4203
MIXTURE: A novel sequence for simultaneous morphological and quantitative imaging based on multi-interleaved 3D turbo-spin echo MRI1Philips Japan, Tokyo, Japan, 2Department of Radiology, Eastern Chiba Medical Center, Chiba, Japan, 3Philips Healthcare, Hamburg, Germany, 4Department of Diagnostic Radiology and Radiation Oncology, Graduate School of Medicine, Chiba University, Chiba, Japan, 5Philips Healthcare, Cleveland, OH, United States, 6Department of Radiology, Saitama Medical University, Saitama, Japan, 7Department of Orthopaedic Surgery, Eastern Chiba Medical Center, Chiba, Japan, 8General Medical Services, Graduate School of Medicine, Chiba University, Chiba, Japan, 9Philips Healthcare, Best, Netherlands
Synopsis
3D high-resolution magnetic resonance imaging (MRI) is clinically essential for an accurate assessment of subtle pathophysiological changes in different anatomies. However, long exam time remains a practical challenge that requires additional scans for either complementary quantitative parametric mapping or morphological information for clinical diagnosis. In this study, we introduce a novel method termed Multi-Interleaved X-prepared TSE with inTUitive RElaxometry (MIXTURE) for simultaneous morphological and quantitative imaging with volumetric isotropic resolution within one single scan and demonstrate the approach in multi-contrast quantitative knee imaging with direct T2- or T1ρ-mapping.
Introduction
3D high-resolution isotropic quantitative mapping is clinically desired to accurately assess various disease statuses. Recent techniques, such as quantitative DESS (qDESS)1 and 3D QALAS2,3, are based on rapid gradient echo (turbo field echo: TFE) readout because high-resolution volumetric images can be obtained within a clinically feasible scan time. Similarly, T2- or T1ρ-prepared multi-interleaved TFE sequences have been introduced for cardiac4,5 and MSK6,7 quantitative applications. Although 3D quantitative maps are clinically useful, source images of these sequences are not utilized for diagnosis purpose, because they do not present comparable contrast to conventional turbo spin-echo (TSE)-based images in either proton density-weighted (PDW) or T2-weighted (T2W) contrast.On the other hand, 3D TSE imaging with tissue-specific optimized contrasts is now becoming clinical routine sequence, especially for the MSK imaging8 owing to scan acceleration techniques such as Compressed SENSE9-11. We hypothesized that 3D quantitative sequences based on TSE, instead of TFE readout, could also be feasible, in which case the source images may be utilized for diagnosis providing comparable contrast to conventional 3D PDW or T2W-TSE images.
In this study, we introduced a new sequence, termed MIXTURE (Multi-Interleaved X-prepared TSE with inTUitive RElaxometry), based on 3D magnetization-prepared multi-interleaved TSE, to simultaneously obtain morphological and quantitative information in one single scan. The concept and optimization of the MIXTURE sequence was presented with initial clinical feasibility demonstrated in imaging of the knee joint in healthy volunteers and patients.
Methods
A schematic overview of the MIXTURE sequence for 3D isotropic MSK T2- or T1ρ-mapping is shown in Figure 1 and 2. Whereas the mapping mechanism is enabled by the corresponding magnetization-preparation scheme, for example, T2- or spinlock (SL)-preparation, the individual preparation times are applied alternatively before each TSE shot. A segmented 3D TSE with variable refocusing flip angles was employed similar to a conventional MSK 3D TSE scan. Furthermore, inversion recovery (IR) pulse and/or spectral-selective IR pulse (SPAIR) are the optional and can be freely applied for respective shots independently, resulting in generating different image types like a combination of PDW and fat-suppressed (FS) T2W, or vice versa in a single scan. Last but not least, the Compressed SENSE technique that employed compressed sensing with coil sensitivity information9 was applied for MIXTURE sequence to further shorten the total scan time.For MIXTURE T2 mapping, two images with different T2-prep times (TE = 0 and 50ms) were acquired with interleaved acquisition for generating the T2map. Furthermore, TSE shot#1 did not employ any prepulses (“PDW”) and TSE shot#2 applied both SPAIR and T2prep (“FS-T2W”) [Fig.1] to obtain morphological and pathological 3D TSE images.
