4126
Differences in acute cerebral infarction distribution patterns between young and elderly patients: a MRI study
Dandan Yang1,2, Yongjun Han3, Dongye Li4, Huiyu Qiao2, Hualu Han2, Rui Shen2, Zihan Ning2, and Xihai Zhao2
1Capital Medical University, Beijing, China, 2Tsinghua University, Beijing, China, 3Aerospace Center Hospital, Beijing, China, 4Sun Yat-Sen Memorial Hospital, Guangzhou, China
1Capital Medical University, Beijing, China, 2Tsinghua University, Beijing, China, 3Aerospace Center Hospital, Beijing, China, 4Sun Yat-Sen Memorial Hospital, Guangzhou, China
Synopsis
This study aimed to determine the distribution patterns of acute cerebral infarction (ACI) between young and elderly patients with intracranial large artery stenosis using diffusion-weighted imaging. In total, 69 young patients and 77 elderly patients were included in this study. We found that young patients had significantly higher prevalence of multiple ACI lesions in more than one vascular territory and higher percentage of lesions in both anterior and posterior circulations than elderly patients. Our findings provide new insights in optimizing the etiological diagnosis of cerebrovascular disease for young and elderly patients.
Introduction
The differences in the TOAST (Trial of Org 10172 in Acute Stroke Treatment) subtype classification and some cerebrovascular risk factors between young and elderly patients have been reported. 1,2 Previous studies indicated that the distribution patterns of acute cerebral infarction (ACI) lesions were associated with TOAST subtype classification. 3,4 We hypothesized that the ACI lesion distribution patterns may be different with age and associated with stroke etiology. However, the differences in the ACI lesion distribution patterns between young and elderly patients have not been fully investigated. Better understanding these differences will be helpful for optimizing the etiological diagnosis of ischemic stroke for young and elderly patients. This study sought to determine the differences in the distribution patterns of ACI lesions between young and elderly patients by using DWI (diffusion-weighted imaging).Methods
Study sample: One hundred and forty-six symptomatic patients (mean age, 52.1±13.4 years; 65.8% males) with intracranial large artery stenosis and ischemic stroke recruited from an observational, multicenter study of ICASMAP (NCT03417063) were retrospectively analyzed. MR imaging: All patients underwent brain MR imaging on 3.0T MR scanners (Achieva TX, Philips Healthcare, Best, The Netherlands) with 8-channel head coils. Brain MR imaging was conducted using a standard protocol including T1‐weighted (T1W), T2‐weighted (T2W), T2‐fluid‐attenuated inversion recovery (FLAIR) and DWI sequences. The imaging parameters are detailed in Fig.1. The study protocol was approved by local Ethics Committee at each participating institution and all patients provided written informed consent. Image analysis: The demographics and clinical risk factors were collected. The MR images were reviewed by two experienced neuroradiologists with consensus who were blinded to clinical information. The ACI was defined as lesions that showed hyperintensity on DWI (b = 1000 s/mm2), but hypo-intensity on corresponding apparent diffusion coefficient maps. The distribution patterns of ACI lesions on DWI were classified as single, multiple lesions in one vascular territory and multiple lesions in more than one vascular territory (Fig.2). The ACI involvement of anterior circulation and posterior circulation was also analyzed. Statistical analysis: All patients were divided into young patient group (18-50 years) and elderly patient group (51-80 years). Chi-square test and multivariate logistic regression models were performed to determine the differences in distribution patterns of ACI lesions between two groups.Results
In total, 69 young patients (mean age: 40.5 ± 8.4 years, 54 men) and 77 elderly patients (mean age: 62.4 ± 7.1 years, 42 men) were included. Young patients had significantly higher prevalence of multiple ACI lesions in more than one vascular territory (50.7% vs. 29.9%,p = 0.010)than elderly patients (Fig.3). After adjusted for confounding factors, the prevalence of multiple ACI lesions in more than one vascular territory remained significantly higher (OR: 2.08, 95% CI: 1.03-4.21, p = 0.042) in young patients compared to elderly patients (Fig.4). In addition, young patients were also found to have significantly higher percentage of multiple lesions in both anterior and posterior circulations (7.2% vs. 0%,p = 0.022) than elderly patients (Fig.5). There were no significant differences of other ACI lesions patterns between two groups (all p > 0.05).Discussion
In this study, young patients were found to have significantly higher prevalence of multiple ACI lesions in more than one vascular territory than elderly patients. Data on the comparison of distribution patterns of ACI lesions between the two groups are scarce. Roh et al have reported that multiple infarcts in more than one vascular territory strongly argue for a proximal source or systemic cause. 5 In addition, we found that young patients had significantly higher percentage of lesions in both anterior and posterior circulations than elderly patients. Previous studies have shown that the ACI lesions in both anterior and posterior circulations were significantly associated with a cardiac embolic source. 4 The findings in the present study imply that young patients with ACI lesions might be more prone to suffering from embolization, suggesting that more attention needs to be paid for identifying the embolism-related diseases in the etiological diagnose of stroke in young patients with intracranial large artery stenosis.Conclusion
In the ACI patients of intracranial large artery stenosis, young patients had higher prevalence of multiple ACI lesions in more than one vascular territory and higher percentage of lesions in both anterior and posterior circulations than elderly patients.Acknowledgements
NoneReferences
- George MG, Tong X, Bowman BA. Prevalence of Cardiovascular Risk Factors and Strokes in Younger Adults. JAMA Neurol. 2017;74(6):695-703.
