S7
Optimized 3D ultrashort TE protocol for lung imaging1Cardiology, Johns Hopkins University, Baltimore, MD, United States, 2Canon Medical Research, Cleveland, OH, United States, 3Radiology, Johns Hopkins University, Baltimore, MD, United States, 4Biomedical Engineering, Johns Hopkins University, Baltimore, MD, United States, 5Canon Medical Systems Corporation, Otawara, Japan
Synopsis
3D radial Ultrashort echo time sequence is a promising technique for lung imaging but the protocol has not been optimized. We examined the parameters including number of trajectories and flip angles using a lung phantom. In-vivo images were obtained and evaluated based on the parameters optimized in the phantom study. UTE acquisition in axial rather than coronal direction produced better quality of images. Breath holding acquisition may be an option in case patients cannot tolerate long scan time.
Background
Ultrashort echo time (UTE) sequence has been used to detect tissues with a short T2* relaxation time. Many studies have been conducted to investigate the usefulness of UTE in lung imaging [1]. MRI is not suitable in evaluating lung parenchyma, and CT imaging is the gold standard. However, CT imaging needs X-ray exposure, which creates resistance to follow up exam. For that reason, much interest has been focused on MRI imaging of the lung parenchyma without X-ray exposure. However, the parameters of lung UTE have not been optimized. Most of the clinical images are performed on coronal plane [2] and reconstructed to axial images to compare with the reference CT image. Therefore, we aimed to optimize the lung UTE protocol using the lung phantom and evaluate in human study.Methods
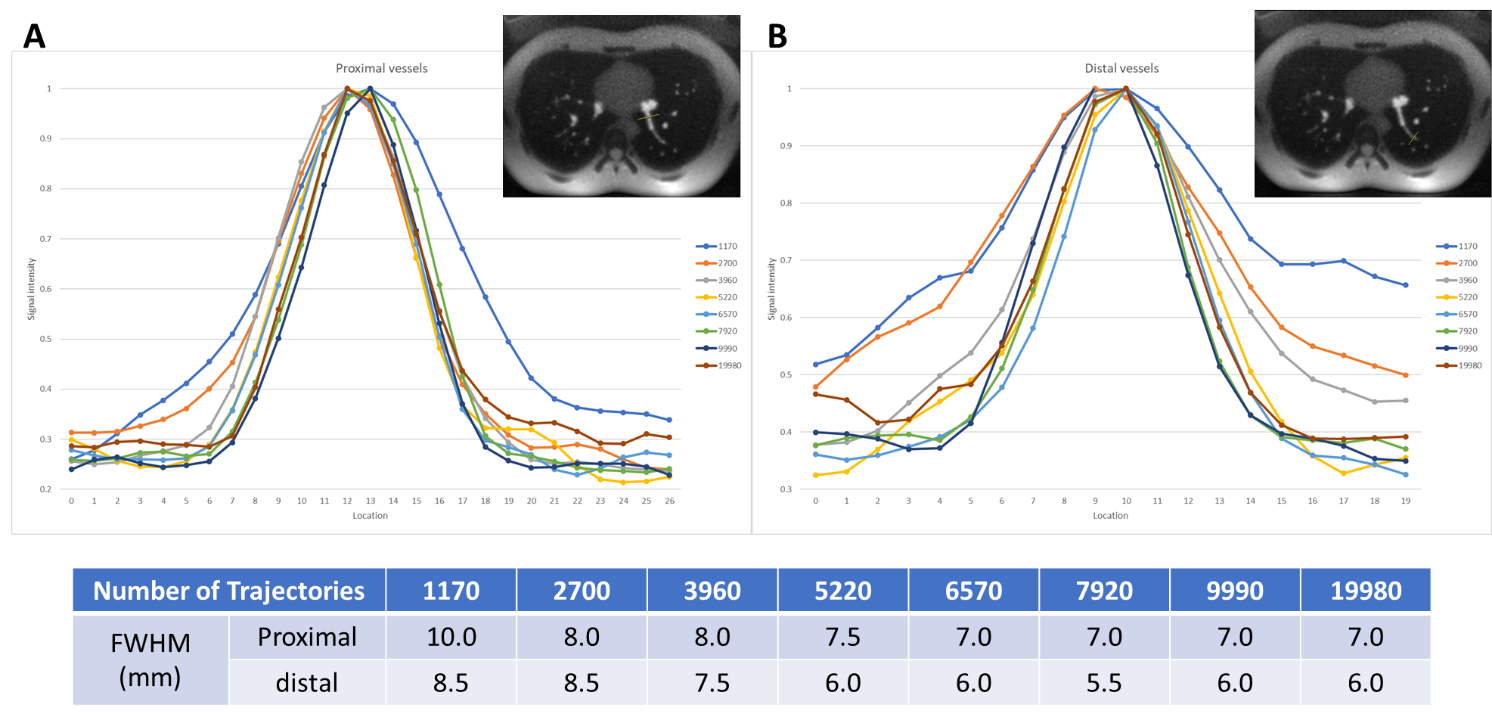
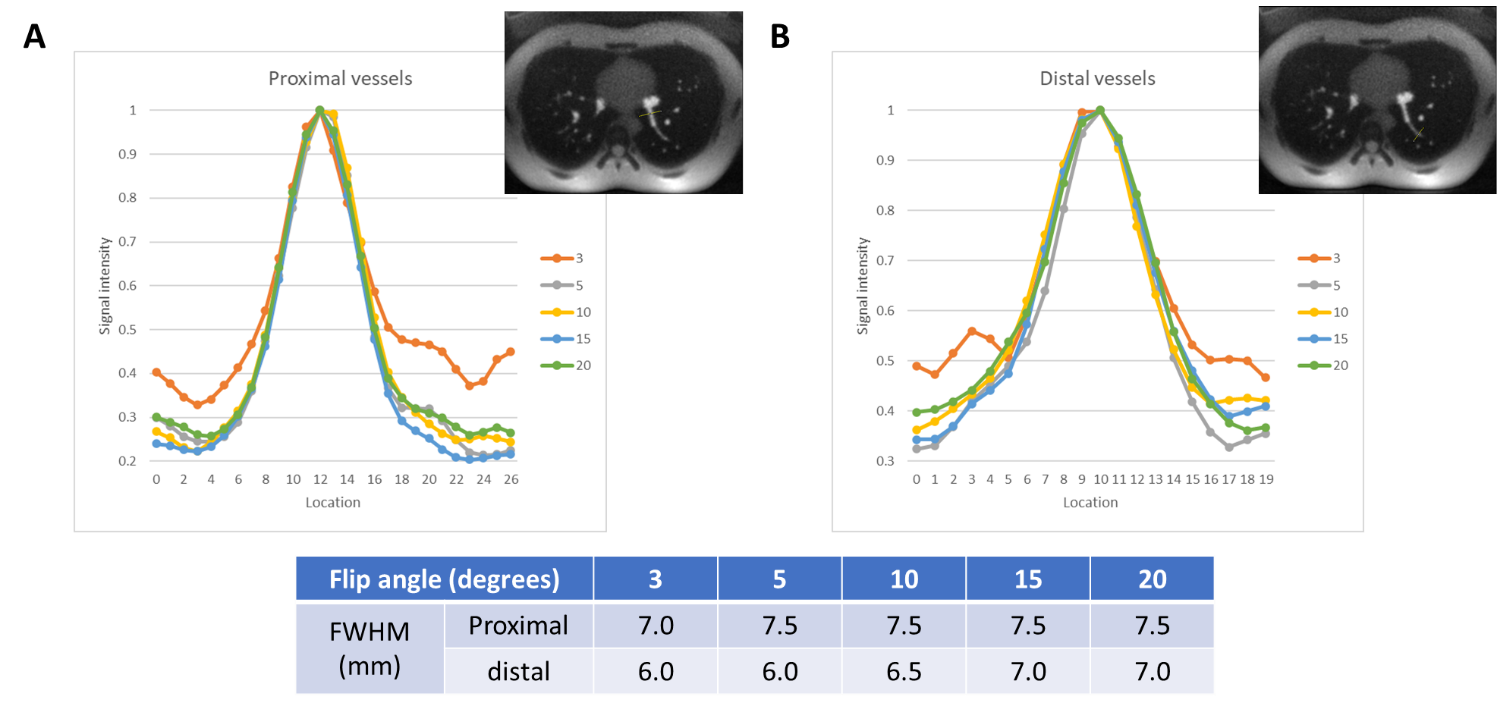
Images of the lung phantom (produced by Kyoto Kagaku Co., Ltd.) were acquired using 3D radial UTE sequence that using various parameters including a) number of trajectories; 1170, 2700, 3960, 5220, 6570, 7920, 9990, 19980. b) flip angle; 3, 5, 10, 15, 20. Imaging protocol was TR = 3.7 ms, TE = 0.096 ms, Field of view = 400 x 400 mm2, Matrix = 400 x 400, Slice thickness = 1 mm, Bandwidth = 488 Hz/Px. The number of acquisitions was set to 20 to obtain a higher signal. Signal profile and full width at half maximum (FWHM) from pseudo vessels were evaluated for qualitative comparison of image sharpness. Three normal volunteers were scanned with the following UTE protocol. a) Coronal acquisition with