For MIXTURE T1ρ mapping, the sequence has three interleaved TSE shot blocks to acquire three images with different SL preparation times (SL = 0, 25, and 50ms) with amplitude of the SL pulse of 500 Hz. Similar to the MIXTURE T2, TSE shot#1 did not apply any prepulses (PDW) and TSE shot#2&3 applied both SPAIR and SL pulses [Fig.2]. For SL preparation pulse, a twice-refocused scheme12 was applied for improving the robustness of SL pulses across the entire imaging volume.
A total of 5 volunteers and 2 patients were examined on 3.0T whole-body clinical systems (Ingenia CX/Ingenia Elition, Philips Healthcare, Best, the Netherlands). The study was approved by the local IRB, and written informed consent was obtained from all subjects.
The scan parameters were optimized for 3.0T with the main imaging parameters for MIXTURE T2: 3D PDW TSE, Coronal acquisition, voxel size=0.7mm3, FOV=150*150mm, C-SENSE reduction factor=3.0, TR/TE=1200/27ms, TSE factor=70, and total acquisition time=5:58. For MIXTURE T1ρ: 3D PDW TSE, Sagittal acquisition, voxel size=0.8mm3, FOV=145*161mm, C-SENSE reduction factor=3.5, TR/TE=1200/26ms, TSE factor=60, and total acquisition time=8:13.
Results & Discussion
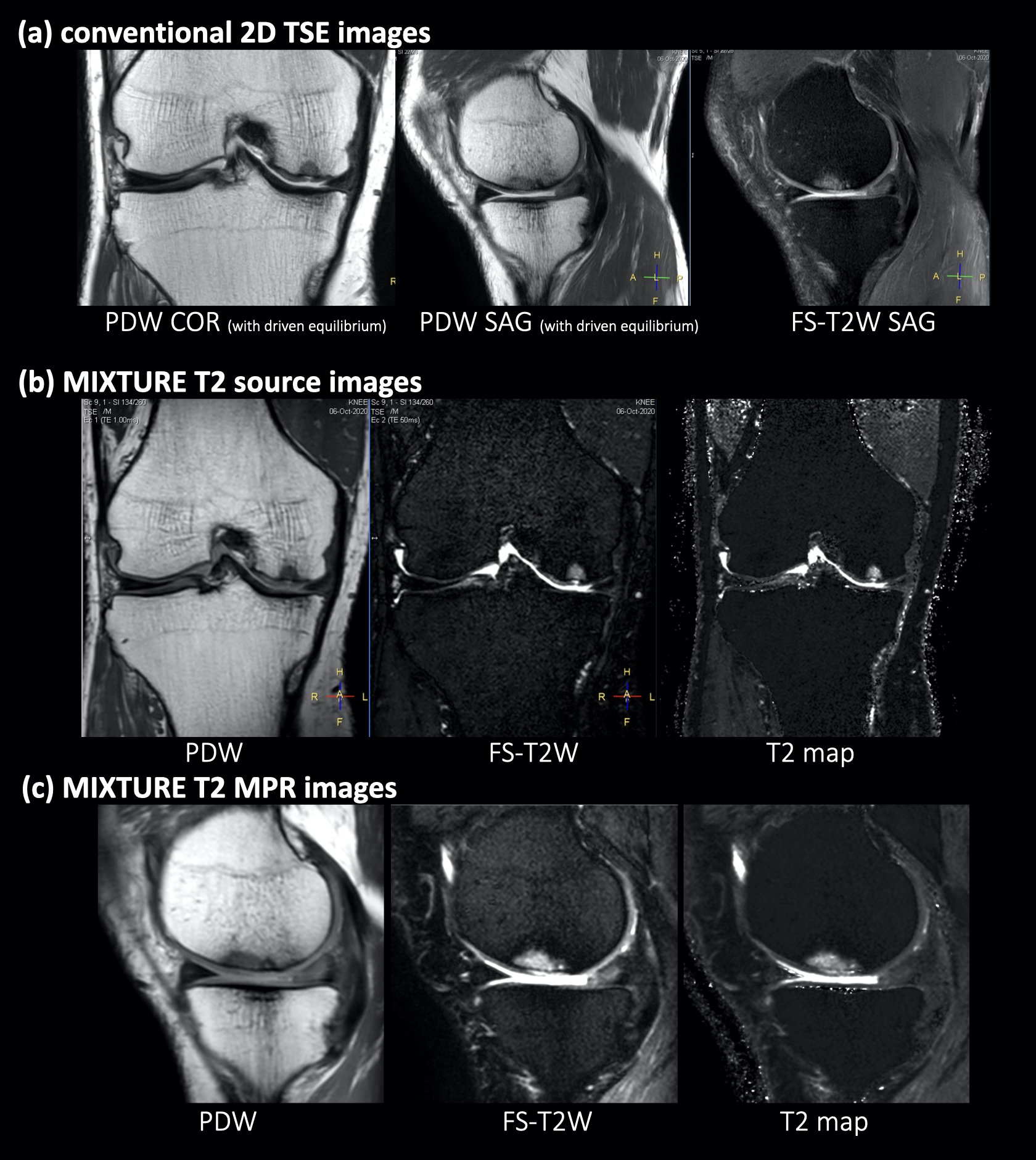
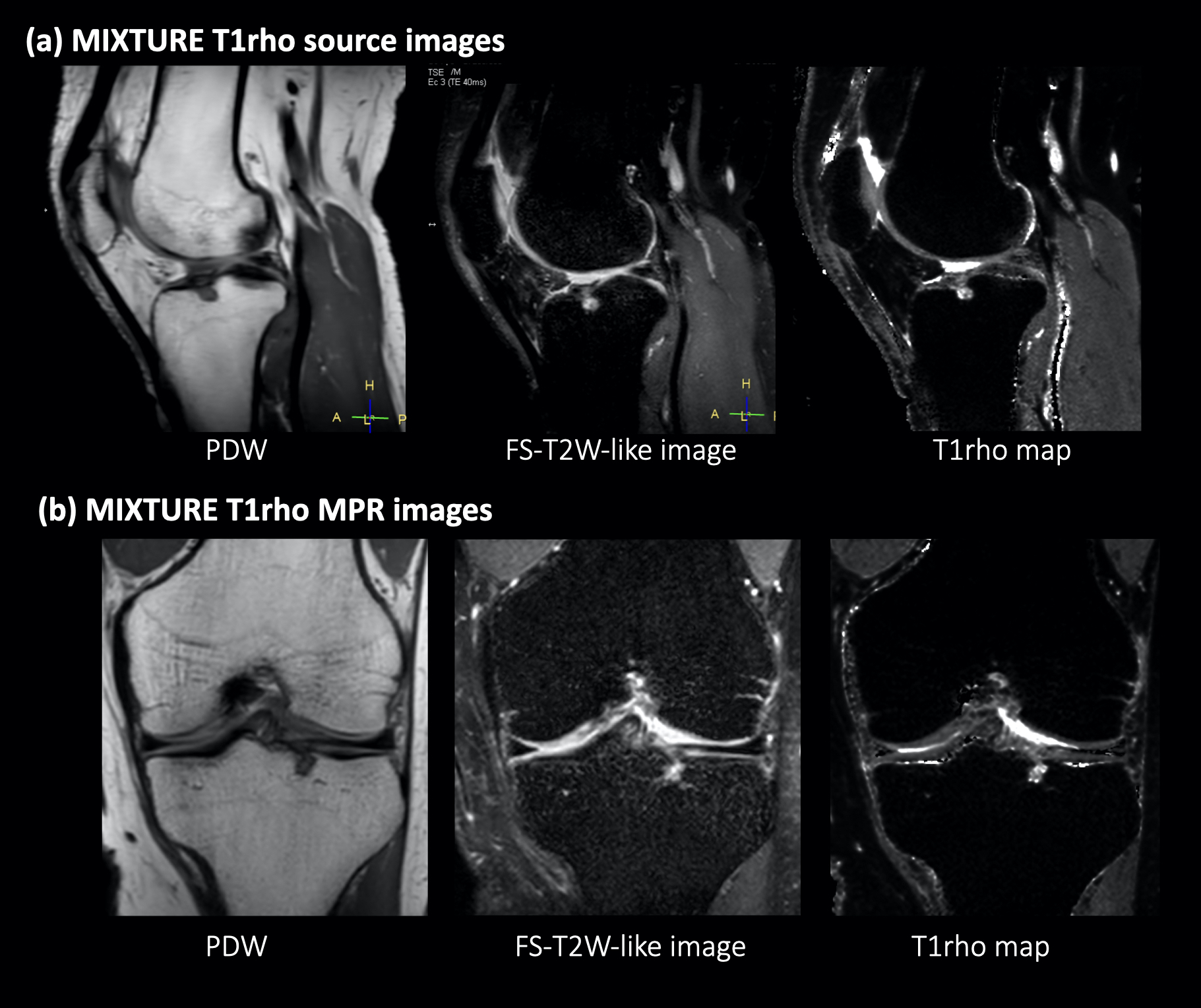
Representative conventional knee clinical routine images, source, MPR and mapping images of 3D MIXTURE T2 are shown in Figure 3. For MIXTURE, all images with a 0.7-mm isotropic spatial resolution showed good SNR with no obvious artifact in the knee. Similar morphological information to conventional PDW and FS-T2W were obtained within one single scan, from which additional quantitative T2 maps could also be generated.Figure 4 shows representative source and MPR images of PDW and T2W-like images, and T1ρ maps from the MIXTURE T1ρ datasets. T2W-like source images could be obtained by cumulating the later TSE shots (fat-suppressed) of SL prepared images.
