0010
Sex-Differences in Intracranial Plaque Burden in Hypertensive Patients with Acute Ischemic Stroke: A Vessel Wall MR Imaging Study
Jae W. Song1, Jiayu Xiao2, Steven Y Cen2, Xiao Liu3, Fang Wu4, Konrad Schlick5, Qi Yang3, Shlee S Song5, and Zhaoyang Fan2
1University of Pennsylvania, Philadelphia, PA, United States, 2University of Southern California, Los Angeles, CA, United States, 3Chaoyang Hospital, Beijing, China, 4Xuanwu Hospital, Beijing, China, 5Cedars-Sinai Medical Center, Los Angeles, CA, United States
1University of Pennsylvania, Philadelphia, PA, United States, 2University of Southern California, Los Angeles, CA, United States, 3Chaoyang Hospital, Beijing, China, 4Xuanwu Hospital, Beijing, China, 5Cedars-Sinai Medical Center, Los Angeles, CA, United States
Synopsis
Hypertension is associated with intracranial atherosclerosis (ICAS) and is a leading cause of acute ischemic stroke (AIS). Given sex-differences in the severity of hypertension, we hypothesized sex-differences in ICAS burden among hypertensive patients with AIS. Results show males have significantly higher adjusted total plaque burdens than females. Subgroup analyses show treated hypertensive males with AIS have higher total proximal and bifurcation plaques than treated females. Untreated hypertensive females have significantly higher total proximal and bifurcation plaques compared to untreated males. The results suggest attention to differential hypertension management by sex may be warranted to reduce ICAS burden and AIS risk.
Introduction
Studies report sex-differences in the severity of hypertension1, which is a strong risk factor for intracranial atherosclerosis (ICAS) and a leading cause of acute ischemic stroke (AIS).2 Based on a higher incidence of hypertension in males compared to females of the same age, we hypothesized a higher total ICAS burden among hypertensive males with AIS compared to hypertensive females.Methods
Patients with a preexisting diagnosis of hypertension, diagnosed with an AIS secondary to ICAS and who underwent an intracranial vessel wall MRI (VWI) within 8 weeks of symptom onset were retrospectively identified. Patients underwent VWI on a 3.0-Tesla scanner (MAGNETOM Prisma, Verio, Skyra, Siemens, Erlangen, Germany) using a 64-channel head-neck coil (Prisma), 32 channel head coil (Verio), or 20-channel head-neck coil (Skyra). VWI was performed using a cerebrospinal fluid-suppressed whole-brain 3D variable-flip-angle turbo spin-echo sequence. Imaging parameters were: repetition time, 900ms; echo time, 15 ms; voxel size, isotropic 0.53 or 0.55 mm; field of view, 170x170 mm2 or 170x210 mm2, number of slices, 224 or 240; scan time approximately 8 minutes. Demographic data, cardiovascular risk factors, and medication history were recorded. Three blood pressure (BP) measurements on the first 3 days of admission were recorded and averaged. Patients with a pre-admission history of hypertension and taking anti-hypertensive medication were defined as treated hypertensive patients. A neuroradiologist with 5 years of experience interpreting VWI blinded to clinical history measured plaque on VWI. Proximal and distal plaques were defined as involving the A1/M1/P1 or A2/M2-M3/P2 segments of the anterior/middle/posterior cerebral arteries, respectively. Bifurcation plaques were identified at the junction between vessel segments. Total plaque burden was the sum of proximal and distal plaques. Culprit plaque was identified by wall thickening/enhancement in the most stenotic lumen supplying the ischemic territory. Negative binomial model was used to assess the association between plaque-count and sex, as well as the interaction between sex and treatment. Covariates were selected by LASSO procedure. SAS 9.4 was used for data analysis.Results
