0091
High resolution motion compensated contrast-free free-breathing 3D CMRA at 7T using single transmit coil
Shubhajit Paul1, Raphael Tomi-Tricot1,2, Camila Munoz1, Karl Philipp Kunze1,2, Shaihan Malik1,3, Joseph V. Hajnal1,3, Philippa Bridgen1,3, Thomas Wilkinson1,3, Sharon Giles1,3, Radhouene Neji1,2, Reza Razavi1, Claudia Prieto1,4, and René Michael Botnar1,4
1School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom, 3The London Collaborative Ultra high field System (LoCUS), London, United Kingdom, 4Escuela de Ingeniería, Pontificia Universidad Católica de Chile, Santiago, Chile
1School of Biomedical Engineering and Imaging Sciences, King’s College London, London, United Kingdom, 2MR Research Collaborations, Siemens Healthcare Limited, Frimley, United Kingdom, 3The London Collaborative Ultra high field System (LoCUS), London, United Kingdom, 4Escuela de Ingeniería, Pontificia Universidad Católica de Chile, Santiago, Chile
Synopsis
3D cardiovascular MR imaging at ultra-high field (7T) is very challenging due to magnetic-field inhomogeneity (B0 and B1), SAR constraints and also the coil-depth issues of surface coils. To our best knowledge this is the first report demonstrating contrast-free ultra-high resolution (0.7mm3 isotropic) free-breathing 3D CMRA images with translational respiratory motion compensation. To avoid SAR constraints imposed by the use of T2-preparation pulses, high excitation flip-angles are exploited to obtain high contrast between the coronary arteries and myocardium. This technique may be adopted for clinical applications to produce high-resolution cardiac MR images at 7T scanners.
INTRODUCTION:
Cardiovascular MR imaging (CMRI) at ultra-high magnetic field (7 Tesla) has the potential to provide images with spatiotemporal resolution at mesoscopic level due to the improved signal-to-noise ratio (SNR). However, at 7T, the increased magnetic-filed inhomogeneity, SAR constraints and also the coil-depth1 issues for transmit and receive of surface array coils make cardiac imaging extremely challenging.2–6 The increased transmit field (B1+) heterogeneity in the body at 7T leads to an inhomogeneous flip angle (FA) distribution.6,7 Different parallel transmission techniques (pTx)3,5,7–9 have been used to address this problem and improve cardiac imaging. So far at 7T only a few 3D CMRI9 studies with pTx and Coronary Magnetic Resonance Angiography (CMRA) studies employing thin slabs using two channel quadrature surface coils have been reported2,4. Because of the SAR constraints, it is also not straightforward to use T2-preparation pulses10 at 7T with standard adiabatic pulses. Therefore, an acquisition technique with low SAR preparation pulses or without the need of any preparation pulse is highly desired.Here we present for the first time ultra-high resolution (0.7mm3 isotropic) free-breathing translational motion compensated 3D CMRA images obtained without any preparation pulses (e.g. T2-prep) with Trueform B1-shim mode at 7T without using any contrast agent. We further have investigated the effect of magnetization transfer (MT) on the contrast behavior between blood and myocardium by employing FA variation.
METHODS:
A free‐breathing 3D CMRA gradient-echo sequence with variable density Cartesian spiral-like trajectory11, image navigator (iNAV)12 and chemical-shift selective fat-suppression (fatsat) was implemented on a MAGNETOM Terra 7T MRI scanner (Siemens Healthcare, Erlangen, Germany) (Figure 1). All the acquisitions were carried out with a body 8Tx/16Rx surface coil (Rapid Biomedical GmbH, Rimpar, Germany) in single transmit (1Tx) mode (Trueform). To circumvent the highly prominent magnetohydrodynamic effect at 7T, which disturbs the ECG typically used for cardiac synchronization, we employed a pulse oximeter (Siemens, Erlangen, Germany) instead. The motion-corrected image reconstruction framework used in this work has been described earlier.10–13 Foot-head (FH) and right-left (RL) translational respiratory motion is estimated from the iNAVs acquired at each heartbeat before the 3D CMRA readout and used to correct the acquired k-space data.To avoid SAR constraints imposed by the use of T2-preparation pulses and to address transmit field (B1+) heterogeneity across the thorax, the effect of high excitation flip-angles (FA) on contrast between the coronary arteries and myocardium was investigated employing free-breathing 3D CMRA for flip angles of 6°, 10°, 20°, 30° and 40°.
A healthy volunteer (male, 25 years old) was scanned in three different sessions to observe the reproducibility of the proposed approach. Acquisitions were performed in-vivo with 0.7mm3 (TR/TE = 4.8/2.17) and 0.9 mm3 (TR/TE = 4.6/2.1) isotropic resolution and 3-fold undersampling with FOV=320mm.
