4310
Diffusion MRI and fibertracking of brachial plexus to diagnose injury1Centre for Advanced Imaging, The University of Queensland, St Lucia, Australia, 2Siemens Healthcare, Brisbane, Australia, Brisbane, Australia, 3Metro North Hospital and Health Service, Brisbane, Australia, 4Application Department, Siemens Shenzhen Magnetic Resonance Ltd, Shenzhen, China, 5School of Clinical Sciences, Queensland University of Technology, Brisbane, Australia, 6Department of Radiology, Princess Alexandra Hospital, Brisbane, Australia, 7Jamieson Trauma Institute, Metro North Hospital and Health Service, Brisbane, Australia, 8Orthopaedics Department, Royal Brisbane and Women’s Hospital, Brisbane, Australia, 9Orthopedics Department, Royal Brisbane and Women’s Hospital, Brisbane, Australia
Synopsis
We describe the utility, optimization of a diffusion weighted imaging protocol, and the post-processing for fibertracking reconstruction of the brachial plexus nerve at 3T using a prototype Simultaneous Multi-Slice RESOLVE Diffusion-Weighted Imaging (SMS RESOLVE DWI) sequence. Best tractography profile was obtained for the acquisition acquired at 2.7 mm isotropic 3D resolution, using 7 segmentations, and 30 diffusion encoding directions at b-value of 800 s/mm2, combined with tractography reconstruction using a probabilistic tensor algorithm.
INTRODUCTION
The brachial plexus (BP) consists of nerve fibers that originate from the cervical spinal cord to the shoulder, arm, and hand. The BP structures can be traditionally imaged using a fat-saturated T2-weighted Short Inversion Time Inversion Recovery (3D-STIR) sequence. The STIR image, however, is difficult to assess the structural integrity of injured BP, as damaged nerves can often appear normal. However, changes in water diffusion is typically correlated with nerve impairment, which can be imaged using diffusion MRI.1 This information is critical to determine if surgical intervention will be required to restore function, or if the nerve is still reasonably intact such that it may be safely allowed to recover.DTI of the BP2,3 is challenging due to the large FOV relative to the small size of the nerve, the presence of physiological motion and the proximity of the FOV to B0 field inhomogeneity near the lungs. The aim of this study was to optimize a prototype Simultaneous Multi-Slice Readout Segmentation of Long Variable Echo-trains Diffusion-Weighted Imaging (SMS RESOLVE DWI) sequence4,5 to tackle the challenges in imaging the BP. Readout segments in the RESOLVE sequence are used to reduce the echo time (and thereby reducing local field inhomogeneity artefacts near the bones and the lung), while maintaining minimal motion artefacts to achieve good quality of DWI data. Here we describe the effects of parameter optimization in the SMS RESOLVE DWI sequence to the quality of BP fibertracking.
METHODS
MRI was performed using a MAGNETOM Prisma 3T (Siemens Healthcare, Erlangen, Germany) using a 64-channel head/neck and 18-channel body array receiver coils at the Herston Imaging Research Facility. Optimization was performed using 5 healthy participants, with varying BMI. The scan protocol included:A) a STIR 3D Space sequence (coronal, TR/TE/TI=3000/254/230ms, matrix=384×252×80, image resolution=0.78×0.78×1.5 mm; and
B) a prototype SMS RESOLVE DWI with variable parameters TR=1710-2230 ms, TE=47-50 ms, coronal or oblique axial orientations, 2.2–3.0 mm in-plane or 3D isotropic image resolutions, multiband acceleration factor 2, in-plane GRAPPA acceleration 2, number of segments 7-9, a single b=0, 20 diffusion encoding directions of 2 averages or 30 directions at b=800 s/mm2. The acquisition time of each DWI scan took ~11 mins or less. Automatic and region-specific volume shimming were trialed.
Diffusion data were preprocessed using MRTrix ver.0.3.2 dwifslpreproc6 pipeline. Seeding ROIs were created on the left and right cervical nerve roots with 100 random seeds per voxel in each of the seeding ROIs, and target ROIs were placed in the mid-shoulder regions. Fibertracks were generated using the tensor probabilistic algorithm.7
RESULTS
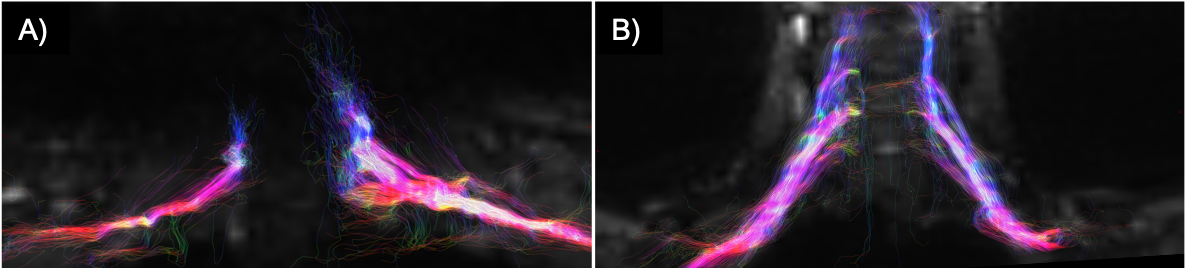
Figure 1 showed that B0 shimming significantly affected the quality. This problem was often observed in larger participants, where the automated shim adjustment volume erroneously optimized the shoulder region, resulting in reduced signal from the neck area. A region-specific shim volume that tightly encompasses brachial plexus and avoids anterior lung provided superior results.Figure 2A and B shows results from 2.7 and 3.0 mm isotropic 3D resolutions, respectively. The higher image resolution was required to reconstruct good quality tracts. Images acquired in an oblique axial orientation had a shorter TE due to the smaller phase FOV. This orientation allowed imaging at a higher (2.2×2.2×2.4 mm) resolution, resulting in longer and higher number of tracts (Figure 2C).
