4158
Comparisons of high-resolution intracranial vessel wall MRI findings in different types of middle cerebral artery territory infarction1Radiology, Severance Hospital, Seoul, Korea, Republic of, 2Neurology, Severance Hospital, Seoul, Korea, Republic of
Synopsis
Our object is the evaluation of spatial relationship of MCA plaque and perforator in different types of MCA infarction using VW-MRI. We included 34 patients with acute MCA infarction and divided into 3 groups according to infarction pattern. We evaluated location relationship between perforators and plaques. Wall area, stenosis degree and plaque enhancement were calculated. There was difference in relationship between plaque and perforator, location and characteristics of plaque in different types of MCA infarction. In patients with BOD, the plaque margin was closer to perforator orifice with less stenosis and enhancement than patients with artery to artery embolism.
Introduction
Intracranial atherosclerotic stroke (ICAS) is one of the major cause of stroke, especially in Asian population1. ICAS is caused by various mechanism and is mainly caused by artery-to-artery embolism or branch occlusive disease (BOD)2. BOD is one of types of ICAS that is caused by atherosclerotic plaque blocking orifice of perforating artery, which is different from ICAS caused by artery-to-artery embolism3. Previous studies showed BOD group had more frequently the plaques in the superior or upper dorsal side of the MCA4-8. However, these studies4-8 only qualitatively evaluated plaque distribution of MCA in BOD and did not consider location of the perforator of MCA. The purpose of our study is the evaluation of the spatial relationship of MCA plaque and perforating artery in different types of middle cerebral artery territory infarction using VW-MRI.Method
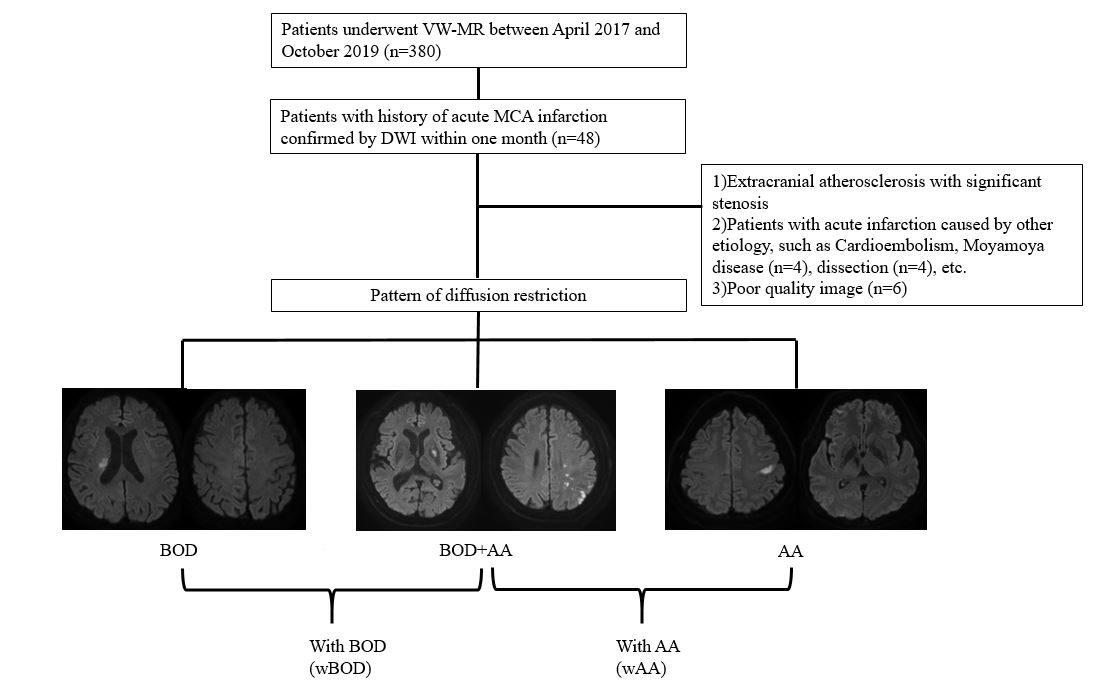
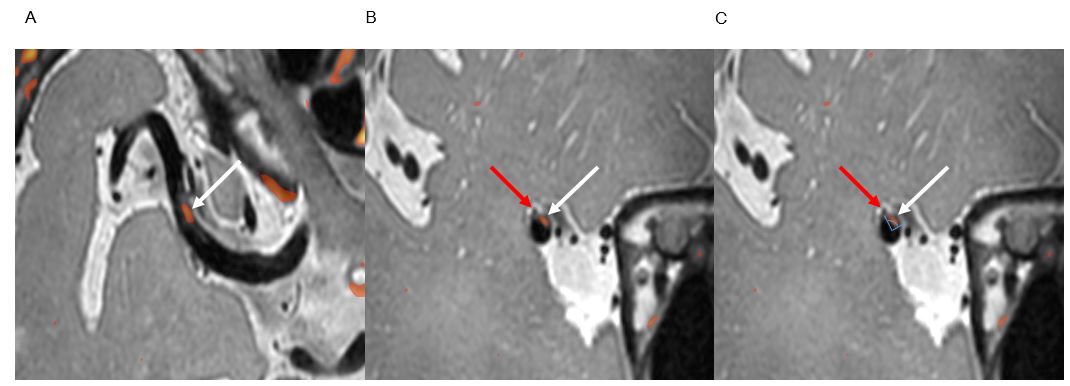
There are 380 patients who underwent 3.0 T-vessel wall MRI between April 2017 and October 2019 in our institution. We included patients with history of acute MCA infarction confirmed by DWI within one month (n=48). Total 34 patients were divided into 3 groups according to the pattern of infarction (figure 1): (1) BOD group (2) BOD+AA (BOD with artery to artery embolism) group (3) AA group. For subgroup analysis, BOD group and BOD+AA group were combined as one group (with BOD group [wBOD]) and compared with AA group. BOD+AA group and AA group were combined as one group (with AA group [wAA]). To evaluate location relationship between the perforators and the plaques, we chose the cross-sectional image perpendicular to MCA course in which perforator arising. Location of the perforator and plaque were evaluated qualitatively. Location of the perforator arising from M1 portion of the MCA and the distribution of the plaque were also quantitatively as the angle (0 º: ventral, 90 º: superior, 180 º: dorsal, 270 º: inferior) (figure 2). In order to evaluate how close orifice of the perforator and margin of plaque are, the angular difference between orifice of the perforator and margin of plaque was calculated. The outer wall and the lumen were manually drawn in cross-sectional images on T1 and PD images at the three location: (1) perforators origin, (2) most stenotic portion of MCA, (3) reference normal vessel (contralateral or proximal to the stenotic portion). Wall area, degree of stenosis and 95% enhancement of enhancing plaque were calculated. All features were compared between groups.Result
