S90
Deep Inspiration Breath-Hold Radiotherapy does not induce MRI detectable LV functional and structural changes in patients with left-sided breast cancer – A six months follow-up1Queensland University of Technology, Brisbane, Australia, 2Translational Research Institute, Woolloongabba, Australia, 3Cardiology, Princess Alexandra Hospital, Brisbane, Australia, 4University of New South Wales, Sydney, Australia, 5Radiation Oncology, Princess Alexandra Hospital, Brisbane, Australia, 6The University of Queensland, St Lucia, Australia
Synopsis
The usefulness of T1 and ECV mappings in the context of radiation cardiotoxicity has yet to be studied. In the current study, we conducted a longitudinal CMR study on 30 females with left-sided breast cancer before and after Deep Inspiration Breast Hold (DIBH) radiotherapy (RT). The results showed patients who were treated with DIBH RT had no CMR detectable functional or structural myocardial changes 6 months following RT treatment. This has important implications on the long-term cardiac health of the growing number of women who are surviving or living with breast cancer.
Introduction
Breast cancer is the most common malignancy and leading cause of cancer-related death in women (1). Adjuvant radiation therapy (RT) following surgery reduces the risk of locoregional recurrence and improves survival. However, unintentional cardiac irradiation is associated with increased risk of long-term adverse cardiac effects including cardiomyopathy (2). Quantitative T1 mapping by cardiovascular MR (CMR) evaluates diffuse myocardial structural changes non-invasively using parameters such as T1 relaxation constant and extracellular volume (ECV) fraction. Both acute and prolonged elevations in ECV have been observed in anthracycline-induced cardiotoxicity (3). The usefulness of T1 and ECV mappings in the context of radiation cardiotoxicity has yet to be studied. The aim of this study was to evaluate early myocardial changes in women who underwent RT for left-sided breast cancer, using CMR T1 and ECV metrics.Research subjects
Institutional ethics approval and written informed consent were obtained. N=30 females with left-sided breast cancer requiring radiotherapy were recruited. Exclusion criteria included participants with significant coronary artery disease, history of myocardial infarction, arrhythmia, significant valvular disease, renal insufficiency (eGFR < 30ml/min/1.73m2), age <18 years and contradictions to MRI.Study protocol
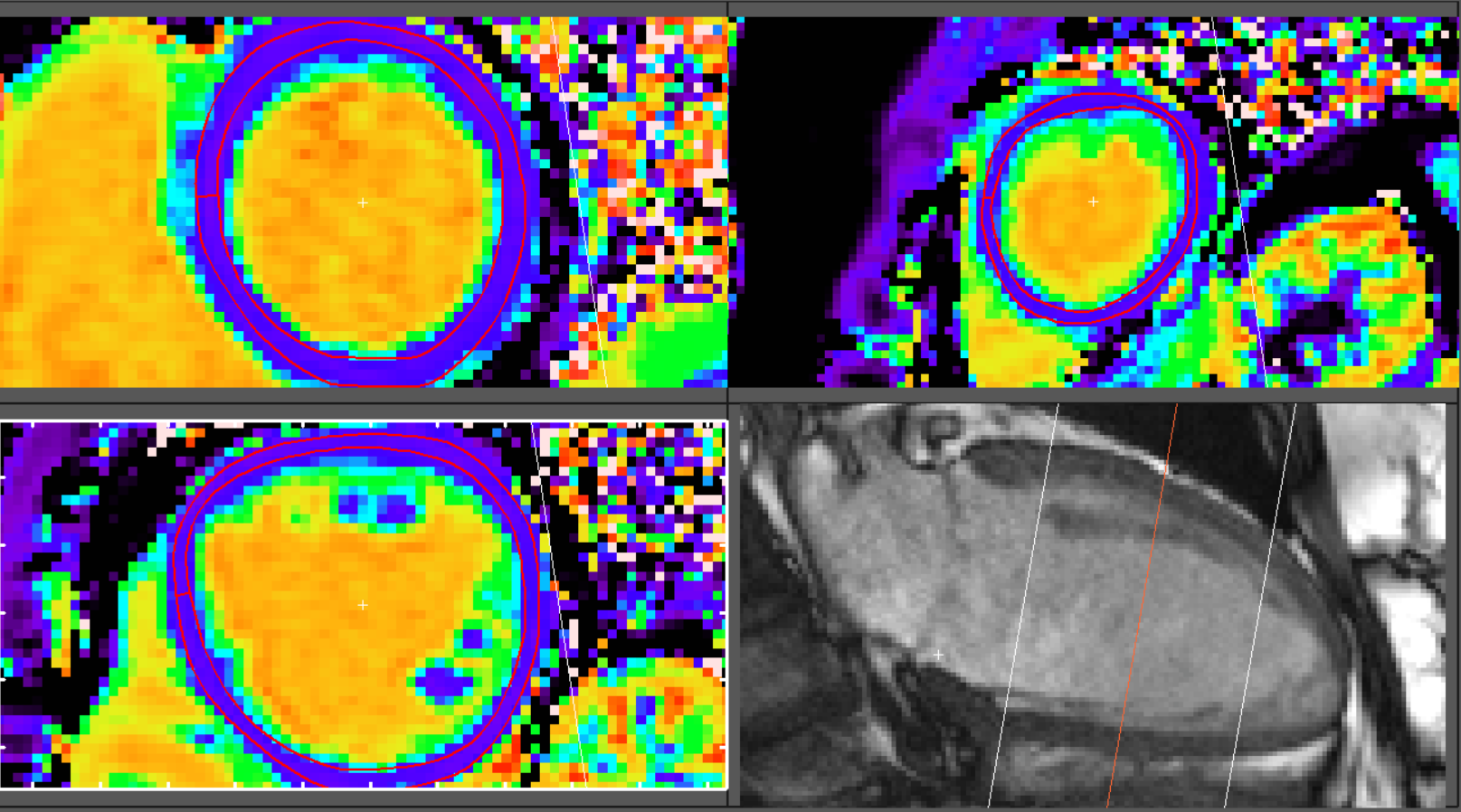