It is noteworthy that, similar to the conventional TSE scan, MIXTURE PDW provided typical information about the anatomy, while MIXTURE T2W, whether FS or not, provided information more sensitive to potential pathological changes, which was further compensated by quantitative information from the obtained parametric maps.
Conclusion
We demonstrated the feasibility of a new multi-interleaved 3D quantitative TSE sequence with volumetric isotropic high-resolution and quantitative T2/T1ρ mapping functionality within one single scan. Clinical examples in the knee joints were presented that were achieved within a clinically reasonable scan time. While it may be helpful for both qualitative and quantitative assessment in patients with various diseases, further systematic investigations are needed to study its clinical robustness and precision in comparison to the conventional techniques.Acknowledgements
No acknowledgement found.References
1. Lu Q, et al. Application of Compressed Sensing to Quantitative Double Echo steady state (qDESS) for Rapid T2 Relaxometry in Knees. Proc. ISMRM 2020:2733.
2. Kvernby S, et al. Simultaneous three-dimensional myocardial T1 and T2 mapping in one breath hold with 3D-QALAS. J Cardiovasc Magn Reson. 2014 Dec 20;16(1):102.
3. Fujita S, et al. Three-dimensional high-resolution simultaneous quantitative mapping of the whole brain with 3D-QALAS: An accuracy and repeatability study. Magn Reson Imaging. 2019 Nov;63:235-243.
4. van Oorschot JW, et al. Single Breath-Hold T1ρ-Mapping of the Heart for Endogenous Assessment of Myocardial Fibrosis. Invest Radiol. 2016 Aug; 51(8): 505-12.
5. Yoneyama M, et al. Rapid free-breathing 3D isotropic whole-heart diastolic and systolic myocardial T2mapping. Proc. ISMRM 2020:2061.
6. Nagawa K, et al. Rapid 3D sub-millimeter isotropic T1ρ mapping of the knee using motion-robust interleaved spin-lock acquisition with compressed sensing. Proc. ISMRM 2020:2690.
7. Nagawa K, et al. Accelerated high-resolution (0.5mm2) T1ρ mapping of the knee joint using interleaved spin-lock-prepared 3D gradient echo with Compressed SENSE. Proc. ISMRM 2020:3808.
8. Glaser C, et al. Understanding 3D TSE Sequences: Advantages, Disadvantages, and Application in MSK Imaging. Semin Musculoskelet Radiol. 2015 Sep;19(4):321-7.
9. Geerts-Ossevoort L, et al. Compressed SENSE Speed done right. Every time. The Netherlands: Philips Healthcare; 2018 Jan. Report No: 4522 991 31821. https://www.philips.de/content/dam/b2bhc/de/resourcecatalog/landingpages/ingeniaelition/White_Paper_Compressed_SENSE-opt.pdf
10. Mönch S, et al. Magnetic Resonance Imaging of the Brain Using Compressed Sensing - Quality Assessment in Daily Clinical Routine. Clin Neuroradiol. 2020 Jun;30(2):279-286.
11. Bratke G, et al. Accelerated MRI of the Lumbar Spine Using Compressed Sensing: Quality and Efficiency. J Magn Reson Imaging 2019 Jun;49(7):e164-e175. 12. Pang Y. A self-compensated spin-locking scheme for quantitative R1ρ dispersion in articular cartilage. Proc. ISMRM 2020:2736.
