0095
Accelerated High-Resolution 3D Isotropic Wrist MRI at 7 Tesla: Compressed Sensing vs. SENSE
Bobby Runderkamp1, Matthan Caan2, Wietske van der Zwaag3, Robert Hemke1, Mario Maas1, Mads Andersen4,5, Gustav Strijkers2, Karin Markenroth Bloch4, and Aart Nederveen1
1Radiology & Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 2Biomedical Engineering and Physics, Amsterdam UMC, Amsterdam, Netherlands, 3Spinoza Center for Neuroimaging, Amsterdam, Netherlands, 4Lund University Bioimaging Center, Lund, Sweden, 5Philips Healthcare, Copenhagen, Denmark
1Radiology & Nuclear Medicine, Amsterdam UMC, Amsterdam, Netherlands, 2Biomedical Engineering and Physics, Amsterdam UMC, Amsterdam, Netherlands, 3Spinoza Center for Neuroimaging, Amsterdam, Netherlands, 4Lund University Bioimaging Center, Lund, Sweden, 5Philips Healthcare, Copenhagen, Denmark
Synopsis
Imaging of the intricate arrangement of small structures in the wrist benefits from high resolution imaging, which the increased SNR at 7 Tesla can enable. However, the increased resolution requires longer scan times, decreasing patient comfort and increasing risk of motion artifacts. In this work, we evaluated compressed sensing (CS) acceleration of a clinical wrist 7T MRI protocol, 0.45mm isotropic resolution, in comparison to SENSE-acceleration. We show that CS-acceleration can produce adequate to good image quality in significantly shorter scan times, not achievable by increasing SENSE-acceleration.
Introduction
The human wrist is composed of an intricate arrangement of interdependent small structures. Among these are ligaments, cartilage and the triangular fibrocartilage complex (TFCC). Reliable evaluation of these structures are of great importance for diagnosis and clinical decision making, but is often difficult and can require invasive arthroscopy. Due to the complex anatomy and small size of these wrist structures, diagnostics may greatly benefit from the high-resolution imaging possible at 7T thanks to increased SNR. However, with increasing resolution the scan duration increases rapidly, decreasing patient comfort and increasing the risk of motion artifacts. Scan acceleration is therefore highly desired. A clinically relevant MRI acquisition for diagnosing wrist injuries at all field strengths is a 3D proton density-weighted TSE with SPAIR fat suppression1. Here, we evaluated compressed sensing2 acceleration of a clinical wrist 7T MRI protocol with and without fat-suppression in comparison to standard SENSE-acceleration.Methods
All MRI scans were performed with a 7T Philips Achieva scanner (Philips, Best, The Netherlands) using a 1Tx/16Rx wrist coil (RAPID Biomedical GmbH, Rimpar, Germany). Thirteen healthy volunteers were included in the study after providing written informed consent. The clinical 7T 3D PD-w TSE protocol used as reference had isotropic spatial resolution of 0.45mm and was accelerated with SENSE-factors 2.2x2.0, giving a scan duration of 7:07 minutes (‘SENSE0.45’). To compare the SENSE0.45 scan, the scan protocol included two compressed sensing (CS) scans, performed using the in-house developed PROUD technique allowing sparse acquisitions3,4. Compared to the reference SENSE0.45 scan, the first compressed sensing scan (‘CS0.45’) had equal resolution but additional acceleration, leading to a scan duration of 4:05 (43% scan time reduction), and the second (‘CS0.35’) had equal scan duration but an increased resolution of 0.35mm isotropic. To keep the TSE shot duration constant, the TSE factor was decreased in CS0.35 with respect to CS0.45 and SENSE0.45. For all scans, versions with and without SPAIR fat suppression were performed. The undersampling patterns used in the CS scans and additional scan parameters are shown in Figure 1. Both undersampling patterns contain a 25x25 sized fully sampled center square which was used to estimate receive coil sensitivity maps5 using the Berkeley Advanced Reconstruction Toolbox (BART)6. All CS reconstructions were performed