RESULTS:
A comparison between the CMRA images obtained with different excitation FAs (6°- 40°) is presented in Figure 2 for two different slice positions. For low flip-angles (6° and 10°), contrast between blood and myocardium is almost absent. The best contrast was obtained for a FA of 40°. A gradual increase in contrast and signal intensity from low towards high FA is apparent.CMRA images with the proposed approach and ultra-high resolution (0.7mm3 isotropic) are shown in Figure 3. Reformatted CMRI views are shown in Figure 3c-e. Figure 3f presents a tracked right coronary artery (RCA) and three cross-sectional images of the RCA.
CONCLUSION:
We demonstrated a new technique to obtain contrast-free ultra-high-resolution free-breathing 3D CMRA images at 7T with high contrast between the coronary arteries and myocardium. The dependency of magnetization transfer (MT) on FA and repetition time (TR) was reported earlier in human brain studies.14 The observed contrast could be due to MT and/or inflow at high FA and low TR. This method may be useful for 7T clinical applications for high resolution cardiac imaging and further evaluation in healthy subjects and patients is warranted.Acknowledgements
This work was supported by EPSRC (EP/L015226/1, EP/P032311/1, EP/P007619/1 and EP/P001009/1), the Wellcome/EPSRC Centre for Medical Engineering (NS/A000049/1) and 7T grant (Wellcome Trust Collaboration in Science grant [WT201526/Z/16/Z]).References
1. Terekhov, M. et al. New commercial 8Tx / 16RX array for Clinical 7T Cardiac MRI : initial experience. Proc. Intl. Soc. Mag. Reson. Med. 29 (2021), 2–4.2. Van Elderen, S. G. C. et al. Initial results on in vivo human coronary MR angiography at 7 T. Magn. Reson. Med. 62, 1379–1384 (2009).
3. Snyder, C. J. et al. Initial results of cardiac imaging at 7 Tesla. Magn. Reson. Med. 61, 517–524 (2009).
4. Van Elderen, S. G. C. et al. Right coronary MR angiography at 7 T: A direct quantitative and qualitative comparison with 3 T in young healthy volunteers. Radiology 257, 254–259 (2010).
5. Schmitter, S. et al. Cardiac imaging at 7 tesla: Single- and two-spoke radiofrequency pulse design with 16-channel parallel excitation. Magn. Reson. Med. 70, 1210–1219 (2013).
6. Aigner, C. S., Dietrich, S. & Schmitter, S. Three-dimensional static and dynamic parallel transmission of the human heart at 7 T. NMR Biomed. 34, 1–15 (2021).
7. Schmitter, S., Schnell, S., Uğurbil, K., Markl, M. & Van de Moortele, P. F. Towards high-resolution 4D flow MRI in the human aorta using kt-GRAPPA and B1+ shimming at 7T. J. Magn. Reson. Imaging 44, 486–499 (2016).
8. Hess, A. T. et al. Aortic 4D flow: Quantification of signal-to-noise ratio as a function of field strength and contrast enhancement for 1.5T, 3T, and 7T. Magn. Reson. Med. 73, 1864–1871 (2015).
9. Aigner, C. S., Dietrich, S., Schaeffter, T. & Schmitter, S. Calibration-free pTx of the human heart at 7T via 3D universal pulses. Magn. Reson. Med. 1–15 (2021) doi:10.1002/mrm.28952.
10. Cruz, G., Atkinson, D., Henningsson, M., Botnar, R. M. & Prieto, C. Highly efficient nonrigid motion-corrected 3D whole-heart coronary vessel wall imaging. Magn. Reson. Med. 77, 1894–1908 (2017).
11. Prieto, C. et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. J. Magn. Reson. Imaging 41, 738–746 (2015).
12. Henningsson, M., Smink, J., Razavi, R. & Botnar, R. M. Prospective respiratory motion correction for coronary MR angiography using a 2D image navigator. Magn. Reson. Med. 69, 486–494 (2013).
13. Bustin, A. et al. 3D whole-heart isotropic sub-millimeter resolution coronary magnetic resonance angiography with non-rigid motion-compensated PROST. J. Cardiovasc. Magn. Reson. 22, 1–16 (2020).
14. Helms, G., Dathe, H. & Dechent, P. Modeling the influence of TR and excitation flip angle on the Magnetization Transfer Ratio (MTR) in human brain Obtained from 3D spoiled gradient echo MRI. Magn. Reson. Med. 64, 177–185 (2010).