Figures
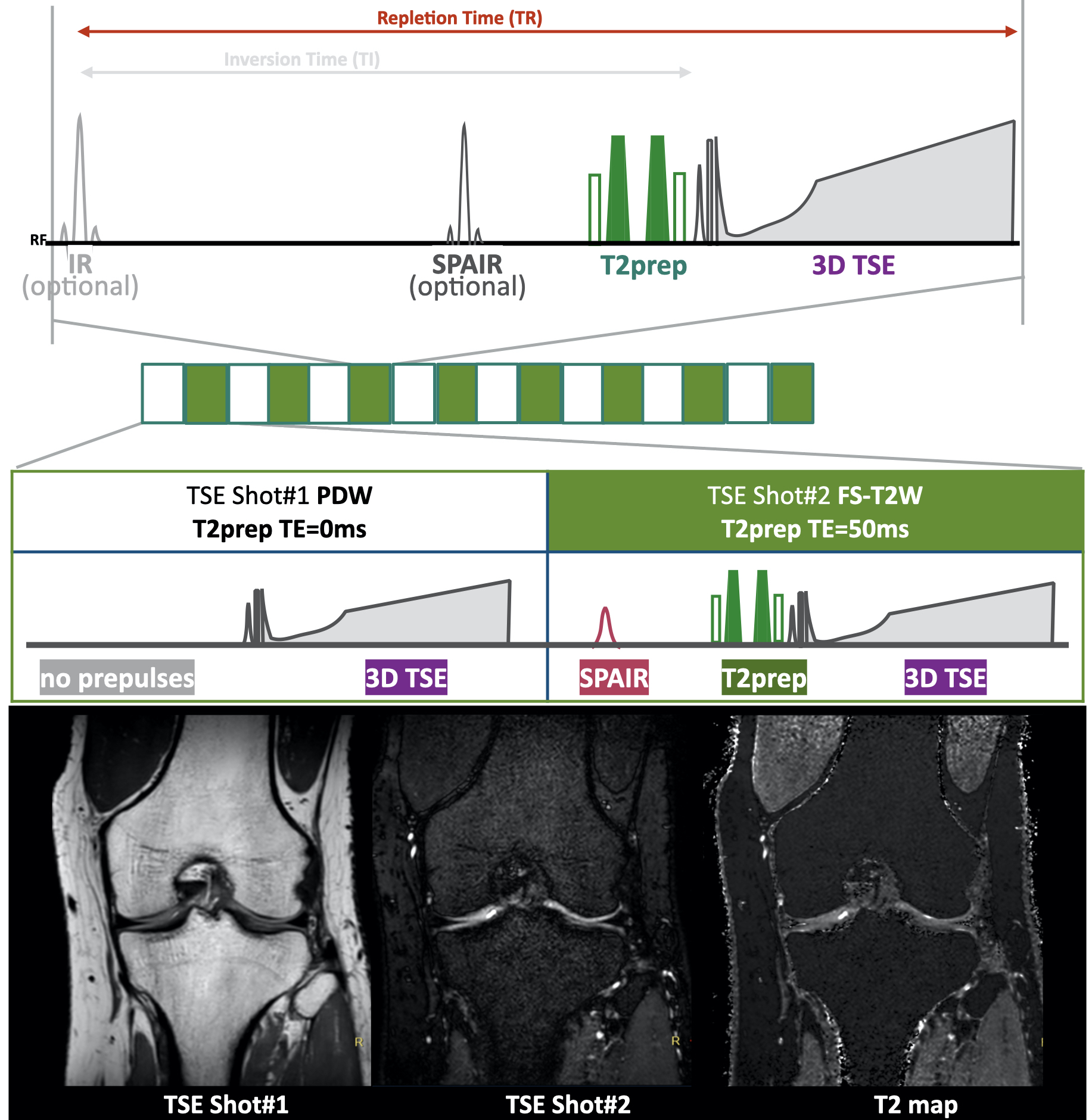
Figure 1. Scheme of the MIXTURE T2 mapping.
T2-mapping is performed using T2-prepared 3D segmented turbo spin- echo (TSE) with variable refocusing pulse trains. Two images with different TE (TE = 0 and 50ms) were acquired with interleaved acquisition. To obtain the compatible contrasts with routine TSE images, TSE shot#1 did not apply any pre-pulses (as “PDW) and shot#2 applied both SPAIR and T2prep (as “fat-suppressed T2W”).