using the PICS algorithm from BART and MRecon (Gyrotools, Zurich, Switzerland) in MATLAB (R2016a, The MathWorks Inc.). Regularization parameter optimization was performed heuristically. For the SENSE-scans, the vendor online reconstruction was used. Finally, a variation of SENSE0.45 was performed using a higher SENSE-acceleration of 3.0x2.6 (‘High-SENSE’). This had the same scan duration as CS0.45, 4:05 minutes. To assess image quality quantitatively, a radiologist performed blinded scoring of visibility of twelve wrist structures for the SPAIR scans: triangular fibrocartilage complex (TFCC, radial, ulnar and foveal attachment), scapholunate and lunotriquetral ligament (SLL/LTL, dorsal and palmar portion), bone trabeculae, articular cartilage, extensor carpi ulnaris (ECU) tendon and median and ulnar nerve. Additionally, images were scored on SNR, edge sharpness, perceived tissue contrast and artifact absence. In scoring, a 1 to 5 Likert scale was used.Results
Figure 2 shows SPAIR images of one volunteer. The high quality in the SENSE0.45 scan was consistent over individuals, as confirmed by the average scores in Figure 3. The CS0.45 scan shows some blurring compared to SENSE0.45, but structures are still well visible and CS0.45 scores adequate to good (3-4) for all parameters except bone trabeculae. Although CS0.35 has a higher isotropic resolution in preserved scan time, this did not translate into consistently improved visibility compared to SENSE0.45 and CS0.45. Figure 4 shows non-SPAIR images for all scan types. The High-SENSE scan shows considerable SENSE-artifacts.Discussion
Good to excellent visibility of nearly all investigated wrist structures could be obtained using a SENSE-factor of 2.2x2.0 in a 0.45mm isotropic 3D PDw SPAIR TSE scan. The CS0.45 scan reduced the scan time with 43% and retained an adequate to good image quality. Future studies will evaluate if diagnostic accuracy can be preserved using CS0.45 instead of SENSE0.45. For the SPAIR scans, CS0.35 did not outperform SENSE0.45. Visibility of bone trabeculae was scored lower for CS SPAIR scans. However, the non-SPAIR scans might be more suited for evaluation of bone structure. It is also clear that using higher SENSE-factors to obtain the same scan time reduction as with CS0.45 is not possible due to severe SENSE-artifacts. Future work will be focused on further improvement of the moderate image quality in CS-scans, with candidates of causing this being motion, a difference between vendor online and MRecon offline reconstruction and a difference in k-space trajectory between SENSE and CS.Conclusion
Compressed sensing was successfully applied to high-resolution 3D TSE SPAIR PD-weighted MRI at 7T to further shorten SENSE-accelerated scans by 43% while still obtaining adequate to good wrist structure visibility.Acknowledgements
The National 7T facility at Lund University Bioimaging Center is acknowledged for providing experimental resources.References
- Götestrand S, Björkman A, Björkman-Burtscher IM, Kristiansson I, Aksyuk E, Szaro P, Markenroth Bloch K, Geijer M. Visualization of wrist anatomy – a comparison between 7T and 3T MRI. Eur Radiol. 2021 Aug 11. doi: 10.1007/s00330-021-08165-5. Epub ahead of print. PMID: 34378077.
- Lustig M, Donoho D, Pauly JM. Sparse MRI: The Application of Compressed Sensing for Rapid MR Imaging. Magn Reson Med. 2007;58:1182-1195. doi: 10.1002/mrm.21391.
- Peper ES, Gottwald LM, Zhang Q, Coolen BF, van Ooij P, Strijkers GJ, Nederveen AJ. 30 times accelerated 4D flow MRI in the carotids using a Pseudo Spiral Cartesian acquisition and a Total Variation constrained Compressed Sensing reconstruction. Proceedings of the 27rd Annual Meeting ISMRM, 2018;Paris, France.
- Gottwald LM, Peper ES, Zhang Q, Coolen BF, Strijkers GJ, Planken RN, Nederveen AJ, van Ooij P. Pseudo Spiral Compressed Sensing for Aortic 4D flow MRI: a Comparison with k-t Principal Component Analysis. Proceedings of the 27rd Annual Meeting ISMRM, 2018;Paris, France.