respiratory gating. b) Axial acquisition with respiratory gating. c) Axial acquisition with breath holding in expiration. d) Axial acquisition with breath holding in inspiration. The images obtained in the coronal orientation were reconstructed into the axial plane for comparison. All experiments were performed in a 3.0T system (Vantage Galan, Canon Medical Systems, Japan).Results
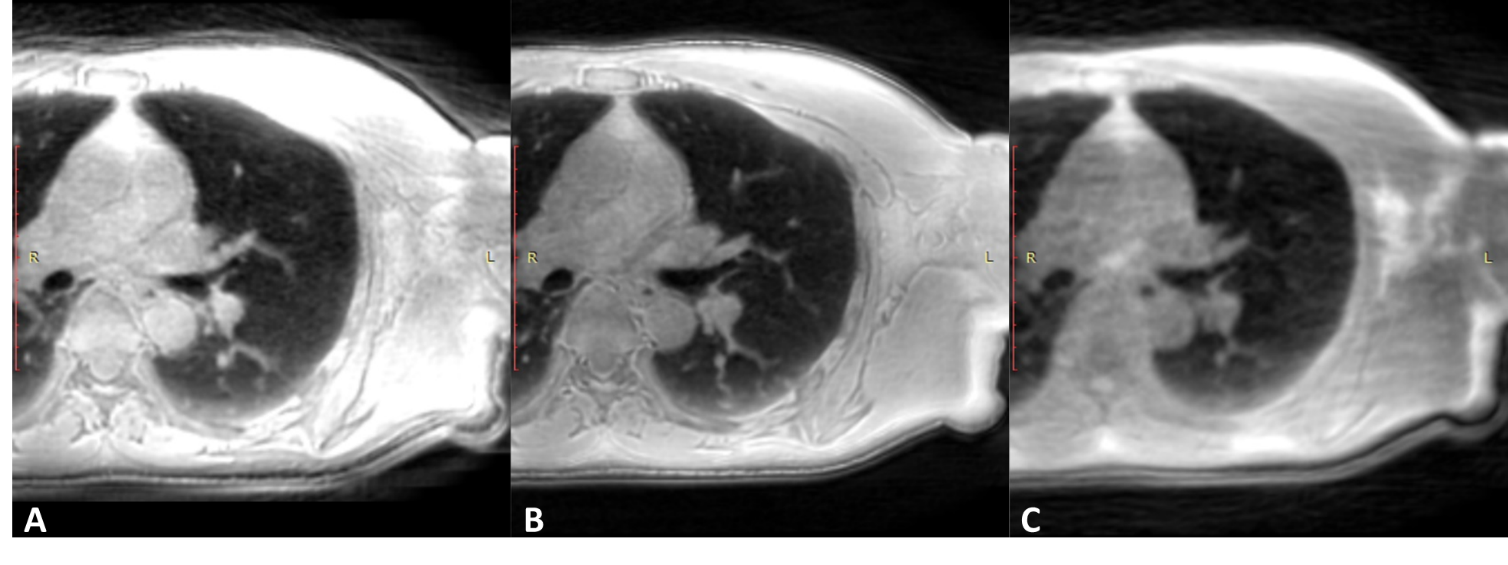
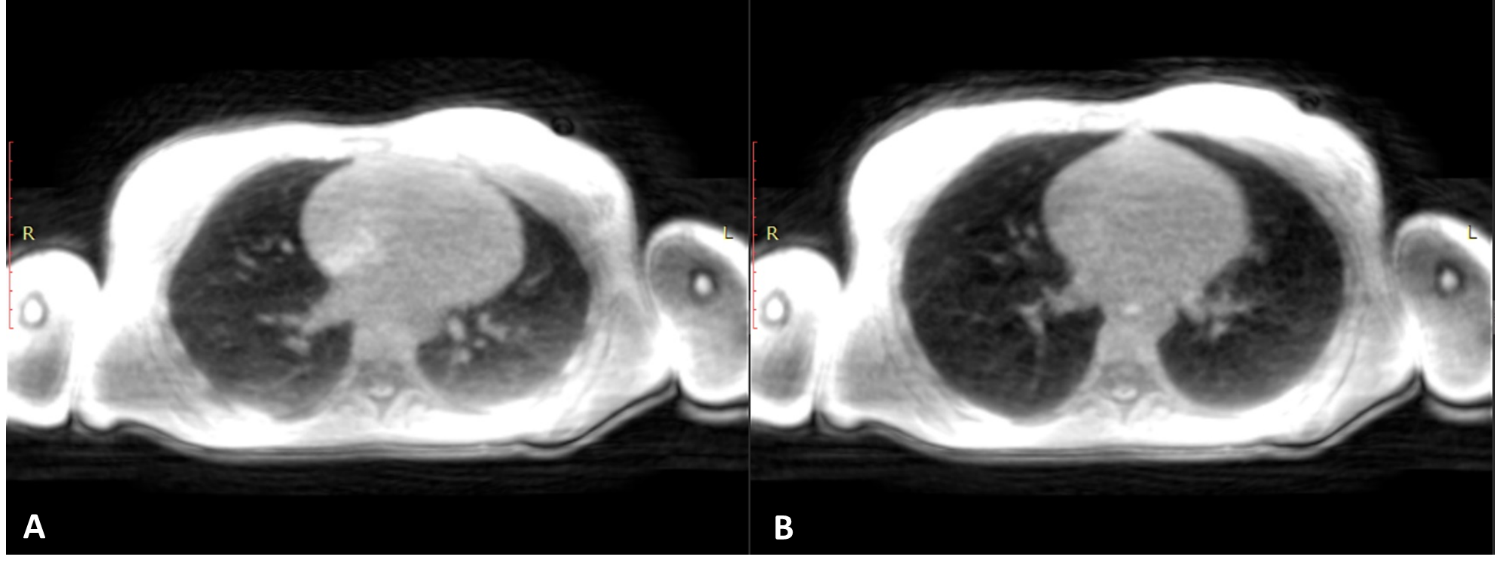
Figure 1 demonstrates signal profile at vessels of lung phantom among each number of trajectories. The lower the number of trajectories the larger the FWHM value. However, when the number of trajectories is over 5220, the FWHM became almost constant. Figure 2 demonstrates signal profile at vessels of lung phantom among each flip angle. The FWHMs were similar with respect to flip angles. Figure 3 demonstrates human lung images using UTE sequence by different acquisitions. Each acquisition was performed using 5º flip angle. The number of trajectories were 48820 for respiratory gating, 5220 for breath holding, respectively. Acquisition time were 11 min 39 seconds in coronal acquisition with respiratory gating, 6 min 55 seconds in axial acquisition with respiratory gating, and 20 seconds in axial acquisition with breath holding, respectively. Comparing the peripheral blood vessels in the lung, axial orientation with respiratory gating produced sharper images than any other acquisitions. Figure 4 demonstrates human lung images using UTE sequence by breath holding. In the inspiration acquisition, lung parenchyma was better showed than in expiration.Conclusion
We recommend using 5º flip angle with more than 5220 number of trajectories in 3D radial UTE acquisitions. UTE acquisition in axial rather than coronal direction produced better quality of images. Breath holding acquisition in expiration may be an option in case patients cannot tolerate long scan time.Acknowledgements
We gratefully acknowledge the work of past and present members of our laboratory.References
1. Gai ND, Malayeri A, Agarwal H, Evers R, Bluemke D: Evaluation of optimized breath-hold and free-breathing 3D ultrashort echo time contrast agent-free MRI of the human lung. Journal of Magnetic Resonance Imaging 2016:1230–1238.
2. Huang Y-S, Niisato E, Su M-YM, et al.: Detecting small pulmonary nodules with spiral ultrashort echo time sequences in 1.5 T MRI. Magnetic Resonance Materials in Physics, Biology and Medicine 2020.
Figures