0094
Extended and weight bearing wrist MRI using a positioning apparatus and flexible glove coil to explore the cause of dorsal pain1Bernard and Irene Schwartz Center for Biomedical Imaging, Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 2Center for Advanced Imaging Innovation and Research (CAI2R), Department of Radiology, New York University Grossman School of Medicine, New York, NY, United States, 3Department of Orthopedic Surgery, New York University Grossman School of Medicine, New York, NY, United States
Synopsis
Dorsal wrist pain during extension or weight bearing is a common symptom, the etiology of which often remains unclear. Clinical MRI often fails to reveal causative pathology in part because it is performed in the neutral position. We built an apparatus to guide motion and used a flexible coil to capture signal in a range of positions that better match the conditions during which pain is reported. Results in nine asymptomatic volunteers show excellent tissue structure delineation, strong measurement agreement among readers, and increases in dorsal capsule thickness and radiocapitate, radiolunate, capitolunate and extensor tendon angulation during weight bearing.
Introduction
Dorsal wrist pain during extension or weight bearing is a common symptom, the etiology of which often remains unclear. While standard clinical MRI provides excellent delineation of the wrist’s complex arrangement of bones and soft tissues, it often fails to reveal any causative pathology. Among potential hypotheses for unexplained dorsal pain is that scaphoid restriction during extension overloads the periscaphoid ligament and articular cartilage1. However, such hypotheses remain difficult to directly test because clinical wrist MRI is performed in the neutral position due to lack of an appropriate mechanical device to guide motion and flexible receive coil to effectively capture signal in a range of positions. We endeavor to image the wrist in positions that better match the conditions during which pain is reported. To do so, we describe a prototype apparatus that allows extended and weight bearing MRI and report initial findings in volunteers.Methods
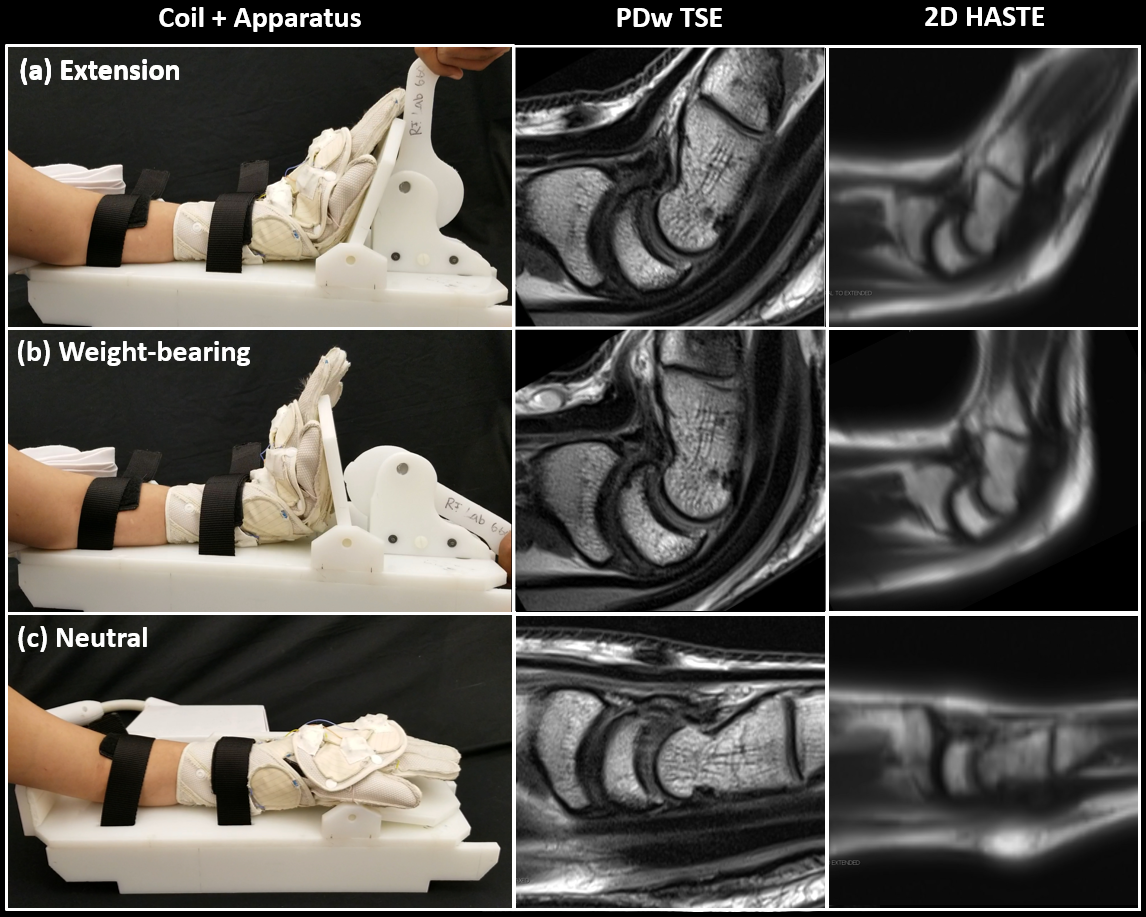
