4245
Prototype Platform for Real-time MR-guided Brain Clot Evacuation1Medical Physics, University of Wisconsin-Madison, Madison, WI, United States, 2Neurological Surgery, University of Wisconsin-Madison, Madison, WI, United States
Synopsis
The international Phase III MISTIE Trial, which used CT-image guidance to position a catheter at the site of intracerebral hemorrhage (ICH) failed to meet its clinical endpoint for all patients. The Trial concluded that improved guidance was needed to help a wider set of neurosurgeons. MR-guidance of ICH evacuation could meet these needs. We present an MR-guidance prototype to provide neurosurgeons with a real-time interface with similar viewpoints as commonly used in stereotactic operating room settings. The MR-guidance prototype shows potential to be a reliable tool to assist as monitoring and guiding tools and lysing drugs during clot-evacuation procedures.
Introduction
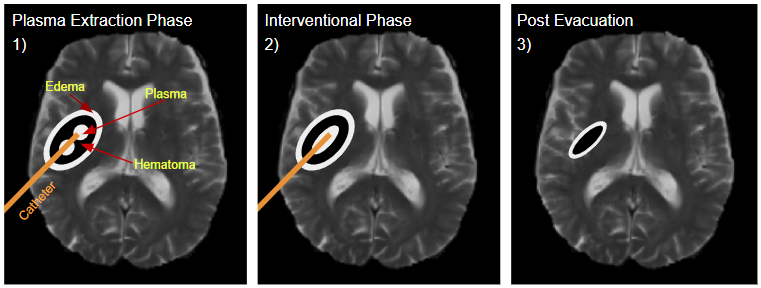
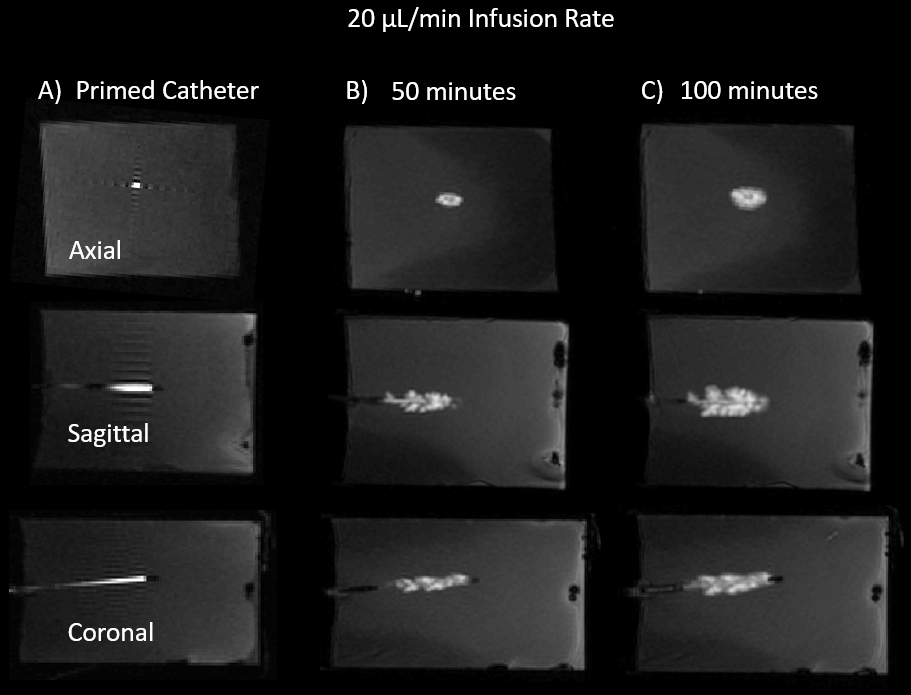
The international Phase III MISTIE Trial, which used CT-image guidance to position a catheter at the site of intracerebral hemorrhage (ICH) for periodic clot drainage and infusion of thrombolytic drugs (Fig. 1), failed to meet its clinical endpoint for all patients. However, a subset of patients whose interventions left less than 15 ml of residual clot volume showed statistically significant reductions in morbidity and increased independence[1]. The Trial concluded that improved guidance was needed to help a wider set of neurosurgeons meet the 15 ml residual volume goal without endangering rebleeds. MR-guidance of ICH evacuation could meet these needs, as envisioned in Figure 1. We have previously presented methodologies indicated that MR-guidance of lysing blood clots in ex-vivo models could accelerate clot evacuation while providing the guidance to assure neurosurgeons that they weren’t interfering with clot boundaries with normal brain tissue[2]. Co-infused Gd with the clot-busting drugs allowed easy visualization of the spatial distribution of the clot buster drug (rtPA) within the clot, as shown in Fig. 2. We present here an MR-guidance prototype that is designed to allow neurosurgeons to periodically assess and alter the clot evacuation by manipulating catheter position, adding