- Kono Y, Terasawa Y, Sakai K, et al. Risk factors, etiology, and outcome of ischemic stroke in young adults: A Japanese multicenter prospective study. J Neurol Sci. 2020;417:117068.
- Kang DW, Chalela JA, Ezzeddine MA, et al. Association of ischemic lesion patterns on early diffusion-weighted imaging with TOAST stroke subtypes. Arch Neurol. 2003;60(12):1730-1734.
- Wessels T, Wessels C, Ellsiepen A, et al. Contribution of diffusion-weighted imaging in determination of stroke etiology. Am J Neuroradiol. 2006;27(1):35-39.
- Roh JK, Kang DW, Lee SH, et al. Significance of acute multiple brain infarction on diffusion-weighted imaging. Stroke. 2000;31(3):688-694.
Figures
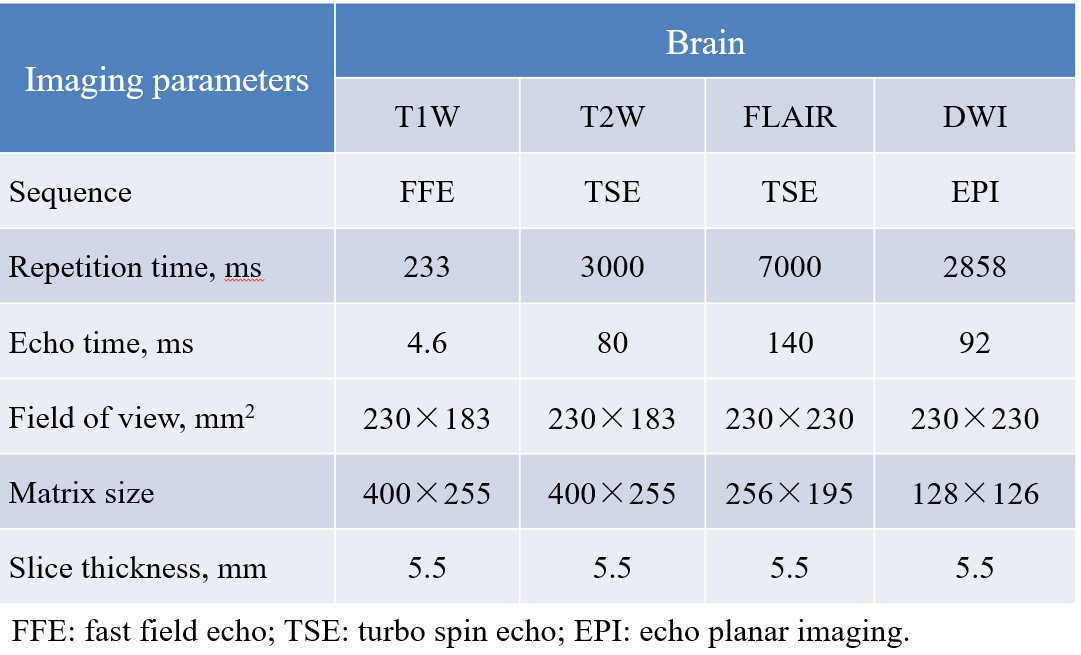
Fig.1. Parameters
of brain imaging.
