0040
Predicting pathological status of prostate cancer patients – Examining the value and leading features in MRI Radiomics1Division of Radiation Oncology, IEO, European Institute of Oncology IRCCS, Milano, Italy, 2Division of Radiology, IEO, European Institute of Oncology IRCCS, Milano, Italy, 3Department of Oncology and Hemato-oncology, University of Milan, Milano, Italy, 4Department of Experimental Oncology, IEO, European Institute of Oncology IRCCS, Milano, Italy, 5Radiology Department, National Cancer Institute, Putrajaya, Malaysia, 6Division of Urology, IEO, European Institute of Oncology IRCCS, Milano, Italy, 7Unit of Medical Physics, IEO, European Institute of Oncology IRCCS, Milano, Italy, 8Radiation Research Unit, IEO, European Institute of Oncology IRCCS, Milano, Italy, 9Scientific Directorate, IEO, European Institute of Oncology IRCCS, Milano, Italy, 10Precision Imaging and Research Unit, IEO, European Institute of Oncology IRCCS, Milano, Italy
Synopsis
The risk of patients being under- or overtreated during radiotherapy depends heavily on the pre-treatment assessment. Prediction models for surgical margin status, pathological lymph nodes, pathological tumor stage and ISUP grade group were formed using clinical and radiological features alone and together with whole-prostate radiomic features in 100 patients who proceeded to prostatectomy after multiparametric-MRI. The addition of radiomics features significantly improved AUC for the prediction models. The leading radiomic features differed between the different models.
Introduction
The risk of patients being under- or over-treated during radiotherapy depends heavily on the pre-treatment assessment and in the case of prostate cancer, increasingly on MRI examination. The combination of radiomics and clinical features for the prediction of pathological features of prostate cancer may improve decision-making and personalization of treatment.1 The purpose of this study was to evaluate the ability of radiomic features to improve the accuracy of non-invasive prediction of pathological features of prostate cancer with prostatectomy as confirmation. We further compared the contributions of leading radiomics features in the prediction models.Methods
A representative subset of 100 patients from a cohort of roughly 1500 who have undergone prostate MRI and prostatectomy in our institution since 2015 was selected by balancing the clinical characteristics of the patients. The prostate of each patient was segmented from T2-weighted MR images by an expert radiologist, and after normalization and bias correction were used in the extraction of 1810 radiomic features (pyradiomics 3.0.1, AIM Harvard).2 The set of clinical (age, iPSA, cT, biopsy total Gleason score, preoperative ISUP grade group, and risk class), radiological (prostate volume, prostate imaging reporting & data system (PI-RADS) category, and extra-prostatic extent (EPE) score) and radiomic features was reduced to 50 features using a hierarchical clustering procedure based on absolute rank correlation. Gradient-boosted decision tree models were separately trained using clinical and radiological features alone and in combination with the radiomics features to predict surgical marginal status (R0 vs R1), the presence of pathological lymph nodes (pN0 vs pN1), pathological tumor stage (pT2 vs pT3), and pathological ISUP grade group (≤3 vs ≥4) and validated with 32-times repeated 5-fold cross validation. The models were evaluated and compared in terms of their AUC values. We also obtained estimates of the mean feature importance based on mean prediction value change calculated over validation folds.Results