- McKenzie CA, Yeh EN, Ohliger MA, Price MD, Sodickson DK. Self-Calibrating Parallel Imaging With Automatic Coil Sensitivity Extraction. Magn Reson Med. 2002;47:529-538. doi: 10.1002/mrm.10087.
- Uecker M. Berkeley Advanced Reconstruction Toolbox Target Audience: 2015;163(1991):25176. doi:10.1002/mrm.25176.
Figures
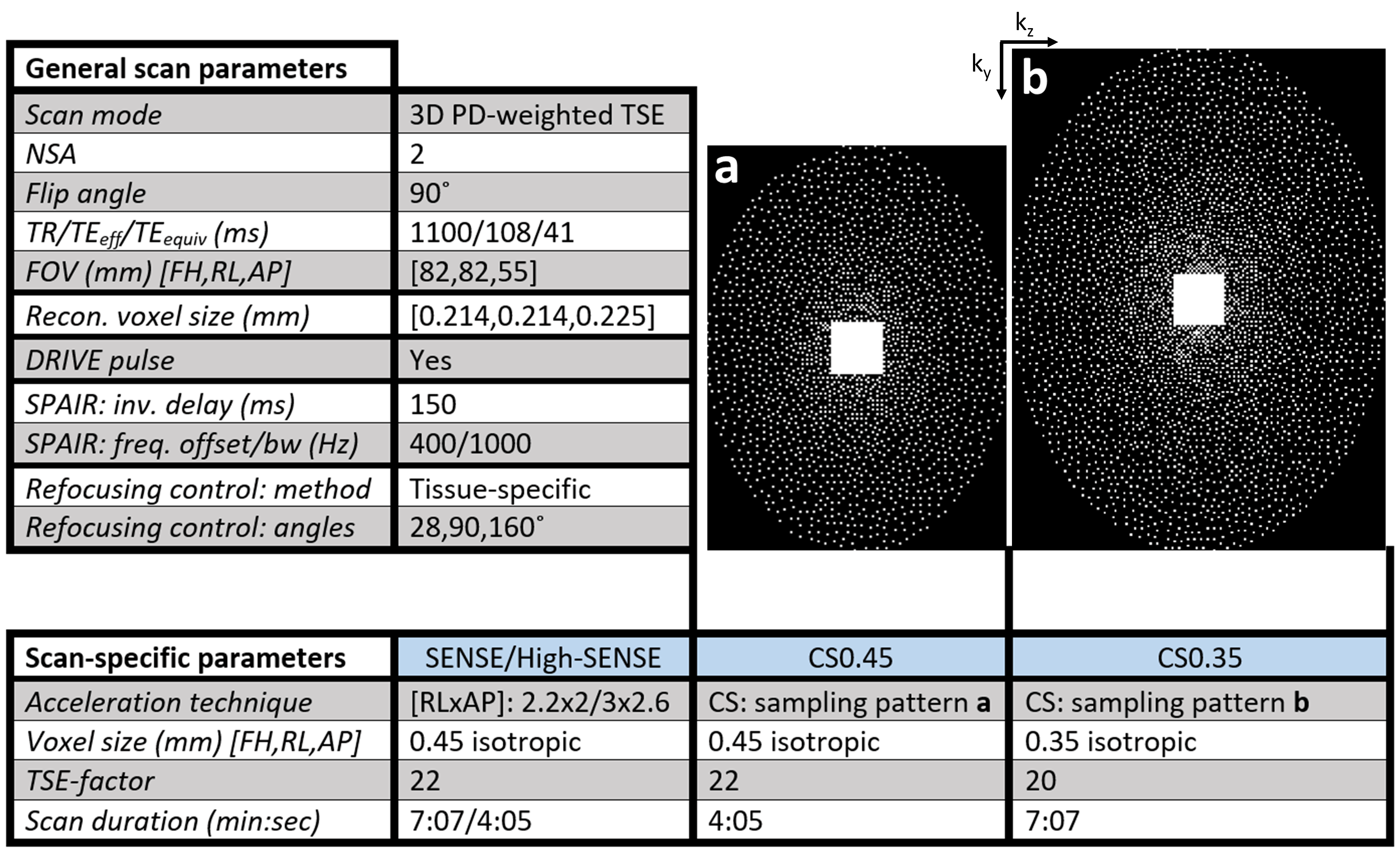
Figure 1. General scan parameters and scan parameters specific to the four different scans performed. a) and b) show the k-space undersampling pattern for CS0.45 and CS0.35 respectively. Both patterns are variable density Poisson disks, containing a fully sampled center square with size 25x25 used for reception coil sensitivity estimation. An elliptical k-space shutter was used.