Patients with BOD (BOD and wBOD group) were closer to the plaque margin and perforator orifice than AA group (p=0.033, 0.011, respectively. The perforators mainly arouse at dorsal (47.1%) and superior sections (44.1%) without difference of location between groups. The location of the plaque at cross-section which perforator arouse was significantly different between groups (p=0.002). In BOD group, the plaques were mainly located in dorsal (41.2%) and superior (41.2%) sections where the perforators mainly arouse. All of patients in AA groups did not have plaque or do not overlap plaque and perforator at the cross-section where the perforator arouses. The perforator associated with culprit plaque was most frequently located in middle two third of M1 segment. BOD group had less stenosis than wAA group (p=0.003) and less enhancement than AA or wAA group did (p=0.03, 0.023, respectively).Discussion
Plaque rupture is more prone to occur at the shoulder of the carotid plaque9-12. Considering margin of plaque is more prone to rupture, we assumed that the distance between margin of the plaque and orifice of perforating artery may be closer in BOD group and BOD+AA group, perforating artery was blocked, than in AA group. Indeed, our results showed wBOD group had higher portion of patients whose orifice of perforator and margin of the plaque were close than AA group did, thereby supporting the above explanation. In our study, orifices of perforating arteries were mainly located in dorsal and superior surface of MCA, regardless of groups. These results is consistent with the results of previous 13,14. Previous studies showed superior wall plaque located near orifice of perforating artery cause symptomatic better by blocking orifice of perforator 8,15, and many patients with BOD had plaque in upper dorsal side 7. In our results, majority of patients in BOD group had plaque located in superior or dorsal wall where the perforators mainly arouse. BOD group was less stenosis than wAA group, which is consistent with previous5,16. Enhancement degree of the plaque was higher in wAA group and AA group than in BOD group and wBOD, respectively. The results is consistent with previous study5,17.Conclusion
There was difference in relationship between plaque and perforator, location and characteristic of plaque in VW-MRI in different types of middle cerebral artery territory infarction. In patients with BOD, the plaque margin was closer to perforator orifice with less stenosis and enhancement than patients with artery to artery embolism.Acknowledgements
NoneReferences
1. Gorelick PB, Wong KS, Bae H-J, Pandey DK. Large artery intracranial occlusive disease: a large worldwide burden but a relatively neglected frontier. Stroke 2008;39:2396-2399.
