4193
Three-dimensional reduced field-of-view imaging (3D-rFOVI)1Center for MR Research, University of Illinois at Chicago, Chicago, IL, United States, 2Department of Bioengineering, University of Illinois at Chicago, Chicago, IL, United States, 3Departments of Radiology and Neurosurgery, University of Illinois at Chicago, Chicago, IL, United States
Synopsis
Reduced field-of-view (rFOV) imaging has been achieved in 2D imaging. Although 2D rFOV can reduce image distortion and produce high in-plane resolution in EPI, the through-plane resolution remains poor and signal voids persist. We report a 3D reduced field-of-view imaging (3D-rFOVI) sequence to extend the conventional 2D rFOV imaging to 3D by using a slab-selection 2D RF pulse in conjunction with through-slab phase-encoding. This sequence features high isotropic spatial resolution in EPI images while reducing off-resonance effects that cause image distortion and signal voids. We have successfully applied the 3D-rFOVI technique to fMRI and DWI.
Introduction:
Echo planar imaging (EPI) has been widely used in functional magnetic resonance imaging (fMRI) and diffusion-weighted imaging (DWI) due to its fast acquisition speed. It, however, suffers from image distortion, signal void, and low spatial resolution. To mitigate these problems, reduced field-of-view (rFOV) imaging based on a 2D RF excitation pulse has been employed to limit the spatial coverage along the phase-encoding direction within a selected slice1-4. In doing so, a wider effective bandwidth along the phase-encoding direction can be achieved to reduce in-plane image distortion while achieving a high in-plane spatial resolution5. However, the through-plane resolution remains poor, making it unsuitable for application requiring isotropic high spatial resolution and subject to signal voids caused by intravoxel dephasing. The goal of this work is to address the problems by developing a three-dimensional reduced field-of-view imaging (3D-rFOVI) sequence based on a slab-selective 2D RF pulse, followed by phase-encoding along the slab direction.Methods:
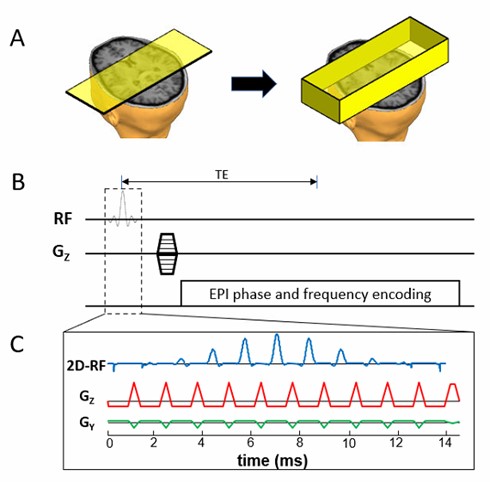
3D-rFOVI: Unlike conventional 2D rFOV imaging, 3D-rFOVI uses a 2D RF pulse to excite a reduced-FOV slab (Figure 1A). The slab is phase-encoded to produce a 3D zoomed image. This approach can result in high isotropic spatial resolution and signal-to-noise ratio (SNR) while reducing off-resonance effects that cause image distortion and signal void.2D RF pulse design: A slab-selective 2D RF pulse (Figure 1C) was designed by employing a fly-back EPI-like excitation k-space trajectory6. Discrete sampling of excitation k-space along the blipped direction resulted in periodic replicates of the excitation profile. Only the main band was used to excite a limited region, while the sidebands were positioned outside the imaged object4. Eleven sub-pulses each with a time-bandwidth product (TBP) of 3.01 were modulated by an envelope pulse (TBP = 3.53 and pulse-width = 14.7ms; Figure 1C). The slab-selective 2D RF pulse was implemented in T2*-weighted GRE-EPI and diffusion-weighted SE-EPI pulse sequences, the latter of which contained a slab-selective 180° refocus pulse. Fat suppression was achieved by using a frequency-selective saturation pulse preceding the 2D RF pulse.