Figures
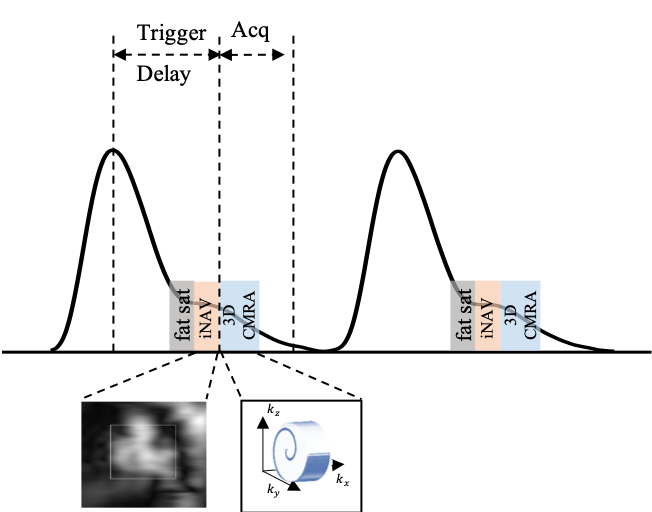
Figure 1: Schematic representation of translational motion corrected free-breathing 3D CMRA sequence with an accelerated 3D variable density spiral-like Cartesian trajectory with golden angle between spiral-like interleaves (VD-CASPR), preceded by low‐resolution coronal 2D image navigators (iNAVs) and fat-suppression (fatsat). iNAVs are used to estimate and correct for the beat-to-beat 2D translational respiratory-induced motion of the heart. The CMRA pulse sequence is shown with respect to the pulse oximeter signal.
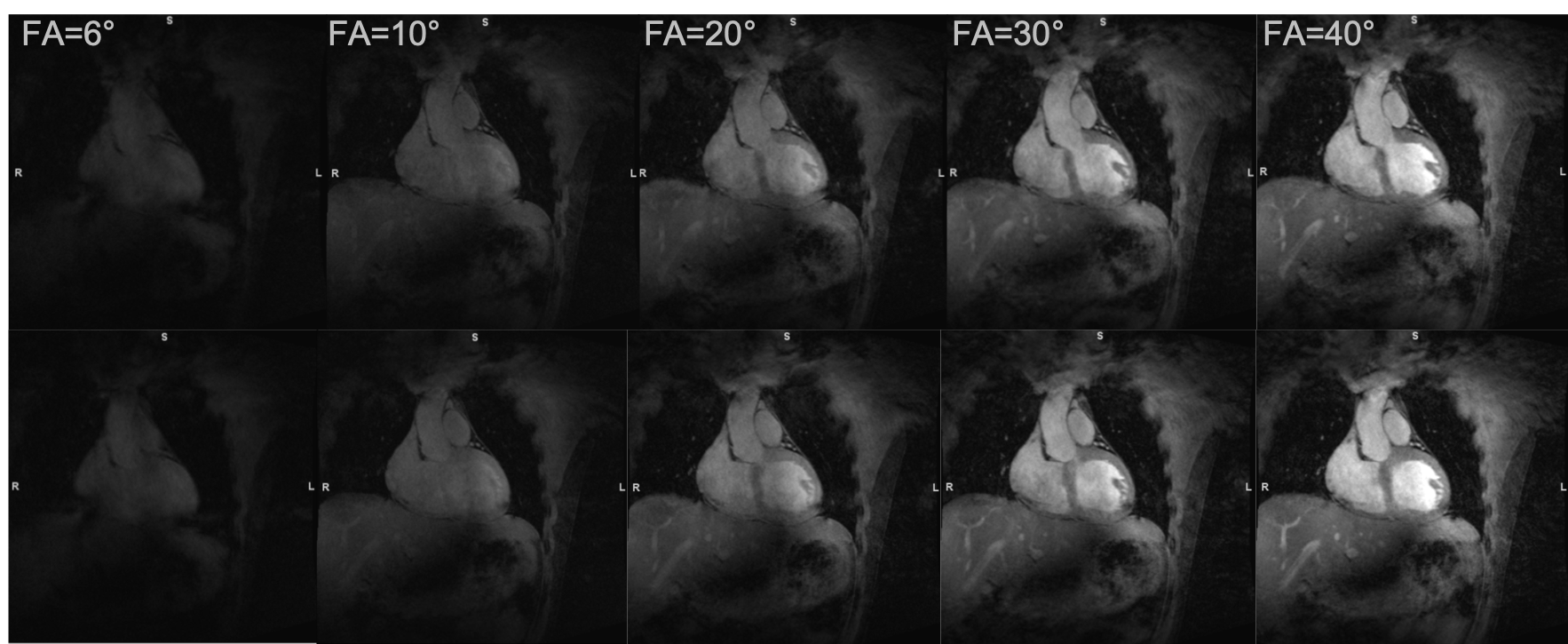
Figure 2: Excitation flip-angle (FA) dependence of magnetization transfer induced contrast between the coronary arteries and myocardium obtained with the proposed free-breathing 3D CMRA sequence. Images obtained with excitation FAs of 6°, 10°, 20°, 30° and 40°, with 40° providing the best contrast and highest signal-to-noise-ratio. Top and bottom rows are two different slice positions. All images are equally windowed. Acquisition parameters: 0.9 mm3 isotropic resolution, TR/TE=4.6/2.1 ms, acceleration factor=3, bandwidth=406 Hz/px.
