0037
Differentiation between benign liver lesions, primary malignant and secondary malignant tumors using APT and IVIM imaging1Department of Radiology, the First Affiliated Hospital of Dalian Medical University, Dalian, China, 2Philips Healthcare, Beijing, China
Synopsis
This study aims to assess the efficacy of amide proton transfer-weighted (APTw) combined with intravoxel incoherent motion (IVIM) imaging in differentiation benign liver lesions, primary malignant and secondary malignant tumors. Results showed that a high diagnostic efficacy could be achieved through the combination use of the APT value and IVIM parameters.
Introduction
Contrary to benign lesions, the malignant liver lesions including primary and secondary liver cancer are usually associated with poor prognosis. The treatment plan for benign or different malignant liver tumors can also be significantly different. However, it is still challenging for conventional MR imaging to differentiate among these different kinds of lesions. Amide proton transfer weighted (APTw) imaging is a kind of chemical exchange saturation transfer (CEST) imaging technology [1-2] that enables indirect detection of the distribution of proteins and peptides in tissues. The feasibility of APTw imaging for liver had been previously validated in animal studies [3]. The intravoxel incoherent motion (IVIM) imaging can simultaneously obtained the quantitative blood micro-perfusion and water diffusion information for liver tumors. The purpose of this study was to investigate the clinical value of APTw and IVIM in differentiation of benign liver lesions, primary malignant and secondary malignant tumors.Materials and Methods
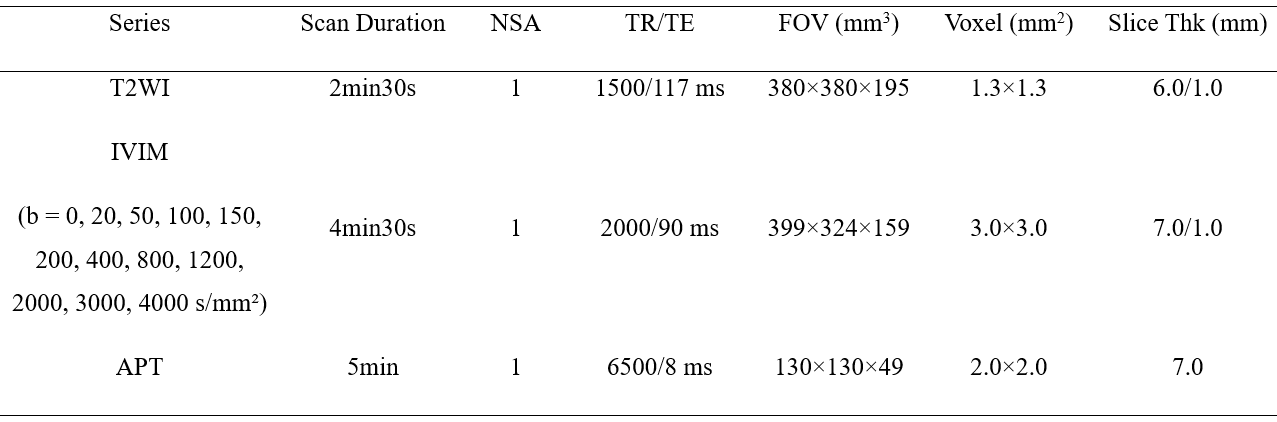
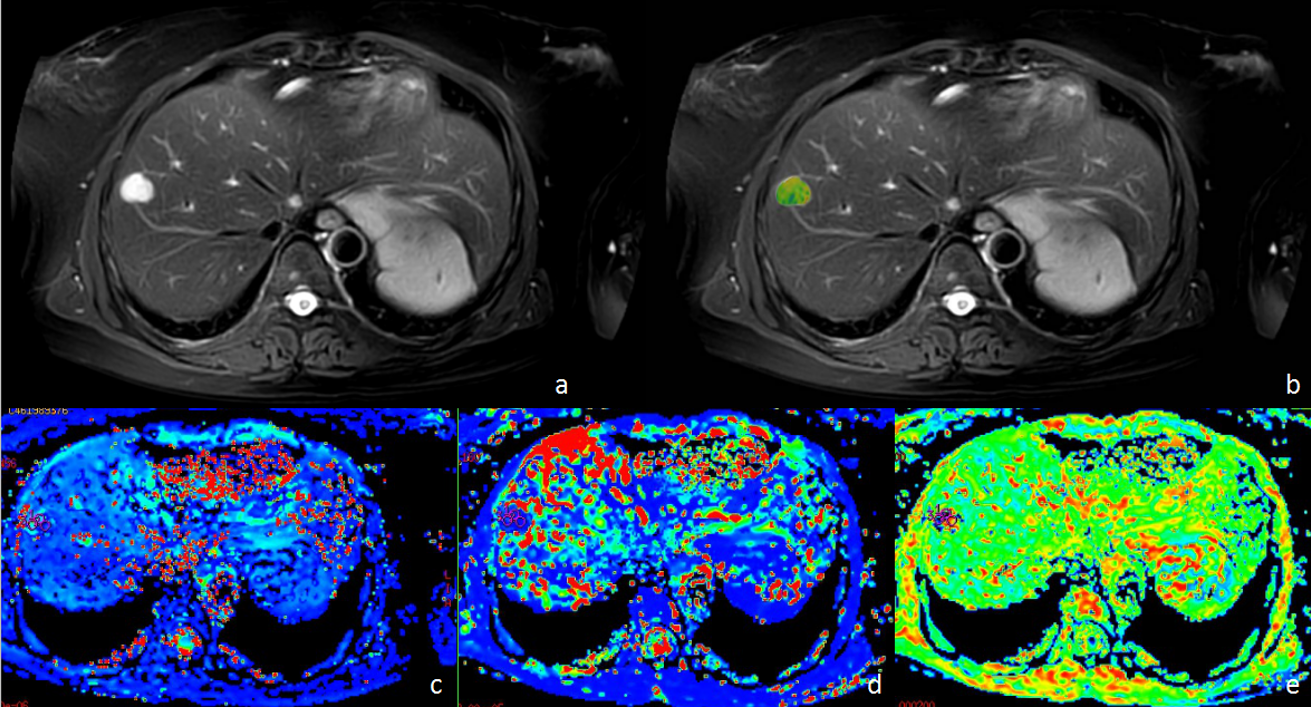
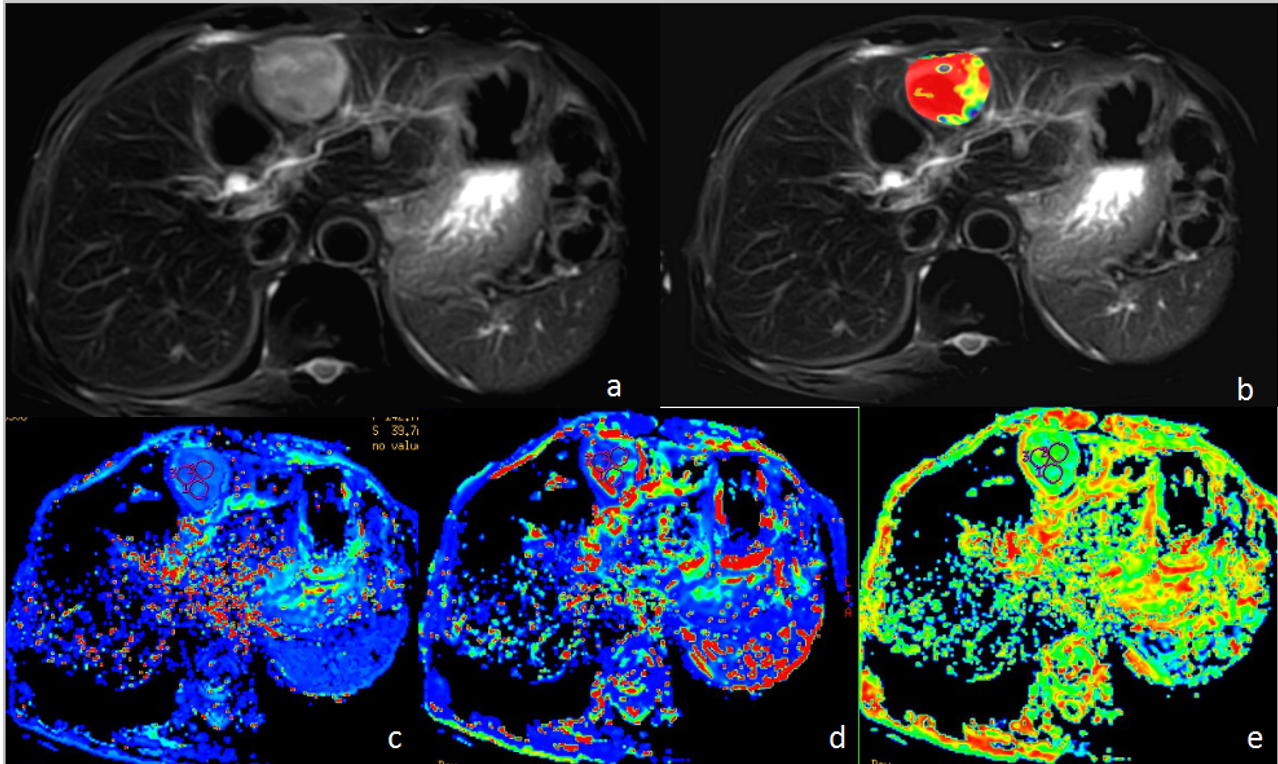
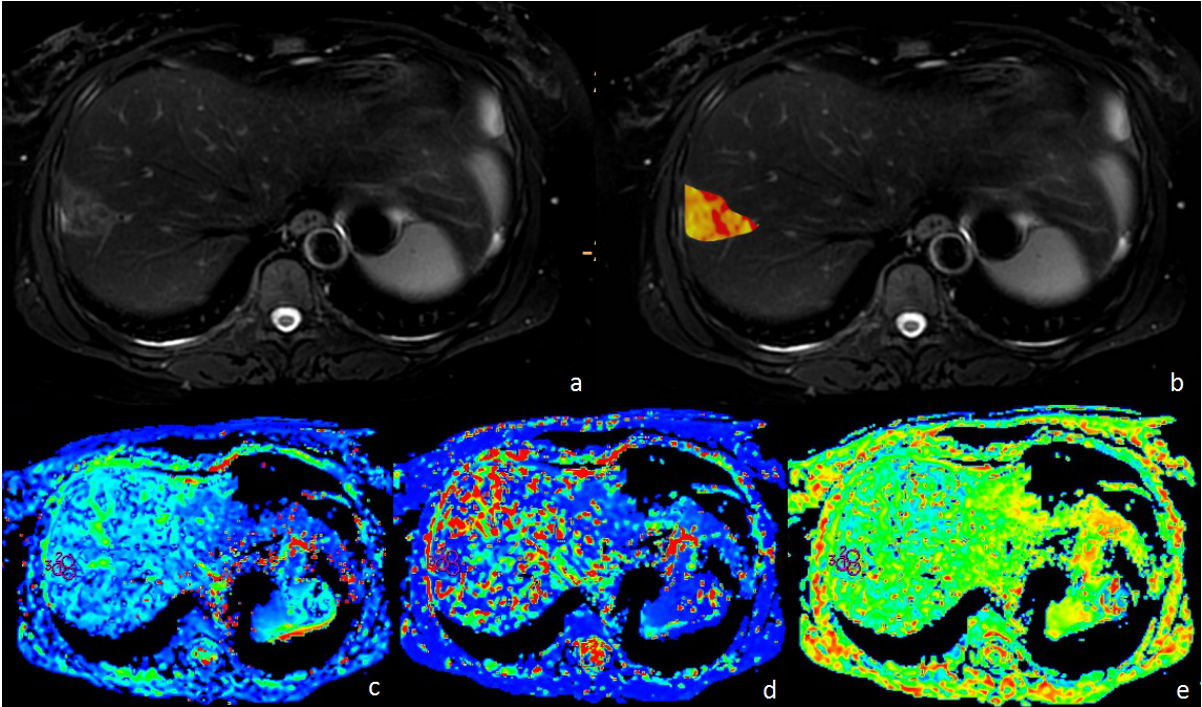