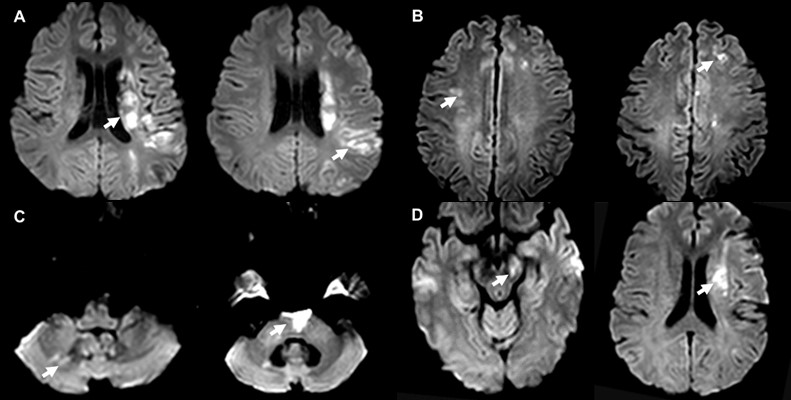
Fig.2. Patterns
of multiple acute cerebral infarction lesions on DWI. A, multiple lesions in one
vascular territory. B, multiple lesions in bilateral anterior circulations. C, multiple lesions in the posterior circulation. D, multiple
lesions in both anterior and posterior circulations.
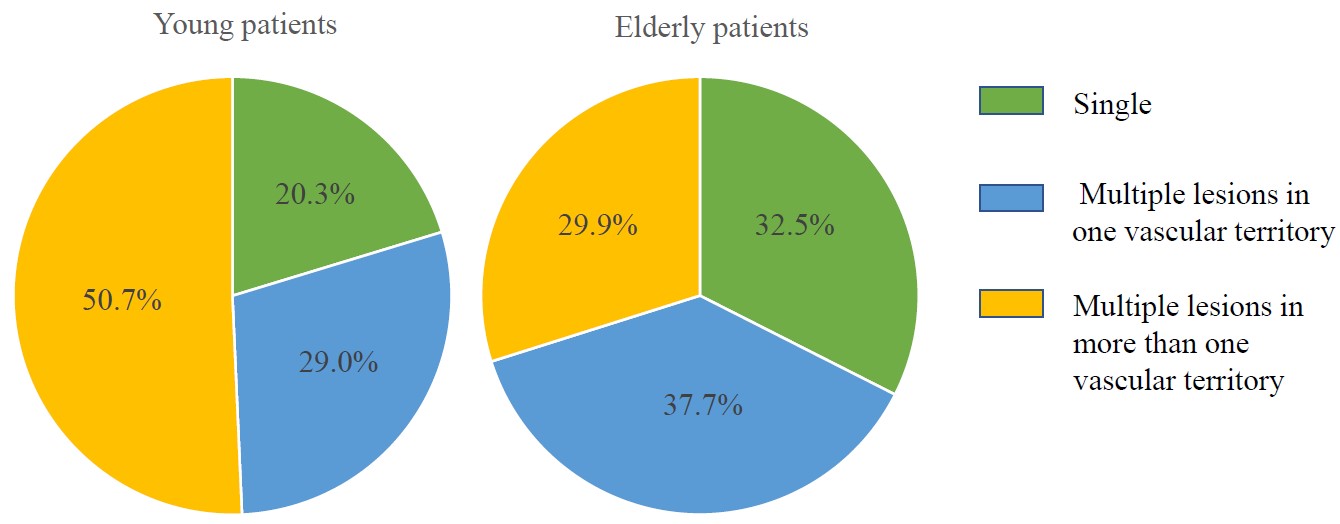
Fig.3.
Comparison of acute cerebral infarction patterns between young and elderly
patients. The left and right pies above showed the percentage of different distribution
patterns of acute cerebral infarction lesions in young and elderly patients, respectively.