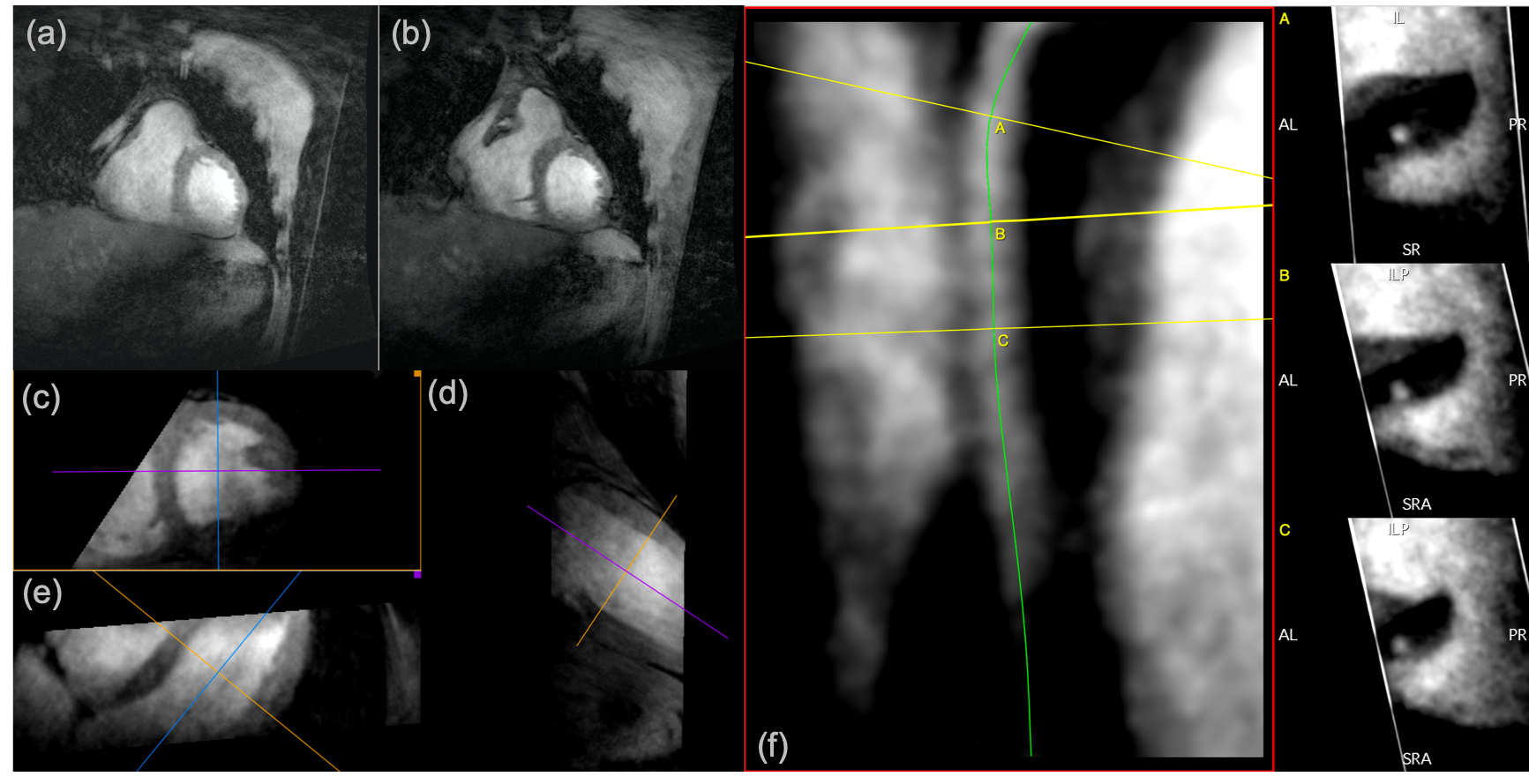
Figure 3: Proposed ultra-high resolution free-breathing 3D CMRA images (coronal view) for two different slice positions obtained at 7T (a, b). (c-e): Reformatted views of the 3D CMRA dataset. (f): Tracked right coronary artery (RCA) with cross-sectional views reconstructed in the mid-RCA. Acquisition parameters: 0.7 mm3 isotropic resolution, TR/TE=4.8/2.17 ms, acceleration factor=3, FA=40°, bandwidth=399 Hz/px.
DOI: https://doi.org/10.58530/2022/0091