4153
Ultrahigh Resolution 3T Clinical Black-blood Angiography: A new imaging biomarker of aneurysm occlusion following endovascular therapy
Adam E. Goldman-Yassen1, Eytan Raz2, Anna Derman2, Ahrya Derakhshani3, and Seena Dehkharghani2,4
1Department of Radiology, Children's Healthcare of Atlanta, Atlanta, GA, United States, 2Department of Radiology, New York University Langone Medical Center, New York, NY, United States, 3Department of Radiology, UCLA Health, Los Angeles, CA, United States, 4Department of Neurology, New York University Langone Medical Center, New York, NY, United States
1Department of Radiology, Children's Healthcare of Atlanta, Atlanta, GA, United States, 2Department of Radiology, New York University Langone Medical Center, New York, NY, United States, 3Department of Radiology, UCLA Health, Los Angeles, CA, United States, 4Department of Neurology, New York University Langone Medical Center, New York, NY, United States
Synopsis
High-resolution black-blood vessel wall imaging optimized with robust flow suppression offers reproducible, reliable, and non-invasive longitudinal evaluation of flow diversion treated aneurysms, with superior overall classification accuracy relative to conventional TOF or dynamic MRA. Aneurysm and parent vessel enhancement may persist even after angiographic occlusion during the healing phase of obliterated aneurysm.
Introduction:
High-resolution vessel wall MRI (VWI) is increasingly used to characterize intramural disorders of the intracranial vasculature unseen by conventional luminal arteriography.1 Time-of-flight MRA (TOF-MRA) and CTA are of limited utility for longitudinal evaluation of aneurysms treated with flow diversion (FD) due to signal corruption by the metallic construct traversing the parent vessel. Dynamic imaging has previously been reported for this purpose, however, commonly used gradient-echo schemes often remain vulnerable to degradation from magnetic field distortions. Routine catheter angiographic surveillance is similarly suboptimal due to requisite iodine and ionizing radiation doses and attendant risks related to peripheral and cerebrovascular catheterization. We evaluated use of state-of-the-art, black-blood VWI obtained at 400-500 micron isotropic whole brain resolution with robust flow suppression for evaluation of FD-treated aneurysms under clinically reproducible conditions, compared with standard-of-care TOF-MRA and dynamic contrast-enhanced (CE) MRA using golden-angle radial imaging with compressive sensing (GRASP).Methods:
Retrospective, IRB-approved study of 21 patients with 28 aneurysms treated by with FD (Mean 56.8 years; 21% female). All patients underwent VWI and contemporaneously obtained digital subtraction catheter angiography (DSA). Multiplanar pre- and post-gadolinium 3D, variable flip-angle T1 fast spin-echo VWI was obtained with flow suppression using delay alternating nutation for tailored excitation (DANTE) on a clinical 3T whole body scanner (PRISMAfit, Siemens Healthineers). 