rtPA, and spatially visualizing the delivery and distribution of the clot buster with respect to normal brain tissue. The prototype is designed to provide neurosurgeons with an interface with similar viewpoints as commonly used in stereotactic operating room settings using popular commercial surgical workstations, such as the Medtronic Stealth or Brainlab platforms.Methods
We used the HeartVista RTHawk interventional platform[3], as it allows us to design the interventional guidance without knowing specific software constructs or data pathways on the commercial scanner. RTHawk also allows for the creation of a custom interface and provides an integrated MRI simulator. Interfaces were created with the purpose of providing neurosurgeons easy and intuitive access to MRI viewpoints that are already commonly used in a stereotactic operating room setting. For this work, these viewpoints included standard axial, sagittal, and coronal views, as well as two views in the plane of an invasive deice, and one perpendicular to the device, termed ‘probe’s eye view’. The standard views are meant to quickly show the clot in relation to well understood brain viewpoints. The oblique planes co-linear with the device are designed to show clot lysing drugs relative to the catheter. The probe’s eye view mimics a standard view used commonly in neurosurgery.With the help of RTHawk’s pre-existing libraries of widgets and pulse sequences, two types of visual interfaces are demonstrated:
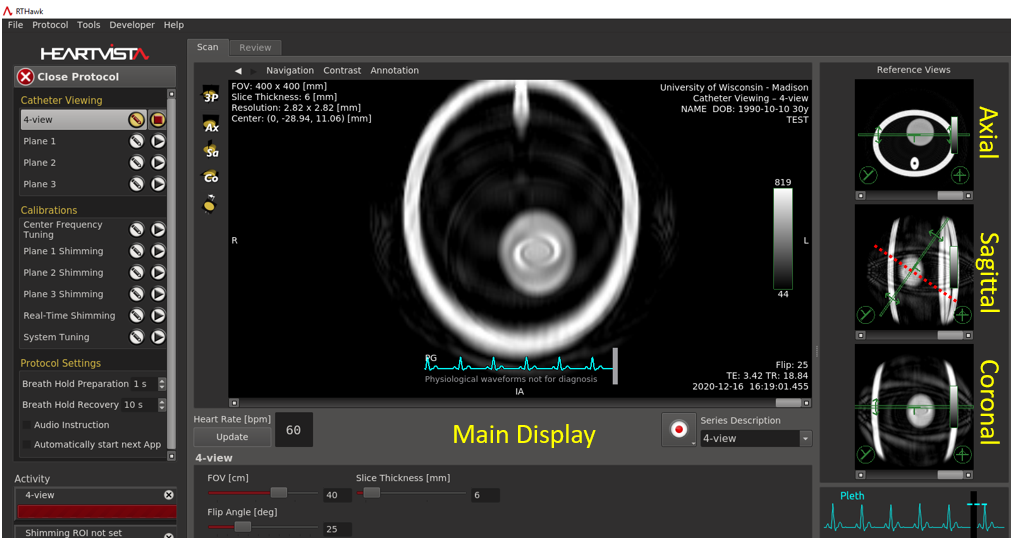
1) A 4-panel display, where three panels are the reference axial, sagittal, and coronal views, with the fourth main window allowing for the real-time display of any through plane selectable by the user from the reference planes. A real-time spiral GRE sequence is used, where FOV, slice thickness, and flip angle are allowed to be changed in real-time. Interface is shown in Fig. 3.
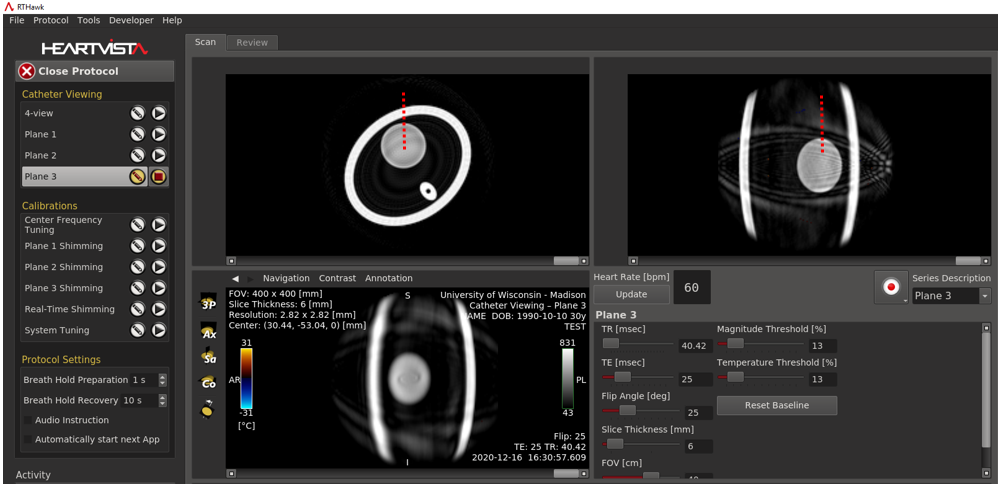
2) A 3-panel display, where each of the three panels are fully adjustable by the user. This includes selecting any through-plane to visualize, rotating the image, and selecting parameters in real-time such as TR, TE, and FOV. A real-time spiral GRE sequence is used as shown in Fig 4. The TE can easily be extended to provide T2* imaging that highlights clot.