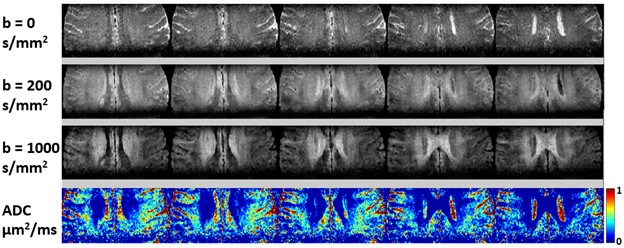
Experiments and data processing: Three experiments were conducted on a GE MR750 3T scanner. In the first experiment, the 3D-rFOVI technique was validated on an ACR phantom. 3D-rFOV images from GRE-EPI were acquired with the following parameters: volume TR/TE = 2000/30 ms, flip angle = 30°,FOV = 240x120 mm2, slab thickness = 38 mm, acquisition matrix = 128x64x20, and spatial resolution = 1.9x1.9x1.9 mm3. For comparison, images were also acquired using 3D GRE-EPI with a full FOV of 240x240 mm2 and a matrix of 128x128. In the second experiment, 3D fMRI was performed on healthy human subjects using a 32-channel head coil with a visual stimulation paradigm (dark-gray and light-gray checkboard flashing at 8 Hz in a block design). The paradigm contained six 48 s blocks with 24 s rest followed by 24 s stimulus, and the total acquisition time for both task and resting scans was about 5 min. Image acquisition was performed using the 3D-rFOVI GRE-EPI sequence with the same parameters as in the ACR phantom experiment except for FOV = 200x100 mm2, slab thickness = 40 mm, and spatial resolution = 2x2x2 mm3. All data were analyzed using SPM8 on MATLAB 2012b. Data preprocessing included image realignment and spatial smoothing with a 6-mm full-width-at-half-maximum Gaussian kernel. A general linear model was applied for visual activation detection with a threshold of P < 0.05 (FWE corrected) and spatial cluster size of at least 30 pixels. In the third experiment, 3D zoomed diffusion-weighted brain images were acquired from healthy volunteers using a SE-EPI 3D-rFOVI sequence with an 8-channel head coil. The key parameters were: TR/TE = 4000/75 ms, FOV = 140x70 mm2, slab thickness = 40 mm, spatial resolution = 1x1x1 mm3, diffusion direction = A/P, b = 0, 200, and 1000 s/mm2, and scan time = 8 mins. ADC maps were obtained from images acquired at all three b-values using a mono-exponential model.
Results:
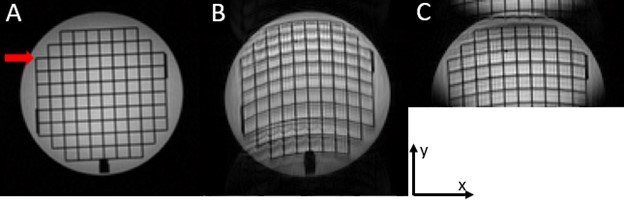
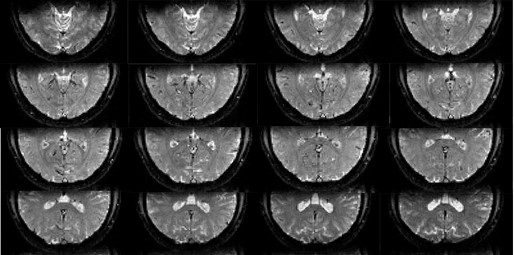
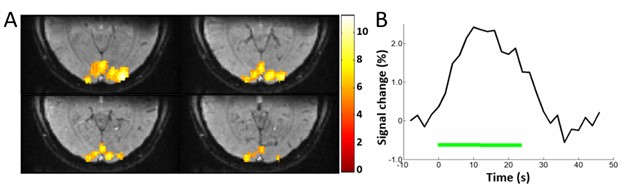
The ACR phantom images acquired with three sequences are shown in Figure 2. Compared to the reference 3D GRE image in Figure 2A, the image with full FOV (Figure 2B) exhibited excessive distortion. Using 3D-rFOVI with GRE-EPI, image distortion was substantially reduced as shown in Figure 2C. A set of rFOV 3D images from the second experiment are displayed in Figure 3 where virtually no geometric distortion was observed in the visual cortex with an isotropic resolution of 2x2x2 mm3. Figure 4 illustrates four contiguous visual fMRI activation maps selected from the 3D volume, together with the averaged time course. Figure 5 shows the results from the third experiment. With 3D-rFOVI using SE-EPI, three-dimensional diffusion-weighted images with isotropic high spatial resolution (1x1x1 mm3) was achieved on the human brain without appreciable image distortion.Discussion and conclusion:
In this study, we have extended the conventional 2D reduced-FOV imaging to 3D by using a slab-selection 2D RF pulse in conjunction with through-slab phase-encoding. This approach allowed us to achieve isotropic high spatial resolution in EPI within relatively short scan times and substantially reduce image distortion. The 3D-rFOVI technique has been successfully demonstrated in 3D fMRI and 3D DWI of the human brain over a zoomed volume, and is expected to find other applications.Acknowledgements
This work was supported in part by the National Institutes of Health (5R01EB026716-01 and 1S10RR028898-01). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.References
1. Alley MT, Pauly JM, Sommer FG, et al. Angiographic imaging with 2D RF pulses. Magn Reson Med. 1997.
2. Saritas EU, Cunningham CH, Lee JH, et al. DWI of the spinal cord with reduced FOV single-shot EPI. Magn Reson Med. 2008.
3. Finsterbusch J. Functional neuroimaging of inner fields-of-view with 2D-selective RF excitations. Magn Reson Imaging. 2013.
4. Zhou XJ, Sui Y, Image Domain Segmented Echo Planar Magnetic Resonance Imaging Using a 2D Excitation Radiofrequency Pulse. US Patent No. 9797970. April 13, 2016.
5. Zhong Z, Merkitch D, Karaman MM, et al. High-spatial-resolution diffusion MRI in Parkinson disease: Lateral asymmetry of the substantia nigra. Radiology. 2019.
6. Finsterbusch J. Fast-spin-echo imaging of inner fields-of-view with 2D-selective RF excitations. J Magn Reson Imaging. 2010.
Figures