4246
PETRA subtraction-based MRA to assess middle-cerebral-artery stenosis before and after treatment with angioplasty1The first Affiliated Hospital of Zhengzhou University, Zhengzhou, China, Zhengzhou, China, 2MR Collaboration, Siemens Healthcare Ltd., Beijing, China, Beijing, China, 3Department of Radiology, University of Washington, Seattle, Seattle, WA, United States
Synopsis
This study investigated the feasibility of PETRA-MRA to evaluate stent angioplasty of middle-cerebral-artery stenosis before and after treatment. PETRA-MRA was shown to significantly reduce susceptibility artifacts induced by metallic devices, decrease the phase dispersion of labeled flow, and increase the signal intensity within the stent. Compared to TOF-MRA, PETRA-MRA has better consistency with DSA in image quality and stenosis measurement, especially for follow-up assessments after stent angioplasty.
Introduction
The aim of this study was to assess the value of an ultra-short-echo-time (UTE) sequence, pointwise encoding time reduction with a radial acquisition (PETRA), in subtraction-based magnetic resonance angiography (MRA). This was performed during follow-up visits of patients who had prior stent angioplasties to relieve middle-cerebral-artery (MCA) stenosis. PETRA-MRA was also compared with time-of-flight (TOF) MRA, using digital subtraction angiography (DSA) as a reference.Methods
Following informed consent, fifty-three patients (n=53, 15 females and 38 males, mean age 52.4±9.1years) with MCA stenosis were enrolled in this study. Of these patients, 43% (n=23, 9 females and 14 males, mean age 52.8±9.9years) also had stent angioplasties performed. All patients underwent TOF-MRA, PETRA-MRA, and DSA examinations. MRI was acquired on a 3-Tesla MRI system (MAGNETOM Prisma, Siemens Healthcare, Erlangen, Germany). According to preoperative findings, the image quality of both MRA images was estimated using a 4-point scale. Following surgery, scoring of both susceptibility artefact intensity and flow signal within the stent were performed using a 4-point scale. The degree of stenosis was measured according to Samuels, the Dstenosis is the diameter of the lumen at the stenosis site, and the Dnormal is the diameter of the lumen at the proximal normal segment, using DSA as a reference.Stenosis%=[1-Dstenosis÷Dnormal]×100%
Wilcoxon signed-rank test was used to compare the mean scores for each MRA technique. The linear relationship between measurements of stenosis from both MRA techniques and DSA was evaluated by calculating Spearman’s correlation coefficient (r). Differences between the stenosis measurements using PETRA-MRA and TOF-MRA and between the two observers were assessed using Bland-Altman analysis, and the intra-class correlation coefficient (ICC) was used to quantify the agreement between MRA techniques.
Results
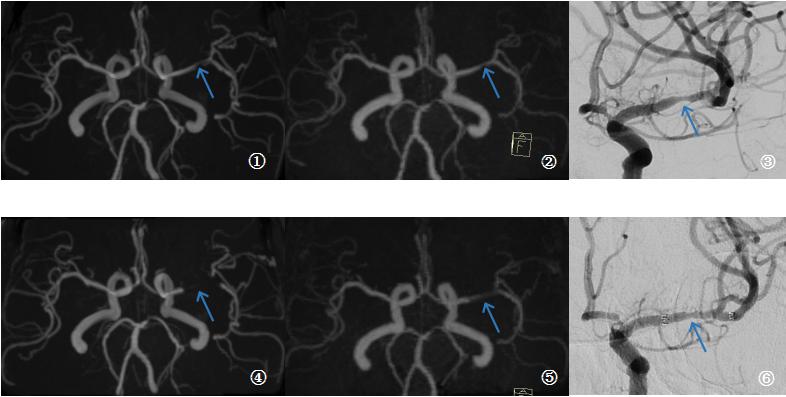