This study has been approved by the local IRB. 81 patients with 85 focal liver lesions in our hospital were retrospectively analyzed. 22 cases of benign lesions (11male, mean age, 56 years; range, 31–77 years), 40 patients with primary liver cancer (32male, mean age, 62 years; range, 31–81 years; 31 HCC and 9 ICC) and 19 patients with 23 secondary liver cancer (11 male, , mean age, 62 years; range, 34–89 years). All patients performed MR examinations on a 3.0 T MR scanner (Ingenia CX, Philips Healthcare, Best, the Netherlands). The MR protocol includes ATPw, IVIM and T2 weighted (T2WI) imaging sequences and detailed scan parameters is shown in Table 1. The APTw images were reconstructed on the MR console immediately after the data acquisition and then transferred to the workstation (Intellispace Portal; v. 10; Philips Healthcare) for quantitative measurements. Referring to the anatomical location of lesion obtained on T2WI, three circle regions of interest (ROI), area of 100-200 mm2, were manually placed on the parenchyma of the tumor on APTw images and IVIM parameter images, respectively (Figure1-3). The raw data of IVIM were uploaded to the GE AW 4.6 workstation, and maps of the IVIM parameters were calculated with the Functool software. The mean values of APTw and IVIM parameters from the three ROIs were calculated and used for further analysis. Use Kruskal-Wallis test to compare whether there are statistical differences in APT values and IVIM parameters in benign liver lesions (group 1), primary malignant tumors (group 2) and secondary malignant tumors (group 3) with the SPSS 22.0 software (IBM, U.S.A). ROC curves were used to analyze the efficiency of the APT and IVIM parameters, as well as their combination, for differential diagnosis between three groups. Logistic regression was used to calculate the value of APT combined with IVIM parameters. P < 0.05 was considered to be statistically significant.Result
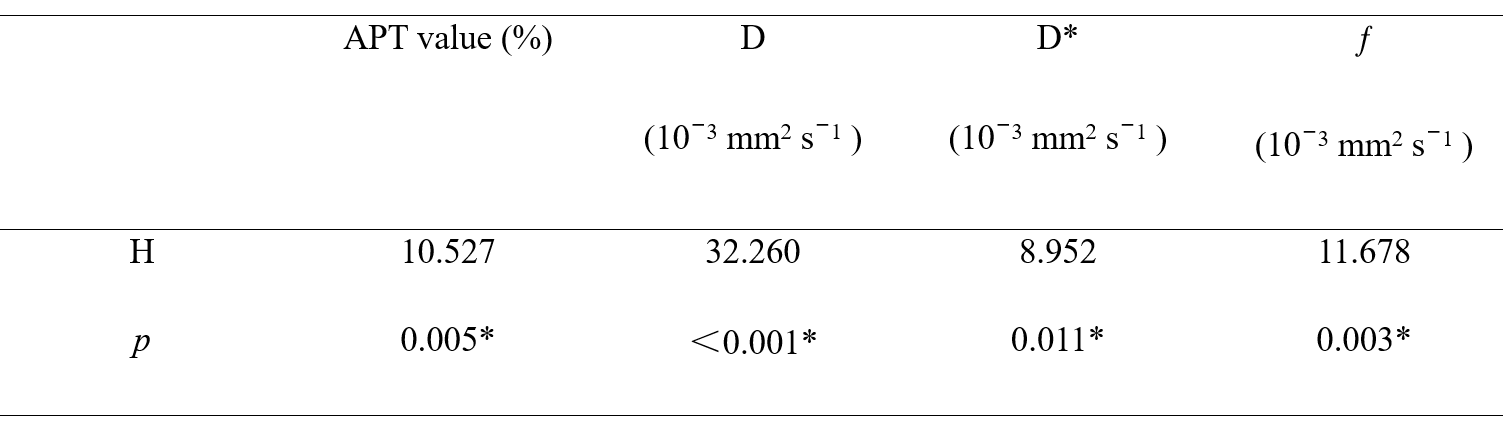
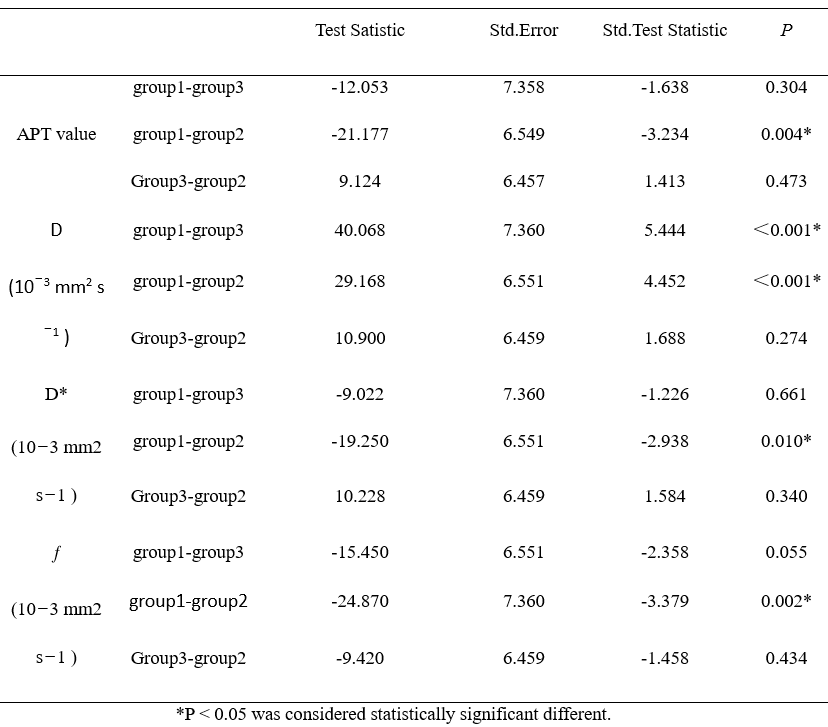
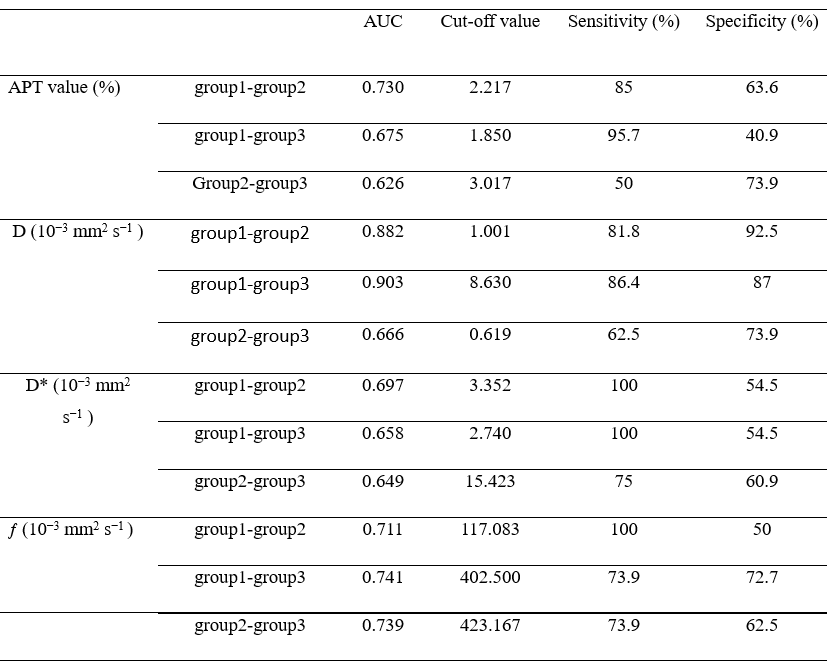
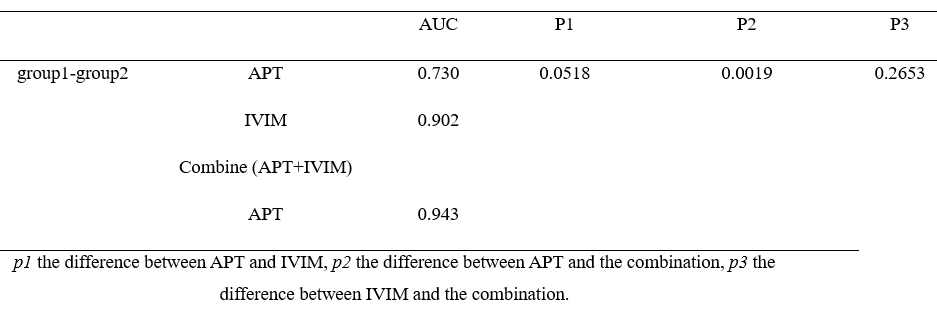