Sixty-one subjects (male, N=42) with a diagnosis of hypertension and AIS due to ICAS were included. There were no significant sex-differences in demographic or cardiovascular risk factors except for smoking history (p=0.002). The adjusted total plaque count for males was 1.58 (95% CI 1.18-2.11, p<0.01) times has high as females. The adjusted proximal plaque count for males was 1.41 (95% CI 1.04-1.93) times has high as females; the adjusted distal plaque count for males was also higher than females (1.51, 95% CI 0.89-2.57, p=0.12) although this did not reach statistical significance (Figure 1). We also tested for a sex-effect among hypertensive patients on an anti-hypertensive medication. Among treated hypertensive patients, the adjusted total proximal and bifurcation plaque counts were 1.46 (95% CI 1.01-2.13) and 1.50 (95% CI 0.91-2.49) times as high in males than females, respectively. By contrast, among untreated hypertensive patients, the adjusted total proximal and bifurcation plaque counts for males were 0.72 (95%CI 0.41-1.28) and 0.5 (95% CI 0.23-1.09) times as a high compared to females, respectively. A statistically significant interaction between sex and anti-hypertensive treatment was present for total proximal and bifurcation plaque burdens (ratio of relative risk for proximal plaques = 2.02 [95% CI 1.05-3.89, p=0.04] and for bifurcation plaques = 3.02 [95% CI 1.2-7.6, p=0.02]). A similar trend was seen for total plaque and distal plaque burdens, although this did not reach statistical significance (Figure 2).Discussion
Among patients with AIS, hypertensive males have higher total plaque and proximal plaque burdens compared to hypertensive females. This sex-difference may be due to the protective effect of estrogen in females.3 Moreover, our results show a sex-effect among hypertensive patients with AIS who are treated with an anti-hypertensive medication compared to those who are not treated. The results suggest anti-hypertensive treatment has greater effects on hypertensive females than males and show a greater magnitude in the reduction in plaque burden in females than in males; this interaction effect between sex and treatment was statistically significant in proximal and bifurcation plaque burdens although a trend was seen with all assessed plaque burdens. The sex-effect with anti-hypertensive treatment may be partly explained by a differential density and sensitivity of sex hormone receptors on vascular smooth muscle cells, which have been described with differences in endothelium-independent dilatation between males and females.4Conclusion
Among hypertensive patients with AIS, hypertensive males have a significantly higher total plaque burden than females. These results suggest that different treatment guidelines for males versus females may help reduce ICAS burden and ultimately AIS risk. Future studies with larger samples sizes are warranted to validate whether differential management of hypertension for males versus females can reduce ICAS burden.Acknowledgements
None.References
[1] Gillis EE and Sullivan JC. Sex Differences in Hypertension: Recent Advances. Hypertension. 2016;68(6):1322-1327. [2] Veglio F, Paglieri C, Rabbia F, Bisbocci D, Bergui M, Cerrato P. Hypertension and cerebrovascular damage. Atherosclerosis. 2009;205: 331–341. [3] Mathur P, Ostadal B, Romeo F, Mehta JL. Gender-Related Differences in Atherosclerosis. Cardiovasc Drugs Ther. 2015;29(4):319-27. [4] Pabbidi MR, Kuppusamy M, Didion SP, Sanapureddy P, Reed JT, Sontakke SP. Sex Differences in vascular function and related mechanisms: role of 17B-estradiol. Am J Physiol Heart Circ Physiol. 2018;315(6):H1499-H1518.Figures
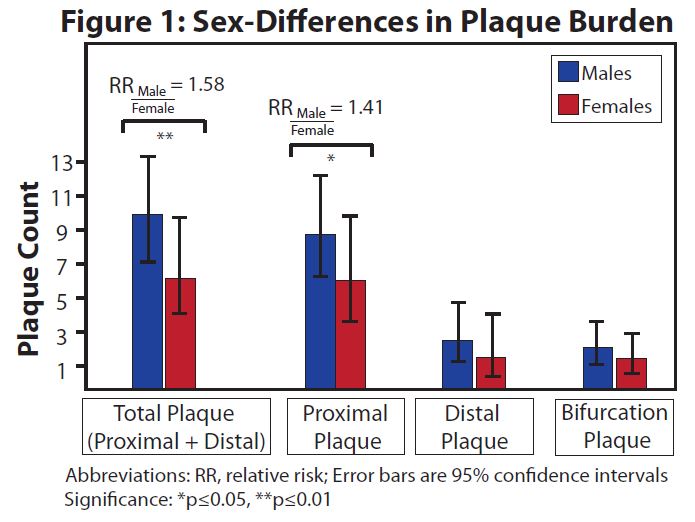
Sex-Differences in Plaque Burden Among Hypertensive Patients with Acute Ischemic Stroke
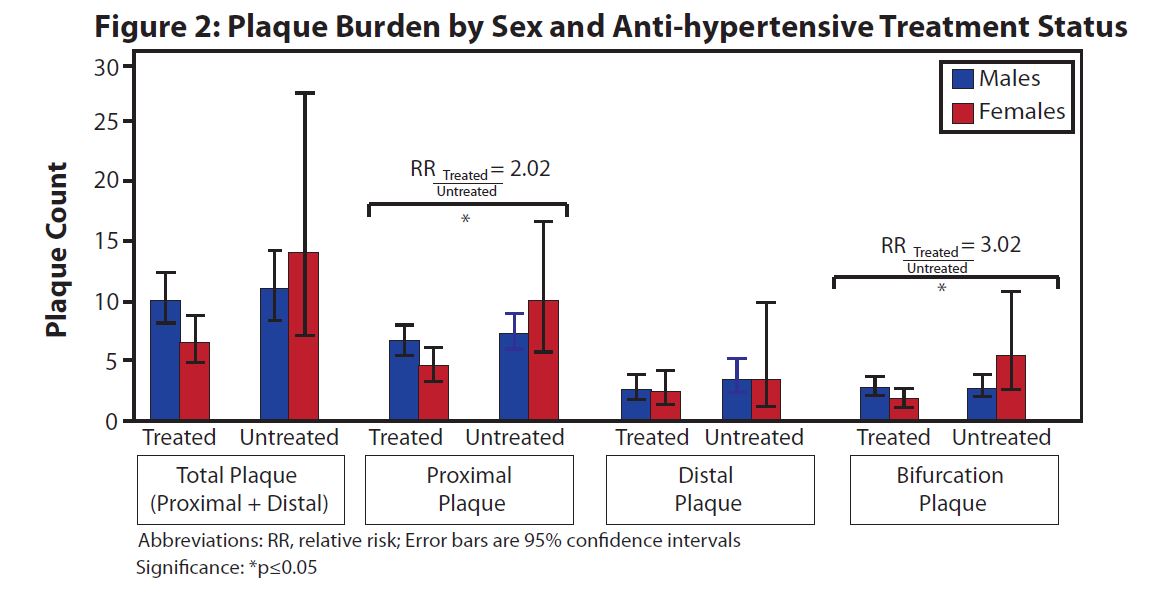
Plaque Burden by Sex and Anti-hypertensive Treatment Status
DOI: https://doi.org/10.58530/2022/0010