CMR examinations were performed on a 60cm 3.0T MRI system (Prisma, Siemens AG, Erlangen, Germany) using two 30-channel flex arrays. The scanning protocol included a stack of short-axis cine images covering the entire end-diastolic Left Ventricle(LV); pre- and 10 minutes post- contrast (Gadovist, Bayer, Germany, dose=0.2mmol/kg) modified MOLLI (MyoMaps, Siemens) in short-axis images at basal, mid, and apical levels; and 15minutes late gadolinium enhancement (LGE) images. All sequences were acquired with cardiac ECG gating and end-expiratory breath-hold. CMR was performed prior to commencement of radiation treatment and repeated 6 months post treatment. Blood samples were collected for haematocrit immediately before or after each CMR. All RT treatments were planned and performed on a breast board using Deep Inspiration Breath Hold (DIBH) technique as per our departmental protocol.Image analysis
Segment (v2.2 R6190, Medviso, Lund, Sweden) was used for image analysis. LV volume and Ejection Fraction (EF) were derived using short-axis cine stack. T1 mapping was generated offline using unprocessed MOLLI images. The ROIs were placed within manually segmented myocardium with a further 20% erosion in both endo- and epicardial directions. The equation for calculating the extracellular volume (ECV) is: $$$ECV=(1/(T1myo postgad)-1/(T1myo native))/(1/(T1blood postgad)-1/(T1blood native))×(1-hematocrit)Statistical analysis
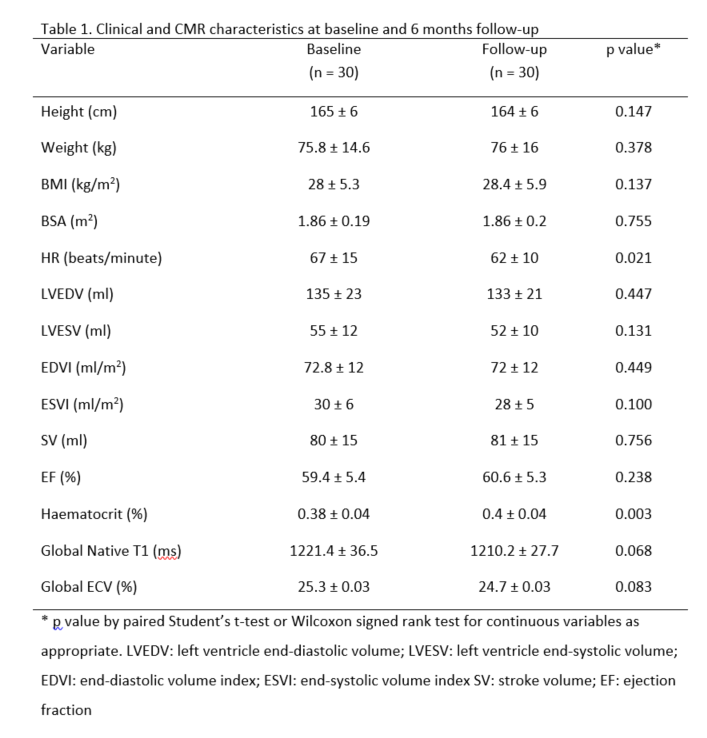
All continuous variables were tested for Gaussian distribution using the Kolmogorov-Smirnov test. The changes in LV were analysed by the paired Student’s t-test or Wilcoxon signed rank test. A two-tailed p value of <0.05 was considered significant. All statistical analyses were performed using SPSS for Windows version 25 (SPSS Inc.; Armonk, NY: IBM Corp).Results
All 30 patients (age = 56 ± 10) returned for their follow-up CMR with a mean inter-scan interval of 7.9 months. The average mean heart dose (MHD) was 1.83 ± 0.93 Gy. Table 1 outlines clinical and CMR characteristics of participants. No significant functional (EF) or structural (T1 and ECV) difference was found between baseline and 6 month post-treatment follow-up.Discussion
T1 mapping represents the longitudinal relaxation time and ECV reflects the volume fraction of extracellular matrix or interstitial space, both are objective measures of the myocardial integrity. Elevated ECV has been reported in cancer survivors following anthracycline exposure regardless of the presence of symptomatic cardiomyopathy (3). Similarly, Hatakenaka et al. were able to use MRI to demonstrate impaired LV function following concurrent chemoradiation for oesophageal cancer (4). However, in our breast cancer cohort, no CMR parameter was significantly changed. This may be explained by the fact that our cohort received significantly less cardiac radiation than previous reports. The cohort in the current study received 1.83 Gy MHD via the DIBH technique, as opposed to 5.2 Gy reported in a recent large-scale systematic review (5). Due to the linear