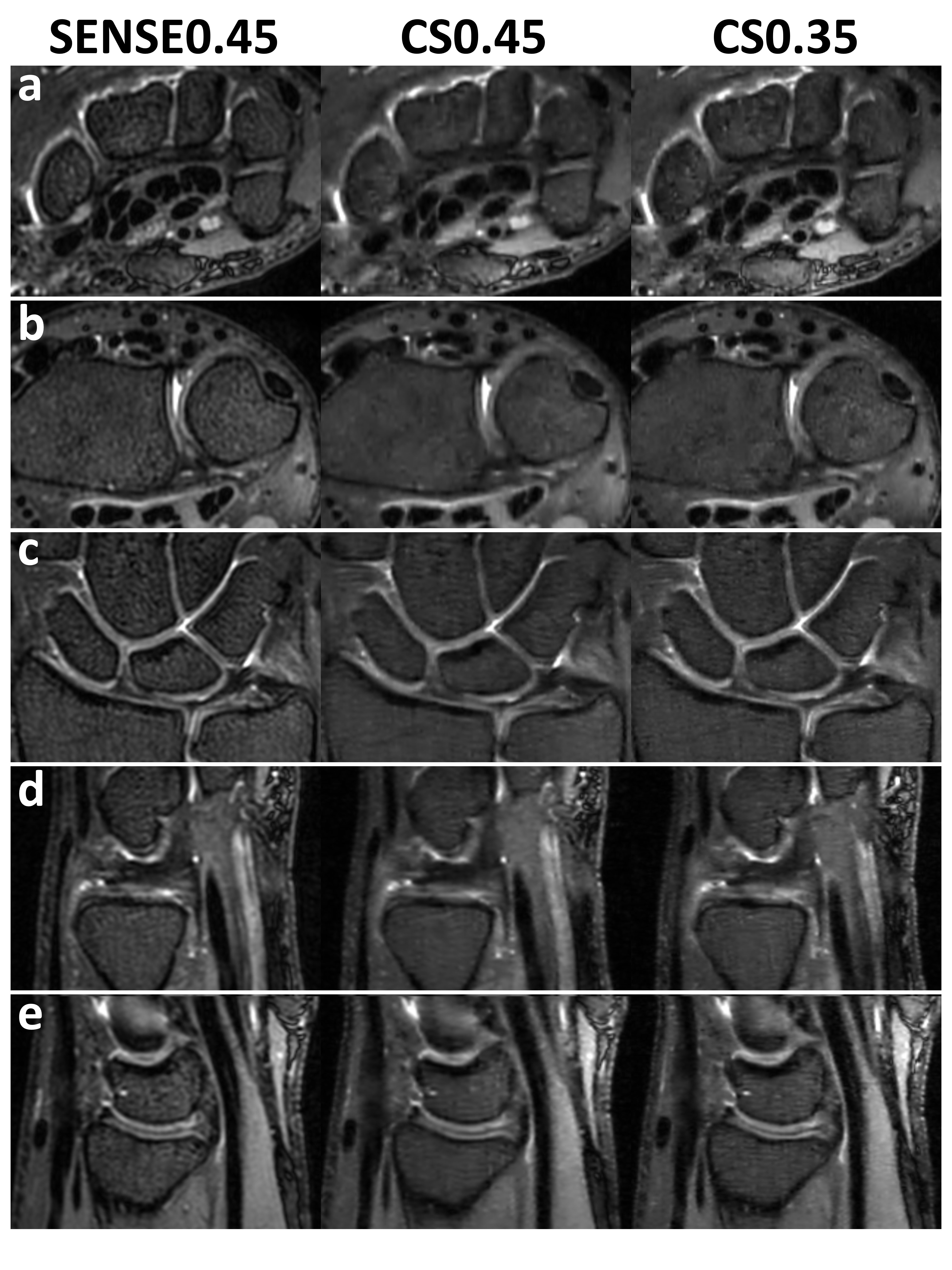
Figure 2. SPAIR magnitude images of SENSE0.45, CS0.45 and CS0.35 in one volunteer. Slices are centered on the following wrist structures: a) median and ulnar nerves at the level of the pisiform bone (carpal tunnel, axial), b) ECU tendon at the dorsal groove of the ulnar head (axial), c) TFCC and articular cartilage (coronal), d) TFCC (sagittal) and e) cartilage between the radius and lunate (sagittal).