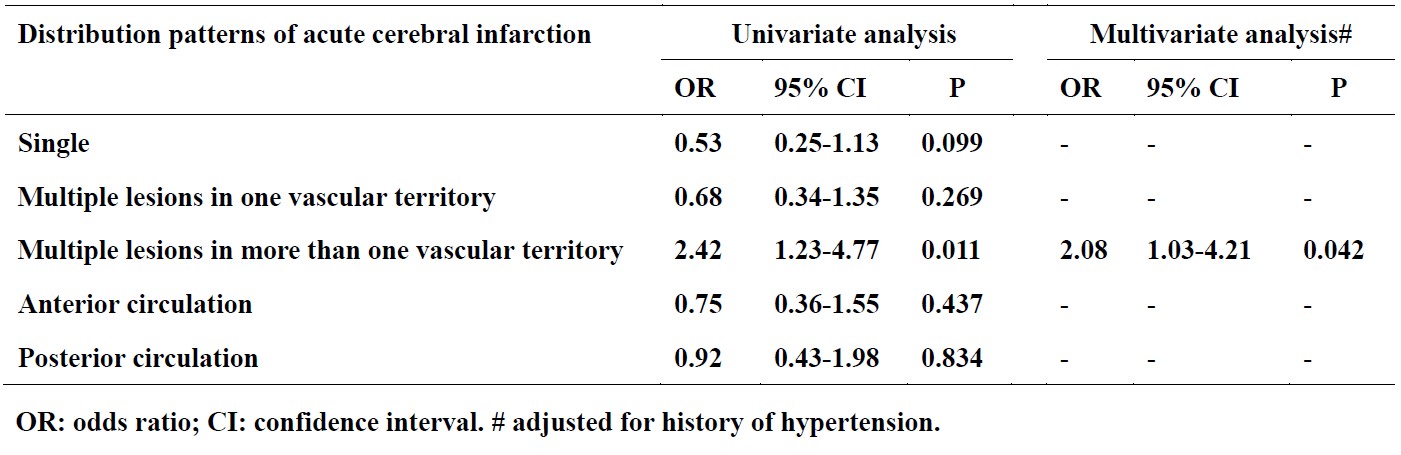
Fig.4. Multiple
logistic regression models for comparing the distribution patterns of acute
cerebral infarction lesions between young and elderly patients.
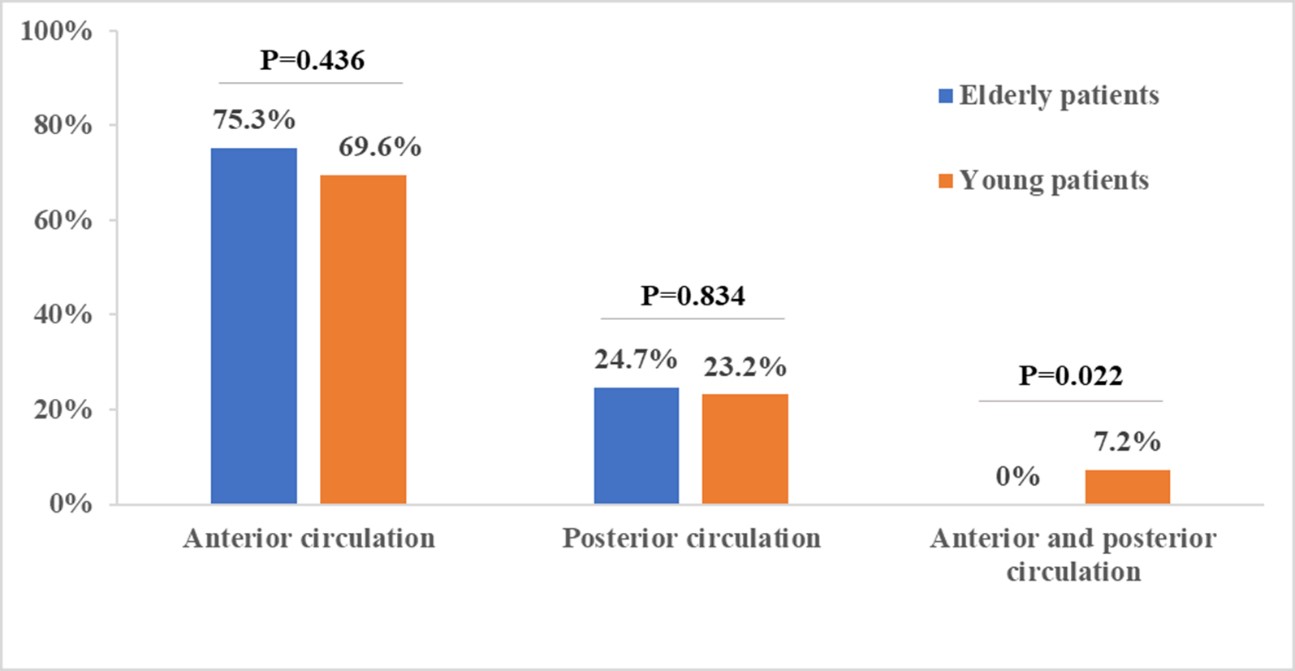
Fig.5. Bar
charts of vascular territory patterns of acute cerebral
infarction lesions between
young and elderly patients. Young patients had significantly higher percentage
of lesions in both anterior and posterior circulations than elderly patients.