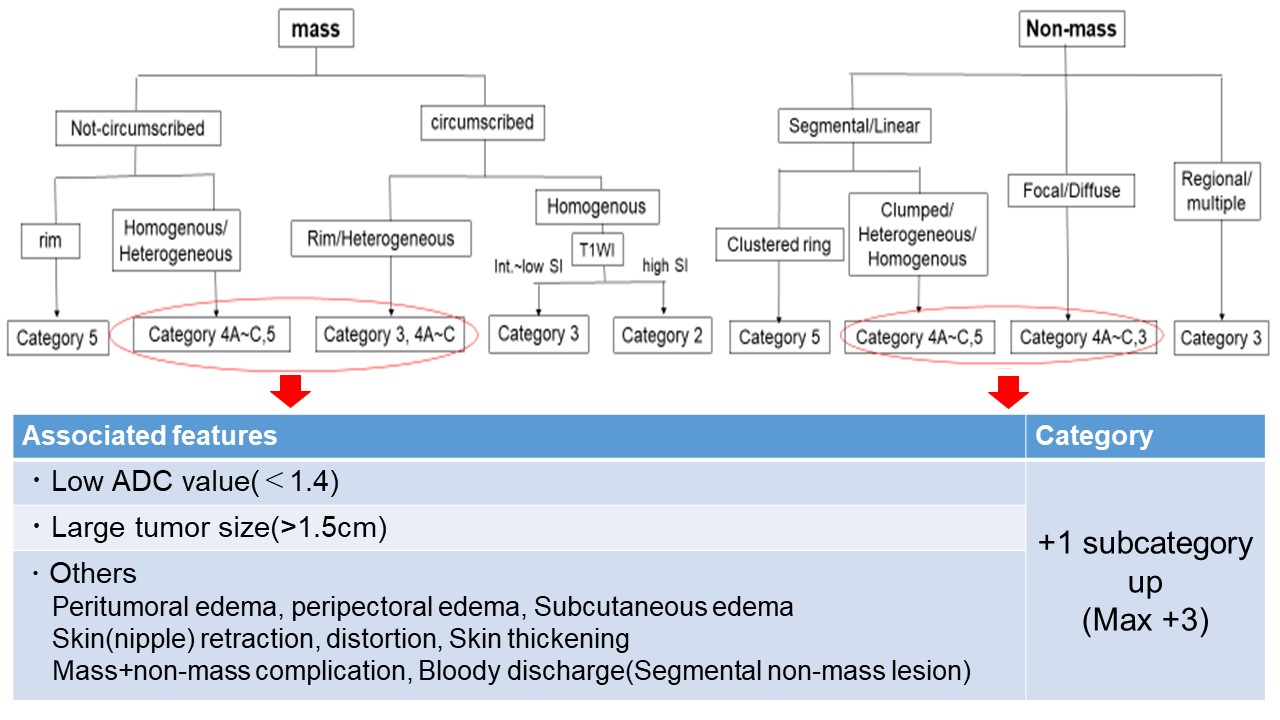
Figure1. The decision tree for mass and non-mass lesions
The diagnostic decision tree was constructed with combining diagnostic criteria based on BI-RADS (the lesion morphology including margins, distribution) with signal intensity and ADC value obtained from HR-DWI. The decision tree is designed to categorize lesions into detailed assessment categories/subcategories (Category 2, 3, 4A, 4B, 4C and 5). Associated features including “large size”, “low ADC value” , “edema” and other findings indicate malignancy and are used to rank up one subcategory.
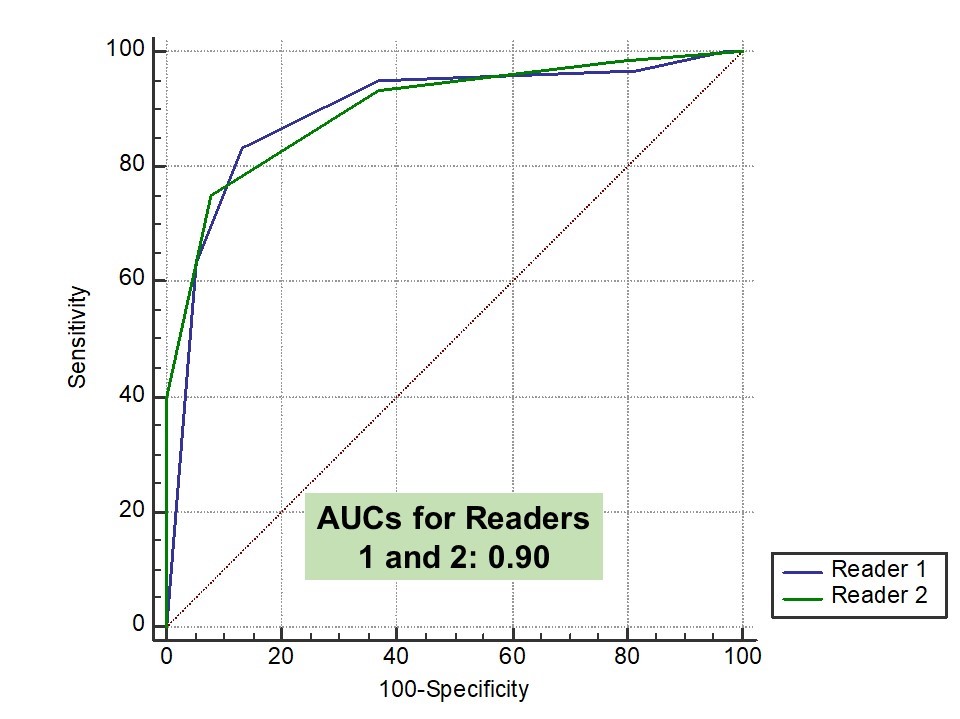
Figure 2. Comparison of ROC curve between Readers 1 and 2 based on results from 98 lesions.