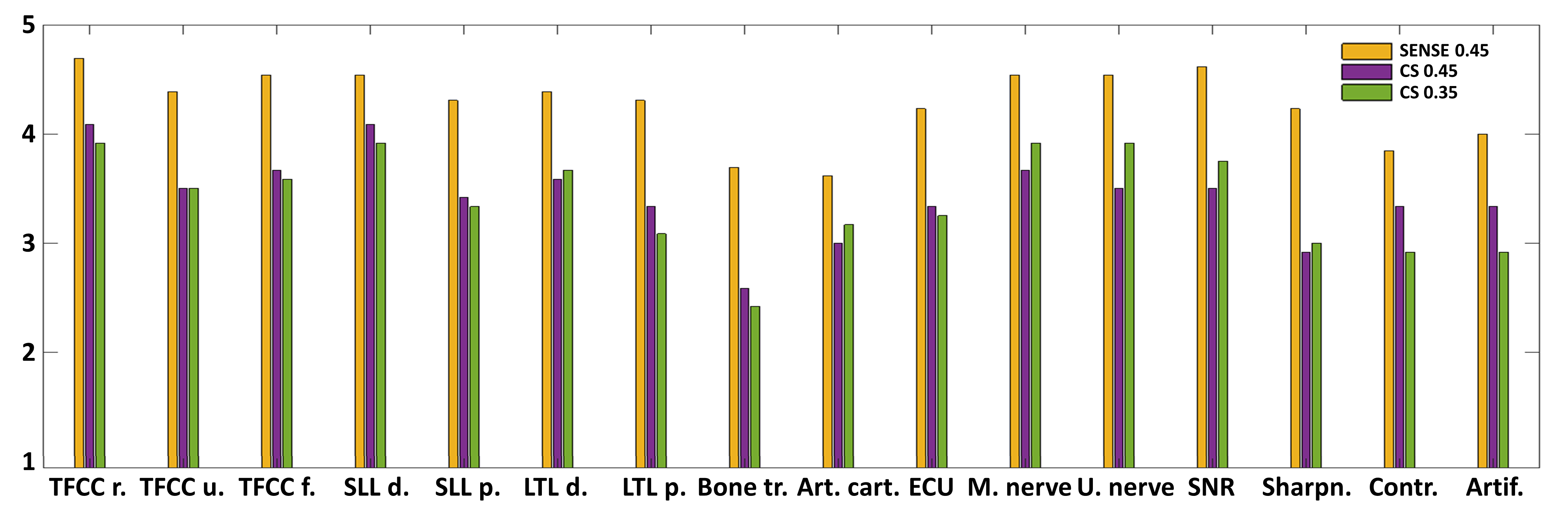
Figure 3. Radiologist Likert scores of the SENSE0.45 (yellow), CS0.45 (purple) and CS0.35 (green) SPAIR scans, averaged over all thirteen volunteers. Scores were given on visibility of twelve wrist structures and four image quality measures, mentioned in the Methods section. While SENSE0.45 shows a visibility of good to excellent for nearly all structures, CS0.45 and CS0.35 consistently score 1 scale point lower, but still have scores of adequate to good.