Two specialized, non-clinical devices are required to facilitate extended wrist MRI: a flexible receive coil and an apparatus to guide the desired motion. To address the former, we utilized a previously described “glove” coil that consists of twenty-four flexible six-cm high-impedance loops2 that are intended to alleviate signal-to-noise degradation arising from coil coupling3. The glove coil was designed to enable a variety of hand and wrist positions, including wrist extension. We additionally built an apparatus to guide wrist extension and loading (Figure 1). The apparatus includes a base that is locked to the MRI patient table, along with straps and an elbow stopper to immobilize the forearm. The palm rests on a hinged platform that shares an axis of rotation with the wrist. A lever enables a manually controlled load to be applied to the wrist via the platform. When the lever is fully engaged the platform is locked into the predetermined maximum weight-bearing position (Figure 2). This position is determined on a patient-specific basis prior to the scan by adjusting the distance between the wrist and hinged platform. Manual load application was preferred over remotely controlled techniques, such as pneumatic or electronic, to allow real-time patient control and ensure patient comfort.The left wrists of 9 asymptomatic volunteers (3 females, 6 males, age = 30 ± 13 years) were scanned using the glove coil and positioning apparatus on a 3T MRI system (Prisma, Siemens Healthcare, Erlangen, Germany). Static proton density weighted turbo spin echo (PDw TSE) images (TE/TR/ETL/TA=33ms/3500ms/9/3:05min, voxel size = 0.3x0.3x2mm) were acquired through the capital-lunate articulation with the wrist in the neutral, extended, and extended weight bearing positions. For the extended position, patients were instructed to voluntarily and maximally extend and hold for the duration of the scan. Similarly, the patient was instructed to push the apparatus lever to apply the maximum tolerable load during the weight bearing TSE acquisition.
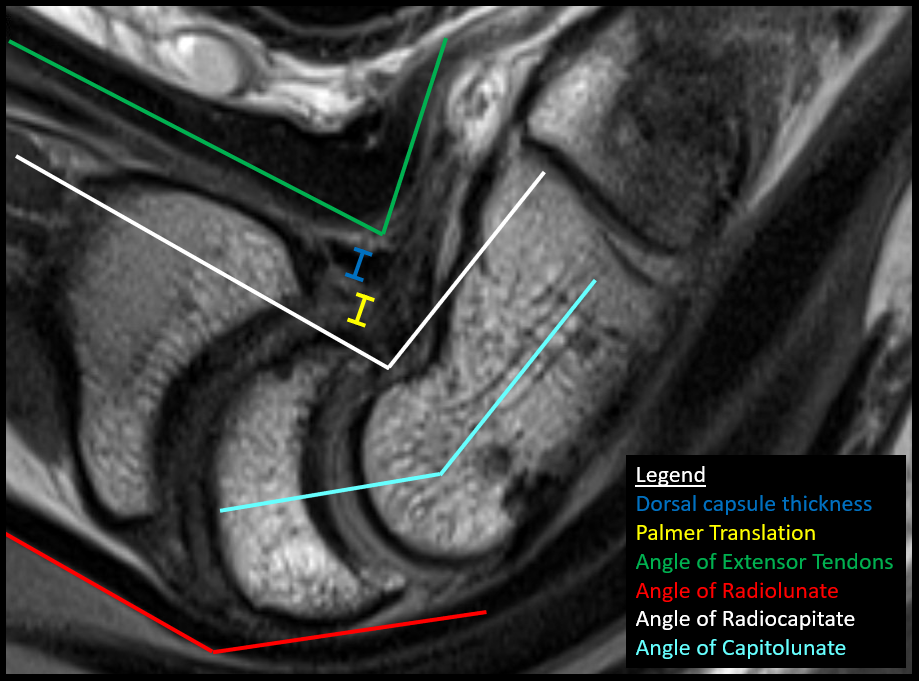
Two musculoskeletal radiologists independently evaluated the following anatomy and conditions (Figure 3) changes in dorsal capsule thickness 2) alterations in angulation of the radius, lunate, and capitate 3) translation of the lunate on the radius 4) changes in angulation of the extensor tendons. 5) evidence of lunate-capitate or dorsal capsule impingement. Dynamic motion was assessed on 2D HASTE images (TE/TR/ETL/TA=66ms/1180ms/112/30s, voxel size = 0.94x1.25x7mm) and maximum angulation of the radius and capitate was compared with static images.