Due to time constraints and difficulties related to COVID-19 MRI, the prototype results are all from a simulated phantom.
Results
Both interfaces were easy to prototype and intuitive to use. Data is acquired in real-time until the user stops acquisition. Viewing any plane during the real-time sequence is possible and nearly-instantaneous due to the rapid GRE sequences used. As an example, Fig. 3 shows a trajectory of an invasive device on the sagittal plane shown in red. By using a through-plane tool on the sagittal reference window, a plane perpendicular to the trajectory is chosen, and is represented on the main view as an example probe’s eye view. This view will constantly update and can be changed at any time. Figure 4 shows that two views perpendicular to the device’s path can be easily displayed (top), all while still displaying the probe’s eye view (bottom). Furthermore, parameters can be chosen in real-time for flexibility.Discussion
MR-guidance holds many advantages over CT in regards to ICH visualization and evacuation. The flexibility provided by the RTHawk interface allow for rapid prototyping and feedback from our neurosurgery collaborators. Due to MR-magnet constraints over the past couple months, integrating on an actual 3T GE scanner has not been completed yet. After integration, we plan to first test the real-time visualization system in ex-vivo models of swine blood and then move to a swine model of ICH using injected blood to simulate an ICH. Further development on the prototype platform is planned to create six concurrent visualization planes, similar to the Medtronic Stealth setup our neurosurgery collaborators use when guiding devices in the stereotactic OR.Conclusion
The MR-guidance prototype created using RTHawk shows potential to be a flexible and reliable tool to assist as monitoring and guiding tools and lysing drugs during clot-evacuation procedures, potentially for more extensive clot evacuation while minimizing chances of rebleeds.Acknowledgements
We acknowledge funding support from NIH 1R43NS110164-01A. UW-Madison also receives research support from GE Healthcare. I would also like to thank Eugene Ozhinsky for his help when I was starting out.References
[1] Hanley DF, Thompson RE, Rosenblum M, Yenokyan G, Lane K, McBee N, Mayo SW, Bistran-Hall AJ, Gandhi D, Mould WA, Ullman N, Ali H, Carhuapoma JR, Kase CS, Lees KR, Dawson J, Wilson A, Betz JF, Sugar EA, Hao Y, Avadhani R, Caron JL, Harrigan MR, Carlson AP, Bulters D, LeDoux D, Huang J, Cobb C, Gupta G, Kitagawa R, Chicoine MR, Patel H, Dodd R, Camarata PJ, Wolfe S, Stadnik A, Money PL, Mitchell P, Sarabia R, Harnof S, Barzo P, Unterberg A, Teitelbaum JS, Wang W, Anderson CS, Mendelow AD, Gregson B, Janis S, Vespa P, Ziai W, Zuccarello M, Awad IA, Investigators MI. Efficacy and safety of minimally invasive surgery with thrombolysis in intracerebral haemorrhage evacuation (MISTIE III): a randomised, controlled, open-label, blinded endpoint phase 3 trial. Lancet. 2019. Epub 2019/02/12. doi: 10.1016/S0140-6736(19)30195-3. PubMed PMID: 30739747.Melander A, Olsson J, Lindberg G, Ciaria MV, Ariano M, Strom R, Gibney J, Weiss U, Turner B, O'Gorman P, Watts G, Powrie J, Crook M, Shaw K, Cummings M. 35th Annual Meeting of the European Association for the Study of Diabetes : Brussels, Belgium, 28 September-2 October 1999. Diabetologia. 1999;42(Suppl 1):A1-A330. Epub 1999/08/01. doi: 10.1007/BF03375458. PubMed PMID: 27770183.
[2] Moskwa R, Olsen M, et al. Feasibility and Demonstration of Controlled, Comprehensive Delivery of Clot-Busting Drugs for MR Image-Guided Intracerebral Clot Evacuation. Poster session presented at: ISMRM. 27th Annual Conference. 2019 May 14; Montreal, Canada.
[3] Santos JM, Wright GA, Pauly JM. Flexible real-time magnetic resonance imaging framework. Conf Proc IEEE Eng Med Biol Soc. 2004;2:1048-51. PubMed PMID: 17271862.
Figures