AUCs were 0.9 (95% CI: 0.82-0.95) for both readers, with almost the same ROC curve.
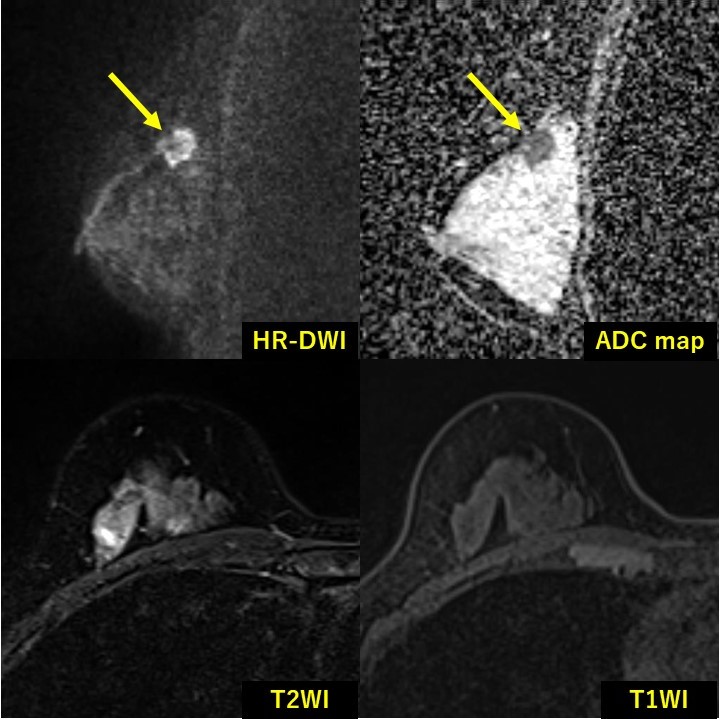
Case 1. (a representative case of malignant lesion)
A 62-year old woman with invasive carcinomas of no special type (NST). A mass with not-circumscribed margin is shown. Rim shape can be appreciated on HR-DWI. According to the decision tree, the lesion is classified as Category 5.
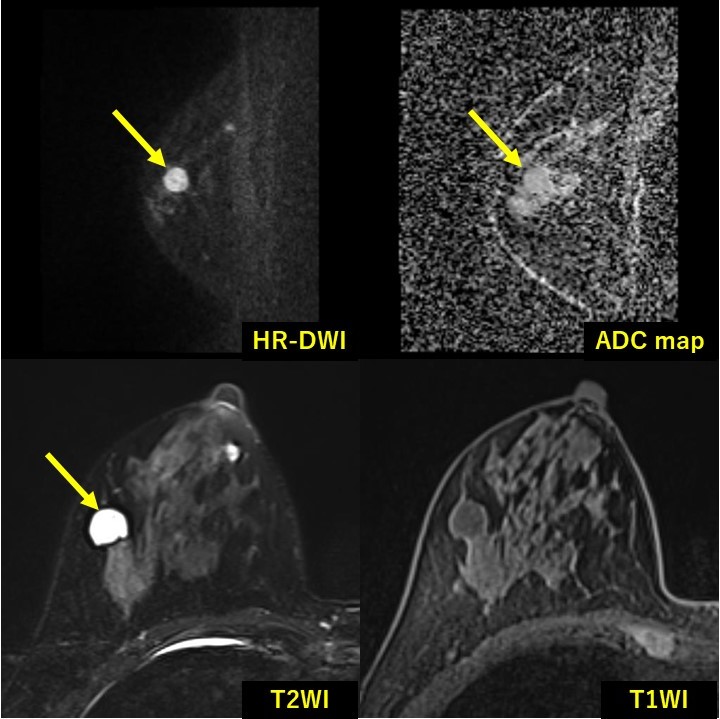
Case 2. (a representative case of benign lesion)
A 76-year old woman with fibroadenoma. A mass with circumscribed margin is shown. According to the proposed decision tree, the lesion is classified as Category 3.