The Pearson correlation was calculated to determine inter-reader agreement. The paired, two-tailed Student’s t-test was used to determine the statistical significance between measurements in the neutral and extended positions, and extended and weight-bearing positions. Statistical significance was set at p<0.05, and all tests are reported without multiple comparison correction and without regard to sex due to the exploratory nature of the study.
Results and Discussion
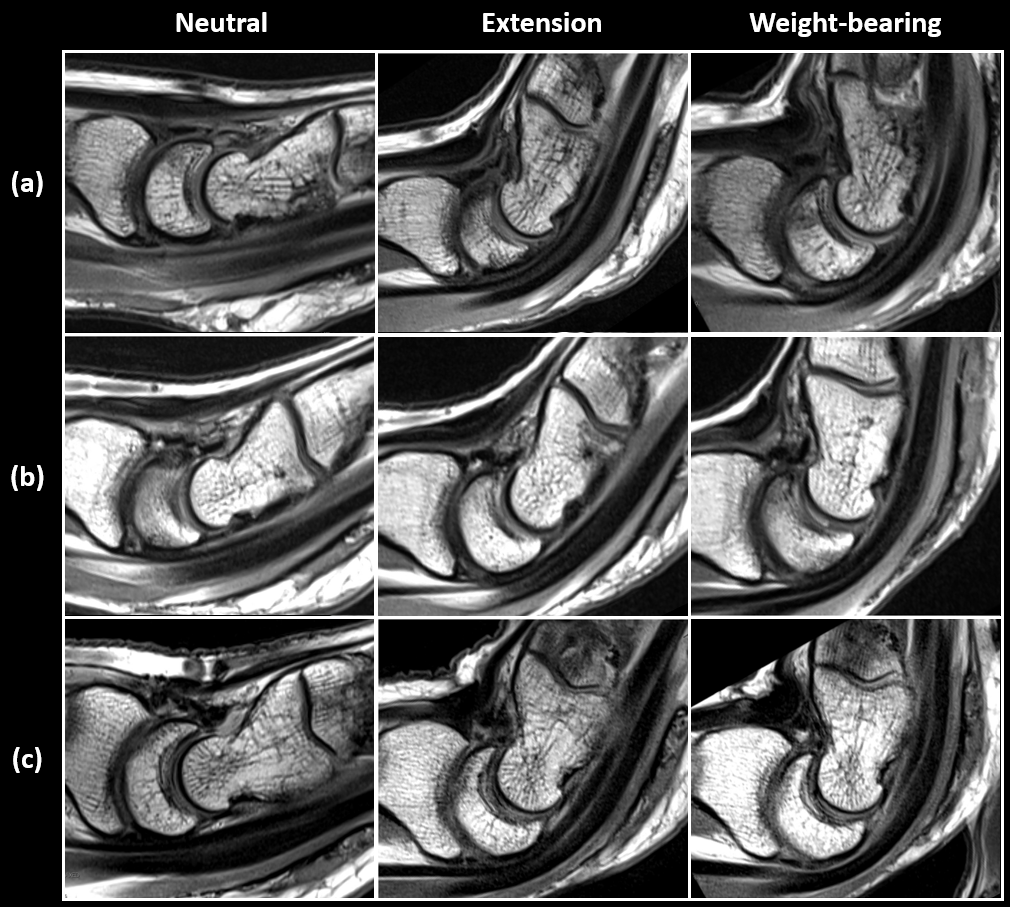
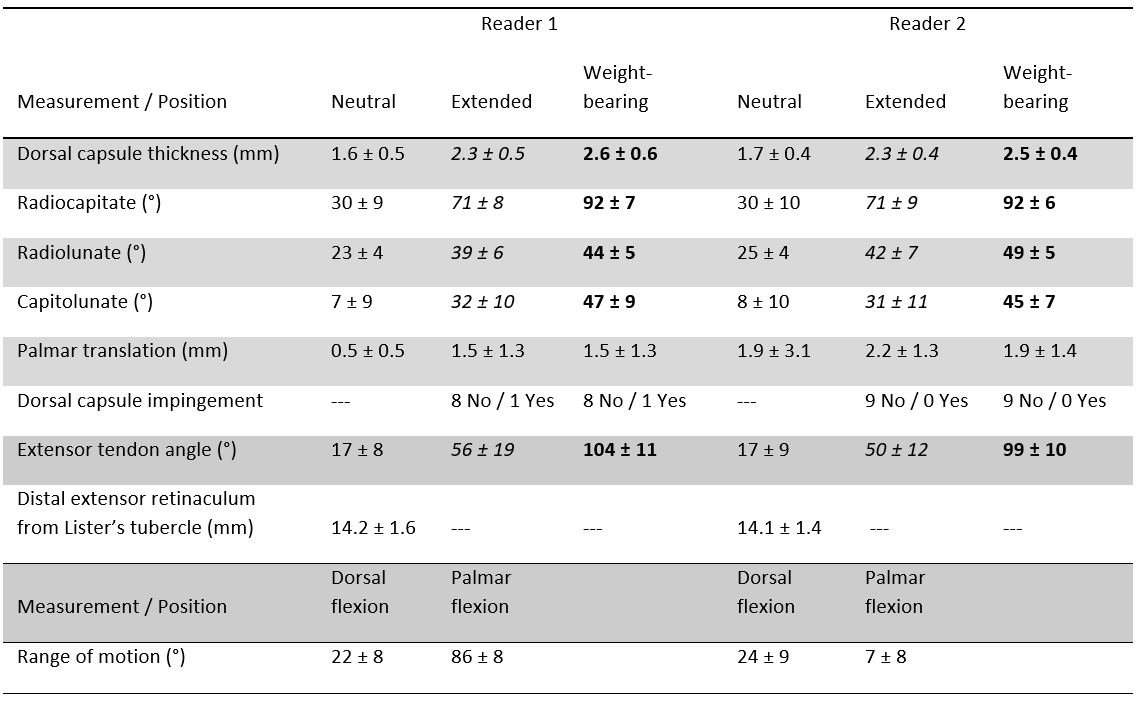
The static PDw TSE images allowed visualization of various anatomical structures relevant to dorsal wrist pain in neutral, extended, and weight-bearing positions (Figure 4). Table 1 summarizes the structural measurements in 9 asymptomatic volunteers. Excellent reader agreement was observed (r>0.57) for all measurements and positions except Palmar translation in the neutral position (r=0.22). The weight-bearing position resulted in significant increases in dorsal capsule thickness and radiocapitate, radiolunate, capitolunate and extensor tendon angulation. Evidence of dorsal capsule impingement was noted in 1 of 9 cases by