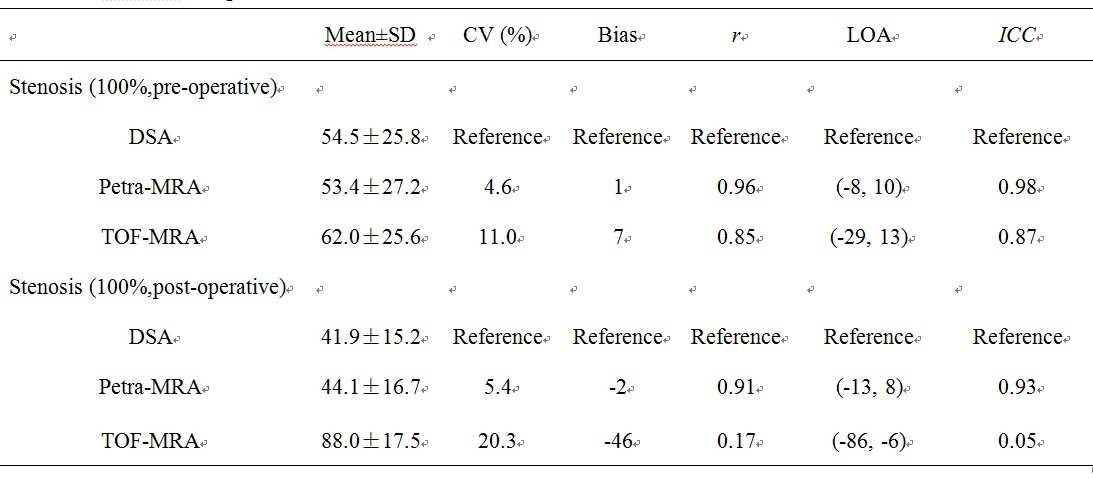
Example results and scoring for a patient both before and after stent treatment are shown in Figure 1. Results for comparison between MRA techniques and DSA are shown in Table 1. There was excellent interobserver agreement between the two readers for degree of stenosis on PETRA-MRA (ICC= 0.96), TOF-MRA (ICC = 0.94), and DSA (ICC = 0.96). For preoperative and postoperative assessments, the image quality, flow visualization within the stents, and susceptibility artifact intensities of PETRA-MRA were all significantly better than those of the TOF-MRA (3.87 ± 0.34 vs. 3.38 ± 0.65, P<0.001; 3.35 ± 0.57 vs. 1.61 ± 0.83, P<0.001; and 3.30 ± 0.63 vs. 1.48 ± 0.66, P<0.001, respectively); at the same time, the ratings of the two readers were very consistent (ICC (PETRA-MRA) = 0.92, ICC (TOF-MRA) = 0.74; ICC (PETRA-MRA) = 0.83, ICC (TOF-MRA) = 0.93; ICC (PETRA-MRA) = 0.89, ICC (TOF-MRA) = 0.91). When comparing PETRA-MRA and TOF-MRA of preoperative and postoperative assessments, the former was more consistent with DSA images (r (PETRA-MRA, preoperative) = 0.96, r (TOF-MRA, preoperative) = 0.85; r (PETRA-MRA, postoperative) = 0.91, r (TOF-MRA, postoperative) = 0.17).Discussion & Conclusion
Evaluation of stenosis after stent placement is challenging for other imaging techniques, such as CT, CE-MRA, and TOF-MRA, due to beam hardening artifacts or magnetic susceptibility artifacts. PETRA-MRA utilizes UTE, which enables significant reduction of susceptibility artifacts and signal voids due to turbulence. It has been successfully used for the evaluation of intracranial aneurysms after stent-assisted coil embolization and the evaluation of other cerebral-artery diseases. We showed that when compared with TOF-MRA, PETRA-MRA had higher image quality and accuracy in depicting MCA stenoses and could be a useful technique for follow-up in patients who have undergone stent angioplasty for MCA stenosis.Acknowledgements
We thank Yong Zhang for helpful discussions.References
1. Shang S, Ye J, Dou W, Luo X, Qu J, Zhu Q, et al. Validation of Zero TE-MRA in the Characterization of Cerebrovascular Diseases: A Feasibility Study. AJNR Am J Neuroradiol. 2019;40(9):1484-90.2. Shang S, Ye J, Luo X, Qu J, Zhen Y, Wu J. Follow-up assessment of coiled intracranial aneurysms using zTE MRA as compared with TOF MRA: a preliminary image quality study. Eur Radiol. 2017;27(10):4271-80.3. Samuels OB, Joseph GJ, Lynn MJ, Smith HA, Chimowitz MI. A standardized method for measuring intracranial arterial stenosis. AJNR Am J Neuroradiol. 2000;21(4):643-6.4. Schmalbrock P, Yuan C, Chakeres DW, Kohli J, Pelc NJ. Volume MR angiography: methods to achieve very short echo times. Radiology. 1990;175(3):861-5.5. Robson MD, Gatehouse PD, Bydder M, Bydder GM. Magnetic resonance: an introduction to ultrashort TE (UTE) imaging. Journal of computer assisted tomography. 2003;27(6):825-46.
Figures