3D time-of-flight MRA without contrast and multiphasic, dynamic CE-MRA were also obtained. DSA was performed at 337.8 days (±254) with MRI at 361 (±259) days post FD procedure. VWI were reviewed by two subspecialty-certified neuroradiologists specializing in cerebrovascular imaging, and were evaluated subjectively for the following: in-stent stenosis, aneurysm occlusion, presence and pattern/distribution of aneurysm gadolinium enhancement, parent vessel wall changes and enhancement, and binary final determination of residual aneurysmal flow. DSA were reviewed by a neurointerventional radiologist for aneurysm occlusion and in-stent stenosis. TOF and dynamic MRA were reviewed by two different neuroradiologists for aneurysm occlusion. Inter-rater agreement was calculated using Cohen’s kappa. Sensitivity and specificity for complete aneurysm occlusion on VWI and TOF and dynamic CE-MRA were calculated relative to gold-standard DSA. Continuous variables were compared using the Mann-Whitney U test and categorical variables using Fisher’s exact test.Results:
Identification of aneurysm occlusion on VWI demonstrated a sensitivity=100%, specificity=88%, PPV=95% and NPV=100% (Table 1). Aneurysm enhancement on VWI was noted independent of angiographic occlusion, including in areas of presumed granulation/healing about the aneurysm and along the parent vessel wall at the proximal and distal landing of the endoluminal construct, however, with a trend towards lower rates of enhancement with occlusion (p=0.277). Similar trends towards lesser aneurysm enhancement were noted based upon time from initial treatment to imaging (p>0.05). Stented parent vessel wall enhancement on VWI was significantly more common when aneurysm enhancement is present (92% vs 33%, p=0.049). Sensitivity and specificity for both TOF and dynamic CE-MRA were lower than for VWI for complete aneurysm occlusion (84% and 56% and 77% and 78% for reviewer 1 and 79% and 56% and 63% and 67% for reviewer 2; Table 2 and Figure 1). High agreement was noted for TOF (kappa=0.75) and fair agreement was noted for dynamic CE-MRA (kappa=0.25).Conclusion:
High-resolution black-blood imaging optimized with robust flow suppression offers reproducible, reliable, and non-invasive longitudinal evaluation of FD-treated aneurysms, with superior overall classification accuracy relative to conventional TOF or dynamic MRA. Aneurysm and parent vessel enhancement may persist even after angiographic occlusion during the healing phase of obliterated aneurysm.Acknowledgements
No acknowledgement found.References
1. Larsen N, Fluh C, Saalfeld S, et al. Multimodal validation of focal enhancement in intracranial aneurysms as a surrogate marker for aneurysm instability. Neuroradiology 2020;62:1627-1635Figures
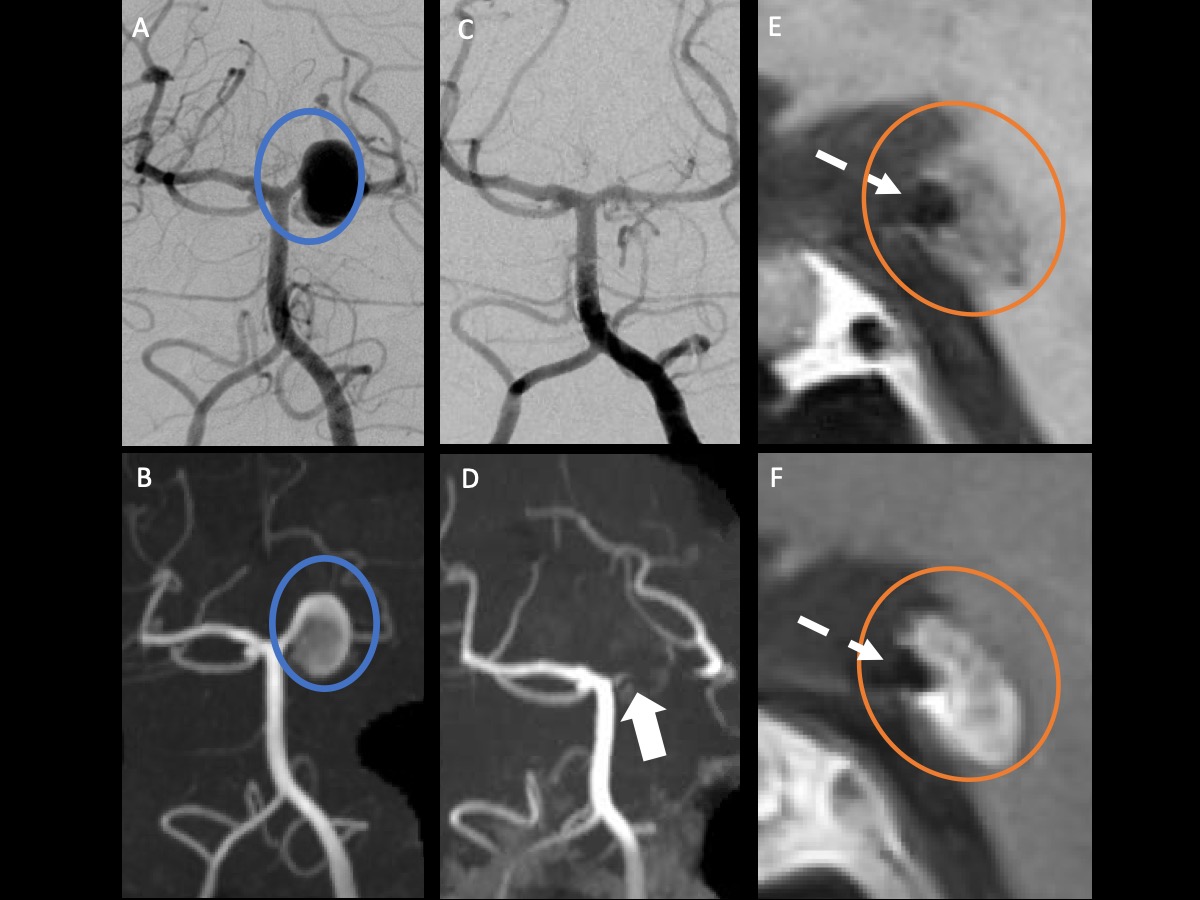
DSA (A) and TOF MRA (B) show an aneurysm at the left SCA and PCA junction (blue circle). Followup DSA (C) after basilar/left PCA flow-diverting stent placement demonstrates complete occlusion. MRA demonstrates questionable flow-related enhancement not easily discriminated from T1 shine through from organizing clot (D). Pre (E) and postcontrast (F) VWI demonstrate preserved high-resolution black blood angiography across the stented PCA segment (dashed arrow). Organizing clot within the aneurysm sac (orange circle) is noted, likely fed through a vasa vasorum, without flow voids.