Reader 1 and 0 of 9 by Reader 2.In conclusion, the wrist position apparatus and glove coil enable artifact-free imaging and evaluation of structural impingement and angulation throughout the motion range. This pilot study on asymptomatic volunteers sets the stage for comparative studies between symptomatic and asymptomatic patients.
Acknowledgements
This work was performed under the rubric of the Center for Advanced Imaging Innovation and Research (CAI2R, www.cai2r.net), a NIBIB Biomedical Technology Resource Center (NIH P41 EB017183).References
1. E.M. Nance, D.J. Byun, Y. Endo, S.W. Wolfe, S.K. Lee. Dorsal Wrist Pain in the Extended Wrist-Loading Position: An MRI Study. J Wrist Surg. 2017 Nov;6(4):276-279.
2. B. Zhang, J. Ho, S. Hodono, B. Wang, R. Brown, R. Lattanzi, M. Vester, R. Rehner, M. Cloos. A 22-channel high impedance glove array for dynamic hand and wrist imaging at 3T. Proceedings of the International Society for Magnetic Resonance in Medicine Annual Meeting and Exhibition, 2020, Paris, France.
3. B. Zhang, D.K. Sodickson, M.A. Cloos. A high-impedance detector-array glove for magnetic resonance imaging of the hand. Nat Biomed Eng 2, 570–577 (2018).
Figures