As shown in table 2 and 3, there is a difference in APT value, D, D*, f between group 1 and group 2, and D between group 1 and group 3. There is no statistical difference between other groups. As shown in table 4, the highest AUC is the D value to discriminate group 1 and group 3. The combinational use of APTw and IVIM imaging showed significantly improved differential diagnosis efficacy between benign and primary malignant tumor(Table 5).Discussion and Conclusion
APT can detect the level of polypeptide and free protein in organism. Intravoxel incoherent motion (IVIM) DWI distinguishes the diffusion of water molecules in biological tissues from microcirculatory perfusion. There are many reports on the diagnosis of neoplastic lesions of the liver by IVIM-DWI [4]. Further studies will be conducted to explorer the relationship between APT and IVIM.In this study, we had preliminarily confirmed the clinical value of APTw and IVIM parameter (fraction of fast ADC Mono and fraction of fast ADC Bi) in the differential diagnosis of primary and secondary liver cancer. With APT value combined with IVIM parameters, the AUC was improved to 0.943. The combined detection of the two methods can significantly improve the detection sensitivity and detection accuracy to some extent.
Acknowledgements
NoReferences
[1] Ferrucci JT. Liver tumor imaging: current concepts. Keio J Med. 1991 Dec;40(4):194-205.
[2]Choi SH. Can Amide Proton Transfer MRI Distinguish Benign and Malignant Head and Neck Tumors? Radiology. 2018 Sep;288(3):791-792.
[3]Chen SZ, Yuan J, Deng M, Wei J, Zhou J, Wáng YX. Chemical exchange saturation transfer (CEST) MR technique for in-vivo liver imaging at 3.0 tesla. Eur Radiol. 2016 Jun;26(6):1792-800.
[4] Ai Z, Han Q, Huang Z, Wu J, Xiang Z. The value of multiparametric histogram features based on intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) for the differential diagnosis of liver lesions. Ann Transl Med. 2020;8(18):1128.
Figures