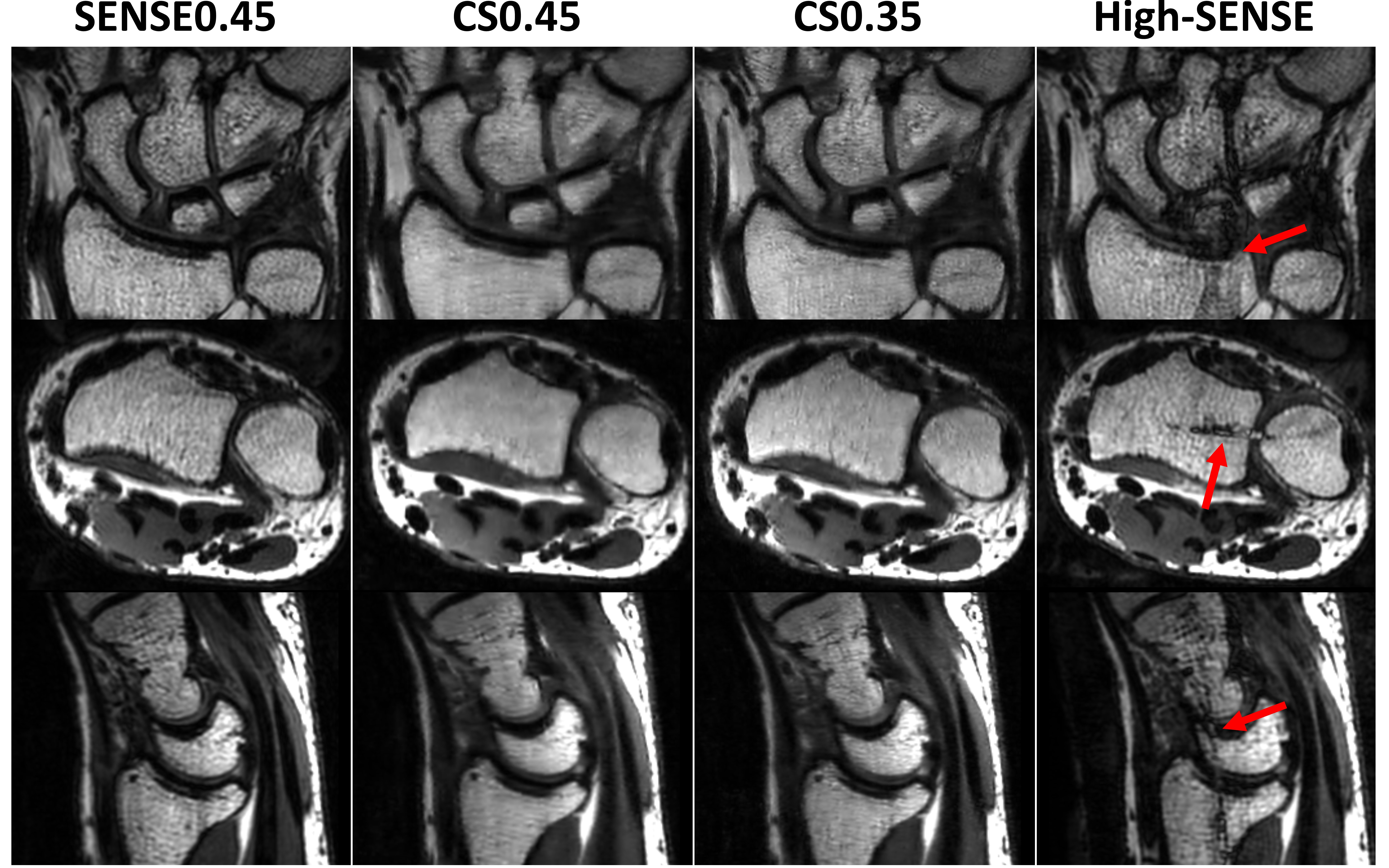
Figure 4. Non-SPAIR images of SENSE0.45, CS0.45, CS0.35 and High-SENSE in three orientations showing bone structure. The High-SENSE scan shows detrimental SENSE-artifacts (red arrows), while the equally long CS0.45 scan shows satisfactory image quality. An inhomogeneous fat signal distribution can be observed in all scans.
DOI: https://doi.org/10.58530/2022/0095