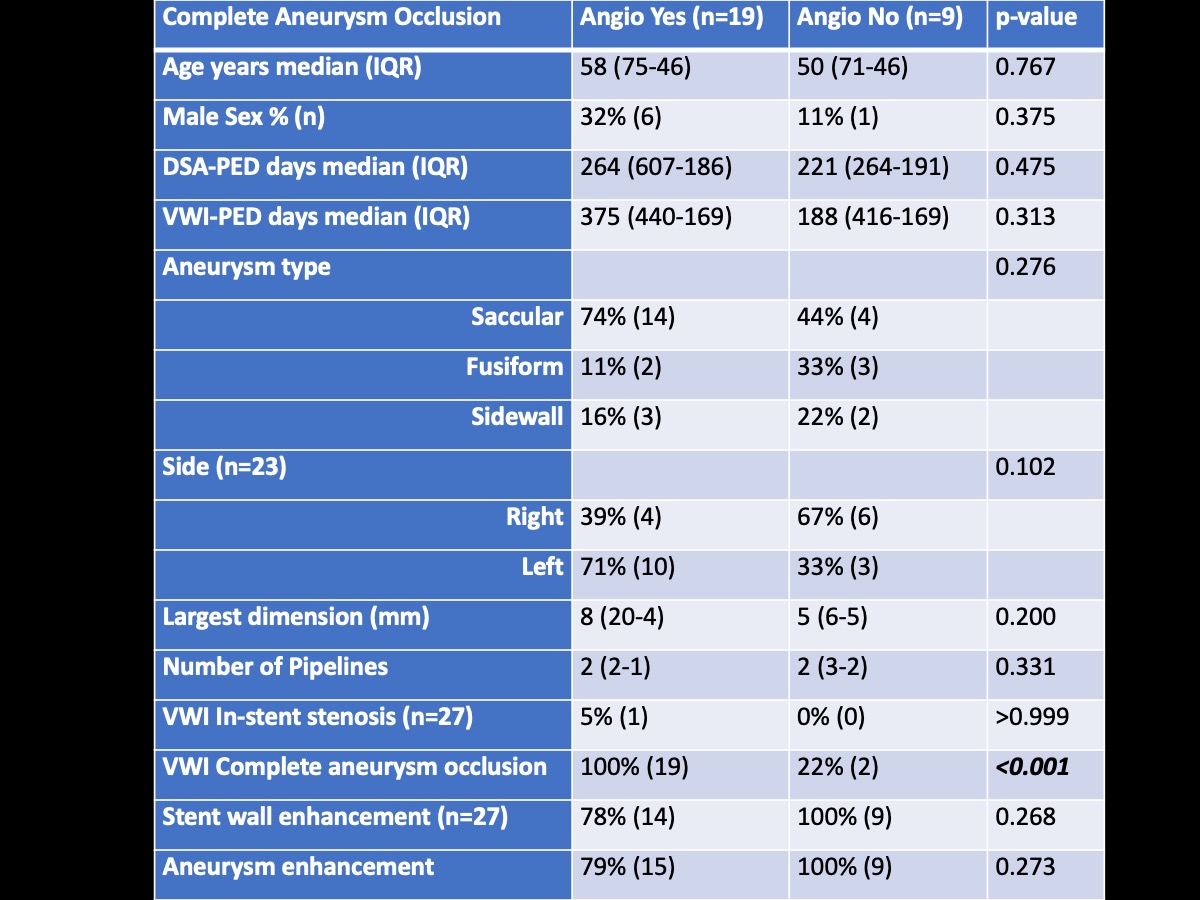
Comparison of patient characteristics and vessel wall imaging findings between subjects with and without complete aneurysm occlusion of followup angiogram after flow diverter placement.