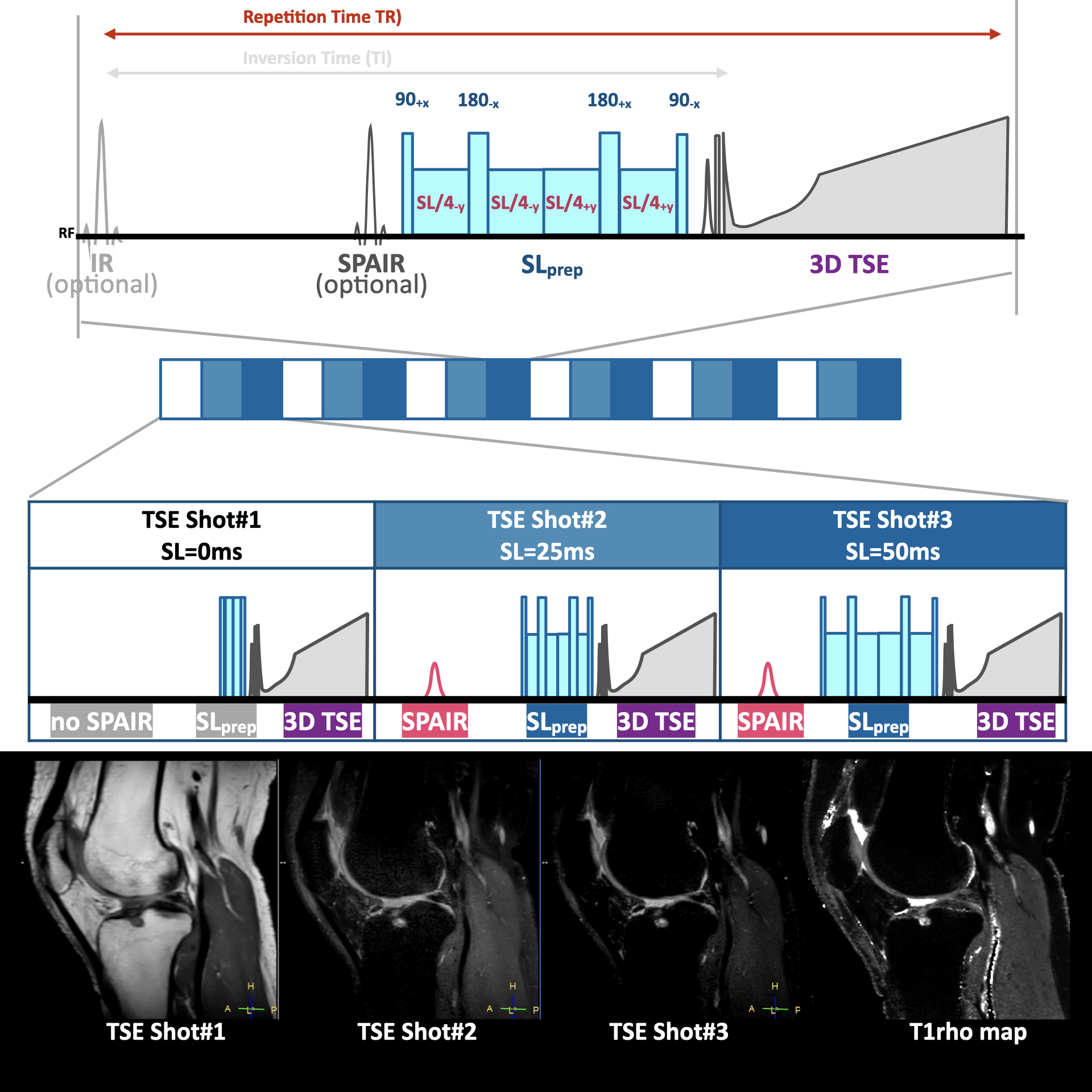
Figure 2. Scheme of the MIXTURE T1ρ mapping.
T1ρ mapping was performed using a twice-refocused spin-lock (SL) prepared segmented TSE sequence with spectral fat suppression. Three images with different SL preparation times (SL = 0, 25, and 50ms) were acquired with interleaved acquisition. Amplitude of the SL pulse was set to 500 Hz. TSE shot#1 did not apply any pre-pulses and later shots applied both SPAIR and SLprep.