S80
A finding of Female Adnexal Tumour of probable Wolffian Origin (FATWO) on magnetic resonance imaging and histology - a rare neoplasm: Case report1Cape Universities Body Imaging Centre, University of Cape Town, Cape Town, South Africa, 2Department of Radiology, Morton & Partners Radiology, Cape Town, South Africa, 3Anatomical Pathology, Lancet Laboratories, Cape Town, South Africa, 4Division of Diagnostic Radiology, Groote Schuur Hospital and University of Cape Town, Cape Town, South Africa
Synopsis
We present the MRI and histological findings in a case of Female Adnexal Tumour of Wolffian Origin (FATWO) / WAT (Wolffian Adnexal Tumour), a rare adnexal neoplasm. This mass, located in the right broad ligament demonstrated diffusely low signal intensity on both T2WI and T1WI, peripheral restriction on DWI, peripheral enhancement and central hypo-enhancement post Gadolinium. An awareness of this condition and its MRI findings will ensure that appropriate immunohistochemical staining is performed. The presence of restriction may be helpful in predicting tumour behaviour, surgical approach and postoperative management.
Background
Female Adnexal Tumour of probable Wolffian Origin (FATWO) is a rare, diagnostically challenging neoplasm, believed to arise from the remnants of the mesonephric or Wolffian ducts.1,2,3,4 In males, these ducts are pivotal in the formation of the vas deferens. In females, they degenerate, but remain as attachments to the broad ligament or less commonly, to the lateral walls of the vagina or cervix.2,3,4 A literature search revealed fewer than 100 case reports of tumours originating in these vestigial tissues, in the rete ovarii, retroperitoneum and, rarely, in the ovary itself.4,5,6,7,8 Few of these reports include MR imaging. We present a 66-year old, asymptomatic woman who, on routine OBGY examination, was found to have a palpable, right adnexal mass. A solid tumour, presumed to be ovarian, was confirmed on in-room ultrasound. She had had an uncomplicated hysterectomy, without oophorectomy for perimenopausal bleeding 10 years previously. MRI was requested for further delineation, localization and associations.Magnetic Resonance Imaging
The patient was scanned on a 3T Siemens Magnetom Verio scanner (Erlangen, Germany), using an 18-channel body array coil, combined with a 32-channel spine coil. Sequences included: T2-weighted imaging (T2WI) in sagittal, axial and coronal planes (TR 7872; TE 89; field-of-view 150mm; slice thickness 4mm). T1-weighted (T1W) axial and coronal without and with contrast (TR 783; TE 13; slice thickness 7mm); Diffusion-weighted-imaging (DWI), with b-value of 800 and apparent diffusion coefficient (ADC) map.Findings
A solid right adnexal mass, measuring 38 x 35 mm x 50mm, was confirmed. The mass returned low signal on T2WI, with internal foci of high signal. On T1WI, the intralesional signal was homogeneously isointense to muscle. A well-defined low signal capsule was present on both T1 and T2WI. Restriction (high signal on b800 DWI and low signal intensity on the ADC map) was limited to the periphery of the tumour, with corresponding peripheral enhancement. Hypo-enhancement was observed centrally (Fig. 1). Based on the ultrasound findings, the mass was initially thought to have replaced the right ovary, favouring the diagnosis of an ovarian stromal or Kruckenberg tumour. On review of the MRI examination, small ovaries were identified bilaterally, which appeared normal for age and post-menopausal status. Minimal nonspecific free fluid was present in the pelvis superior to the vaginal vault. There was no adenopathy or peritoneal deposit and no osseous, bladder or rectal lesion was identified.Histology
This tumour presented a diagnostic challenge. It was comprised of both polygonal and spindled cells, which showed positive staining with the pan epithelial immunohistochemical marker and negativity with the sex cord stromal and smooth muscle markers. Initial impression was that this likely represented a metastasis, possibly from the breast, as the morphology would fit a lobular carcinoma. All immunohistochemical markers for a metastatic carcinoma proved negative. Further staining with CD 10 showed positive staining (Fig. 2). This combination of immunophenotype and the location of the tumour was diagnostic, for a Female Adnexal Tumour of probable Wolffian origin (FATWO).Teaching points
- Most adnexal/ ovarian neoplasms return high signal on T2WI- MRI findings may help in differentiating FATWO from other, more common adnexal masses
FATWO:
- Well defined with a low signal capsule
- Hypo-intense on both T1 and T2WI, suggesting hypercellularity, fibrous tissue and/or chronic blood products
- Peripheral restriction on DWI – suggesting cellularity
- Central hypo-enhancement – suggesting a central ‘scar’
Conclusion
Magnetic resonance imaging plays an important role in the delineation of soft tissue pelvic tumours and in surgical planning. MRI findings may, however, be non-specific. Given its rarity and the diagnostic challenges of routine histology, the diagnosis of FATWO may be elusive. The location of a mass in the broad ligament, in the setting of normal ovaries increases the likelihood of this diagnosis. Low signal on T2WI, peripheral restriction and a central hypoenhancing ‘scar’ on T1WI have not been previously described in this condition. The combination of these findings on MRI should raise suspicion for this diagnosis pre-operatively and guide appropriate immunohistochemical investigation of this uncommon condition.Keywords
Female Adnexal Tumour of Wolffian Origin (FATWO), Magnetic Resonance Imaging, Histology.Acknowledgements
Dr Katrien De Haeck (Surgeon)
Dr Joy Robinson (Surgeon)
References
1. Zhang, W., Valente, P.T. & Riddle, N.D. 2016. Female Adnexal Tumours of Probable Wolffian Origin with a Biphasic Histologic Growth Pattern and Positive for C-kit. Human Pathology: Case Reports. 4:46-49.