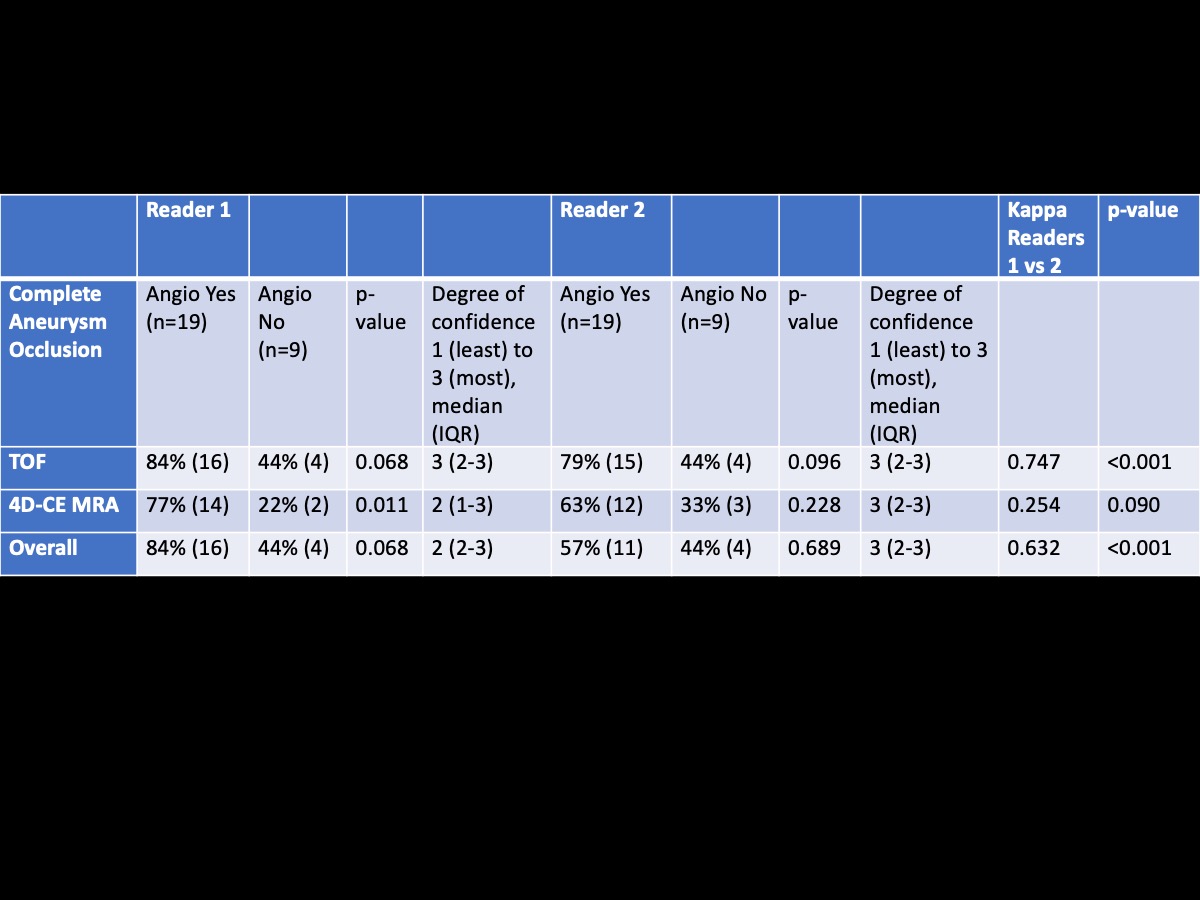
Sensitivity and specificity of time-of-flight and contrast-enhanced 4D MRA and the agreement of the two readers.