relationship between the dose and the degree of cardiotoxicity, the potential myocardial changes were likely to be less in the DIBH cohort, and thus statistically insignificant. Furthermore, clinical manifestations of radiation induced cardiotoxicity (RIC) have been observed in the first 5 years following RT (6), whereas an image-based study using 2D speckle tracing echocardiography could identify a decline in LV strain as early as 6 weeks post RT (7). With variable latency in the development of cardiotoxic effects, it is not clear when the deregulation of the myocardial interstitium begins. Multiple time-point CMR studies may be of use to better understand the pathogenesis of RIC.Conclusions
The present pilot study showed patients who were treated with DIBH RT for left-sided breast cancer had no CMR detectable functional or structural myocardial changes 6 months following RT treatment. These results suggest that decreased radiation dose techniques, such as DIBH, may be beneficial in preventing radiation induced cardiac injury. This has important implications on the long-term cardiac health of the growing number of women who are surviving or living with breast cancer.Acknowledgements
No acknowledgement found.References
1. Ferlay J, Colombet M, Soerjomataram I, Mathers C, Parkin D, Piñeros M, et al. Estimating the global cancer incidence and mortality in 2018: GLOBOCAN sources and methods. International journal of cancer. 2019;144(8):1941-53.
2. Rygiel K. Cardiotoxic effects of radiotherapy and strategies to reduce them in patients with breast cancer: an overview. Journal of cancer research and therapeutics. 2017;13(2):186.
3. Jordan JH, Hundley WG. MRI of Cardiotoxicity. Cardiology Clinics. 2019;37(4):429-39.
4. Hatakenaka M, Yonezawa M, Nonoshita T, Nakamura K, Yabuuchi H, Shioyama Y, et al. Acute cardiac impairment associated with concurrent chemoradiotherapy for esophageal cancer: magnetic resonance evaluation. International Journal of Radiation Oncology* Biology* Physics. 2012;83(1):e67-e73. 5. Taylor C, Correa C, Duane FK, Aznar MC, Anderson SJ, Bergh J, et al. Estimating the risks of breast cancer radiotherapy: evidence from modern radiation doses to the lungs and heart and from previous randomized trials. Journal of Clinical Oncology. 2017;35(15):1641.
6. Darby SC, Ewertz M, McGale P, Bennet AM, Blom-Goldman U, Brønnum D, et al. Risk of ischemic heart disease in women after radiotherapy for breast cancer. New England Journal of Medicine. 2013;368(11):987-98.
7. Lo Q, Hee L, Batumalai V, Allman C, MacDonald P, Delaney GP, et al. Subclinical cardiac dysfunction detected by strain imaging during breast irradiation with persistent changes 6 weeks after treatment. International Journal of Radiation Oncology• Biology• Physics. 2015;92(2):268-76.
Figures