2. Shin DH, Lee PH, Bang OY. Mechanisms of recurrence in subtypes of ischemic stroke: a hospital-based follow-up study. Archives of neurology 2005;62:1232-1237.
3. Caplan LR. Intracranial branch atheromatous disease: a neglected, understudied, and underused concept. Neurology 1989;39:1246-1246.
4. Kim BJ, Yoon Y, Lee D-H, Kang D-W, Kwon SU, Kim JS. The shape of middle cerebral artery and plaque location: high-resolution MRI finding. International journal of stroke 2015;10:856-860.
5. Ryoo S, Lee MJ, Cha J, Jeon P, Bang OY. Differential vascular pathophysiologic types of intracranial atherosclerotic stroke: a high-resolution wall magnetic resonance imaging study. Stroke 2015;46:2815-2821.
6. Ryoo S, Park J, Kim S, Kim G-M, Chung C-S, Lee K, et al. Branch occlusive disease: clinical and magnetic resonance angiography findings. Neurology 2012;78:888-896.
7. Sun L-L, Li Z-H, Tang W-X, Liu L, Chang F-Y, Zhang X-B, et al. High resolution magnetic resonance imaging in pathogenesis diagnosis of single lenticulostriate infarction with nonstenotic middle cerebral artery, a retrospective study. BMC neurology 2018;18:1-7.
8. Xu W-H, Li M-L, Gao S, Ni J, Zhou L-X, Yao M, et al. Plaque distribution of stenotic middle cerebral artery and its clinical relevance. Stroke 2011;42:2957-2959.
9. Richardson PD, Davies M, Born G. Influence of plaque configuration and stress distribution on fissuring of coronary atherosclerotic plaques. The Lancet 1989;334:941-944.
10. Shindo S, Fujii K, Shirakawa M, Uchida K, Enomoto Y, Iwama T, et al. Morphologic features of carotid plaque rupture assessed by optical coherence tomography. American Journal of Neuroradiology 2015;36:2140-2146.
11. Thrysøe SA, Oikawa M, Yuan C, Eldrup N, Klærke A, Paaske WP, et al. Longitudinal distribution of mechanical stresses in carotid plaques of symptomatic patients. Stroke 2010;41:1041-1043.
12. Toutouzas K, Karanasos A, Tsiamis E, Riga M, Drakopoulou M, Synetos A, et al. New insights by optical coherence tomography into the differences and similarities of culprit ruptured plaque morphology in non–ST-elevation myocardial infarction and ST-elevation myocardial infarction. American heart journal 2011;161:1192-1199.
13. Marinkovic S, Milisavljevic M, Kovacevic M, Stevic Z. Perforating branches of the middle cerebral artery. Microanatomy and clinical significance of their intracerebral segments. Stroke 1985;16:1022-1029.
14. Umansky F, Gomes FB, Dujovny M, Diaz FG, Ausman JI, Mirchandani HG, et al. The perforating branches of the middle cerebral artery: a microanatomical study. Journal of neurosurgery 1985;62:261-268.
15. Yoon Y, Lee DH, Kang D-W, Kwon SU, Kim JS. Single subcortical infarction and atherosclerotic plaques in the middle cerebral artery: high-resolution magnetic resonance imaging findings. Stroke 2013;44:2462-2467.
16. Zhao Z-N, Li X-L, Liu J-Z, Jiang Z-M, Wang A-H. Features of branch occlusive disease-type intracranial atherosclerotic stroke in young patients. BMC neurology 2018;18:87.
17. Kim J-M, Jung K-H, Sohn C-H, Moon J, Han MH, Roh J-K. Middle cerebral artery plaque and prediction of the infarction pattern. Archives of neurology 2012;69:1470-1475.
Figures