The TE could be reduced further with in-plane GRAPPA (phase encoding lines skipped) and higher number of readout segments (increasing from 7 to 9 segments). However, increasing the number of segments appeared to worsen the tract quality. This is probably resulting from motion artifacts (data not shown) associated with the increased length of scan.
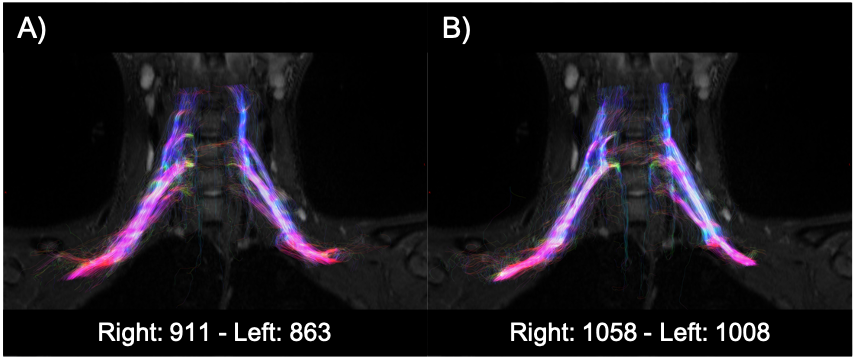
Comparison between BP tracts reconstructed from data acquired with 20×2 and 30×1 diffusion encoding directions (both with 2.7 mm isotropic 3D image resolution and similar scan time), shown in Figure 3A and 3B respectively, indicated that the higher number of directions produced approximately 16% more tracts (Figure 3). This is likely due to improved tensor definition and improved quality of fibertracking in turning regions.
DISCUSSION
Our results showed that the segmented SMS RESOLVE DWI sequence with protocol optimisation can provide high-quality visualisation of the brachial plexus and its entry point (the roots) into the spinal cord with a reasonable scan time. The number of readout segments scales negatively with acquisition time, thus increasing the risk of patient motion beyond what can be tackled by the advanced techniques provided by the prototype sequence. This potential problem highlights the importance of patient positioning and immobilisation during the scan. The oblique orientation allowed a unilateral examination of the BP, but it may be less useful in the clinic as it could not simultaneously provide a contralateral measurement. Further development will include optimization on shimming and fat saturation strategy, and measurement of reproducibility using test-retest experiments.CONCLUSION
Our results indicate that the brachial plexus can be reconstructed reliably with SMS RESOLVE DWI in a relatively short acquisition time, which is suitable for clinical imaging for the diagnosis of nerve injury. Future studies will use this technique to measure brachial plexus integrity in patients with and without clear root avulsion.Acknowledgements
The authors acknowledge the 3T T MRI facility and scientific and technical assistance of the National Imaging Facility, a National Collaborative Research Infrastructure Strategy (NCRIS) capability, at the Herston Imaging Research Facility.References
1. Lehmann, H. C., Zhang, J., Mori, S. & Sheikh, K. A. Diffusion tensor imaging to assess axonal regeneration in peripheral nerves. Exp Neurol 223, 238-244, doi:10.1016/j.expneurol.2009.10.012 (2010).
2. Ho, M. J. et al. Diffusion Tensor Imaging of the Brachial Plexus: A Comparison between Readout-segmented and Conventional Single-shot Echo-planar Imaging. Magn Reson Med Sci 18, 150-157, doi:10.2463/mrms.mp.2018-0004 (2019).
3. Wade, R. G. et al. Diffusion Tensor Imaging for Diagnosing Root Avulsions in Traumatic Adult Brachial Plexus Injuries: A Proof-of-Concept Study. Front Surg 7, 19, doi:10.3389/fsurg.2020.00019 (2020).
4. Porter, D. A. & Heidemann, R. M. High resolution diffusion-weighted imaging using readout-segmented echo-planar imaging, parallel imaging and a two-dimensional navigator-based reacquisition. Magn Reson Med 62, 468-475, doi:10.1002/mrm.22024 (2009).
5. Setsompop, K. et al. Blipped-controlled aliasing in parallel imaging for simultaneous multislice echo planar imaging with reduced g-factor penalty. Magn Reson Med 67, 1210-1224, doi:10.1002/mrm.23097 (2012).
6. Andersson, J. L. R. & Sotiropoulos, S. N. An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging. Neuroimage 125, 1063-1078, doi:10.1016/j.neuroimage.2015.10.019 (2016).
7. Jones, D. K. Tractography gone wild: probabilistic fibre tracking using the wild bootstrap with diffusion tensor MRI. IEEE Trans Med Imaging 27, 1268-1274, doi:10.1109/tmi.2008.922191 (2008).
Figures