2. Bennett, J.A., Ritterhouse, L.L., Furtado, L.V., Lastra, R.R., Pesci, A., Newell, J.M., et al. 2019. Female adnexal tumours of probable Wolffian origin: morphological, immunohistochemical, and molecular analysis of 15 cases. Modern Pathology. 33(4):734–47.
3. Sato, T., Isonishi, S., Sasaki, K. et al. 2012. A case of female adnexal tumour of probable Wolffian origin: significance of MRI findings. International Cancer Conference Journal. 1:108–112.
4. Hübner, T.B., Schwab, M., Hartmann, E., Mayr, D., Thurner, A., Bley, T., Wöckel, A. & Herr, D. 2019. Female Adnexal Tumour of Probable Wolffian Origin (FATWO): Review of the Literature. Geburtshilfe Frauenheilkd. 79(3):281-285.
5. Li, C.C, Qian, Z.R. & Hirokawa, M. et al. 2004. Expression of adhesion molecules and Ki-67 in female adnexal tumour of probable Wolffian origin (FATWO): report of two cases and review of the literature. APMIS: Acta Pathologica, Microbiologica, et Immunologica Scandinavica. 112(6):390-398. 6. Harada, O., Ota, H., Takagi, K., et al. 2006. Female adnexal tumour of probable Wolffian origin: morphological, immunohistochemical, and ultrastructural study with c-kit gene analysis. Pathology International. 56(2):95-100.
7. Shalaby, A. & Shenoy, V. 2020. Female Adnexal Tumour of Wolffian Origin: A Review. Archives of Pathology and Laboratory Medicine. 144(1): 24-28.
8. Matsuki, M., Kaji, Y. & Matsuo, M. 1999. Female adnexal tumour of probable Wolffian origin: MR findings. British Journal of Radiology. 72:911-913
Figures
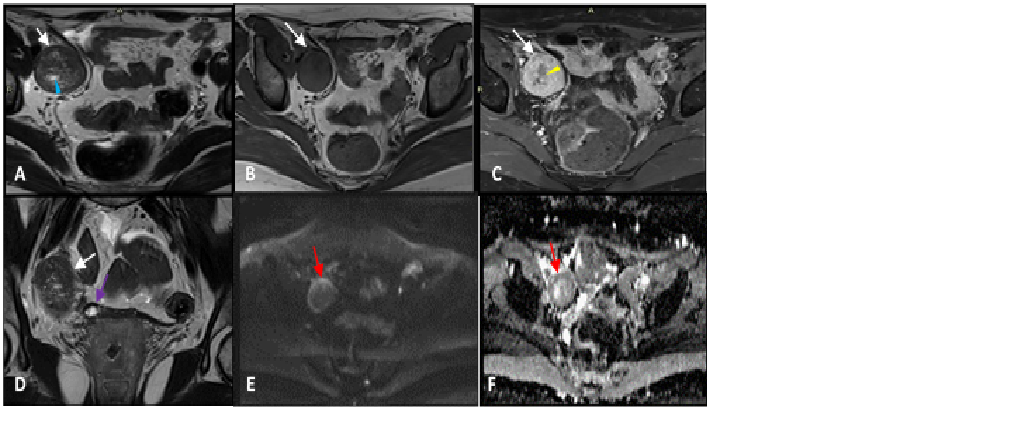
Figure 1:MRI features of FATWO in a 66-year old woman A: T2W axial shows right adnexal mass (white arrow) displaying areas of high signal intensity (light blue arrow). B: T1W axial shows lesion, with homogeneous low signal intensity (white arrow) C: T1W axial post-contrast shows homogeneous peripheral enhancement (white arrow), with central hypo-enhancement (yellow arrow) D: T2W coronal showing lesion (white arrow), in relation to right ovary (purple arrow) E: DWI shows high signal intensity at the rim of the lesion (red arrow) F: ADC map shows restricted diffusion (red arrow)
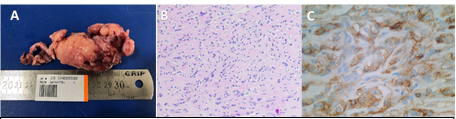
Figure 2: Specimen of resected mass and its histological appearance A: Specimen measuring 65x35x30mm. The surface has a fairly well circumscribed nodular appearance B: Microscopic specimen haematoxylin and eosin (H&E) tissue stain showing polygonal cells C: Microscopic specimen: Positive staining with Cell Development marker (CD10)