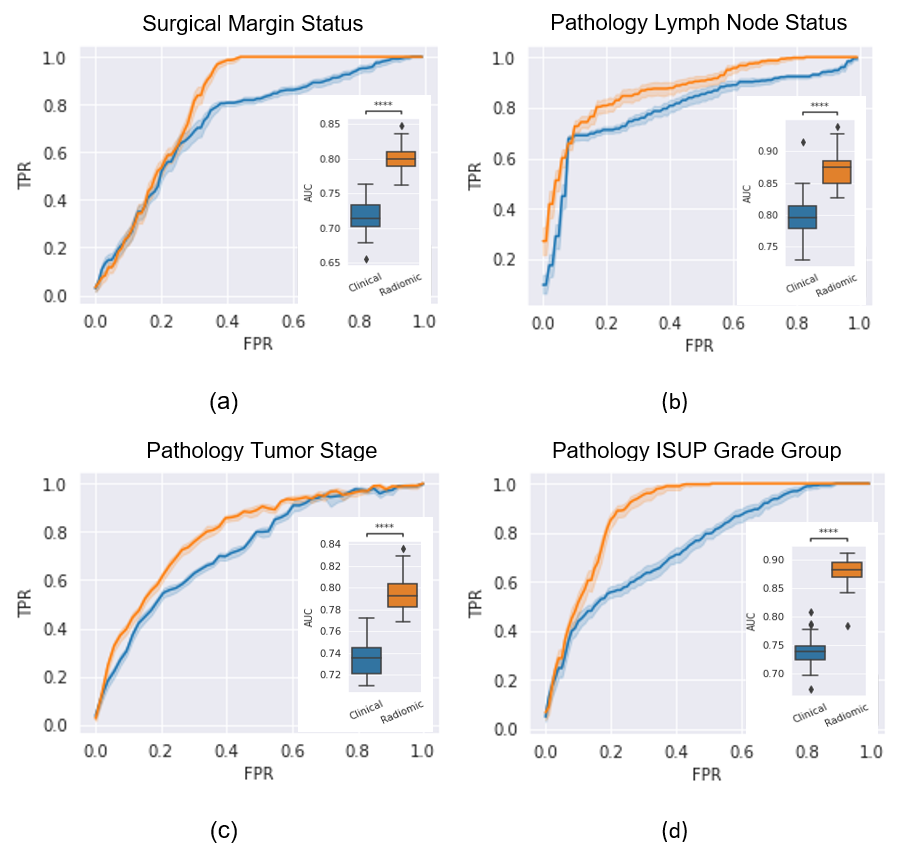
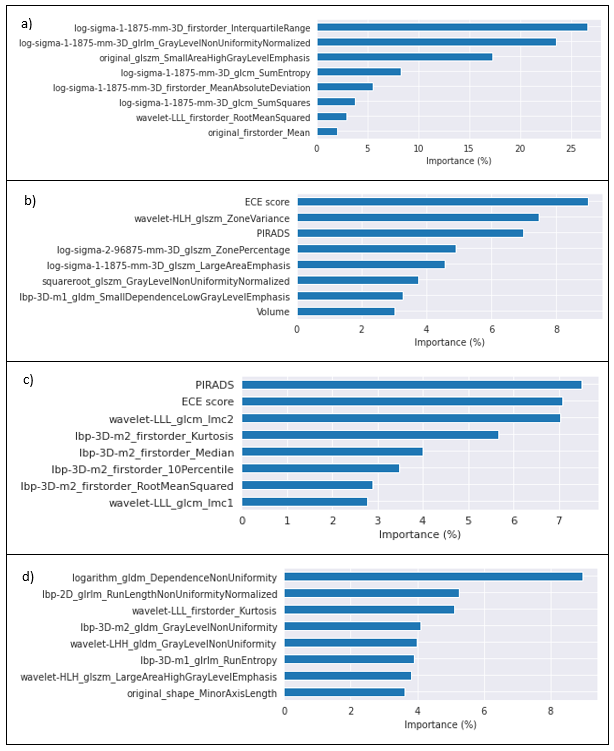
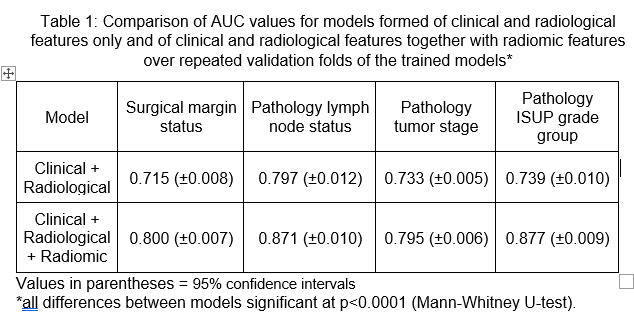
The validation AUC values (±95% CI) of the different models were 0.800 (±0.007) for surgical marginal status, 0.871 (±0.010) for pathological lympho-nodes, 0.795 (±0.006) for pathological tumor stage, and 0.877 (±0.009) for ISUP grade group (see Figure 1). The addition of radiomics features led to increases of AUC ranging between 0.061 (pT) and 0.139 (ISUP grade group) as illustrated in Figure 1 and summarized in Table 1. All AUC gains were statistically significant at a level of at least 0.0001 (Mann-Whitney U-test). The contributions of the top eight radiomic features in each model are displayed in Figure 2. In the models for pathological lymph nodes and tumor stage, both EPE score and PI-RADS category had a large impact on the predictions, while none of the clinical or radiological variables appeared in the top eight for surgical marginal status and pathological ISUP grade group prediction. The leading eight radiomic features were largely distinct between the models for the four variables examined, in general involving Laplacian of Gaussian (“log”) features for surgical marginal status, local binary pattern (“lbp”) features for pathological tumor stage, and wavelet features for pathological ISUP grade group.Discussion
We found the inclusion of whole-prostate radiomics to improve prediction of all four pathological features of prostate cancer examined, with AUC values in the 0.80-0.88 range. The potential of a radiomic + clinical feature model to better predict pathological features of prostate cancer, and in particular extra-prostatic extension and pelvic lymph node involvement, is of considerable interest for guiding the clinical decision-making process and can provide valuable information for personalizing therapy. These preliminary, but promising, results will be validated in the larger cohort of 1500 patients. The leading radiomics features in each model were largely distinct, and tended to involve clusters within radiomic feature families, suggesting that distinct aspects of prostate appearance are contributing to the different models. This small study reinforces our prior results for the ability of whole-prostate radiomics features to contribute to the prediction of clinically relevant endpoints. Nonetheless, considering the small size of our cohort, the possibility of overfitting is a concern.Conclusion
Our results illustrate that incorporation of radiomics features, even at the whole-prostate level, can have a significant impact on the prediction of prostate cancer features, and that radiomic features and clinical parameters often complement each other. Different types of radiomic features can be important in different contexts and should not be judged on an absolute utility scale.Acknowledgements
No acknowledgement found.References
1. Gugliandolo SG, Pepa M, Isaksson LJ, et al. MRI-based radiomics signature for localized prostate cancer: a new clinical tool for cancer aggressiveness prediction? Sub-study of prospective phase II trial on ultra-hypofractionated radiotherapy (AIRC IG-13218). Eur Radiol. 2020 Aug 27.
2. Isaksson LJ, Raimondi S, Botta F, et al. Effects of MRI image normalization techniques in prostate cancer radiomics. Phys Med. 2020;71:7-13.
Figures