4101
Standardization of SE-MRE at 3.0T for the prostate.1Magnetic Resonance, Fundacion Escuela de Medicina Nuclear, Mendoza, Argentina, 2Magnetic Resonance, Fundación Argentina para el Desarrollo en Salud, Mendoza, Argentina, 3Universidad de Mendoza, Mendoza, Argentina, 4Universidad Nacional de Cuyo, Mendoza, Argentina, 5Comisión Nacional de Energía Atómica, Mendoza, Argentina, 6Hospital Italiano, Mendoza, Argentina
Synopsis
MRE generates quantitative information of shear modulus. Several challenges exist for the assessment of prostate. Difficulties with wave propagation due to the central location of the prostate, have induced the development of different techniques including transurethral and endorectal drivers. The objectives of this work were to study the 3.0 Tesla trans-pelvic MRE performance in PCa at a standard excitation frequency (⍵) of 60 Hz, as well as the reproducibility of µ at different ⍵ values. In 43 patients, the MRE were acquired using five 2D-SE sequences (⍵ values: 40, 50, 60, 70 and 80 Hz) and GRE 2D sequences
INTRODUCTION
The magnetic resonance multiparametric protocol (mpMR) for prostate cancer (PCa) diagnosis includes images for morphological evaluation, diffusion techniques to cell density analysis, and perfusion sequences for neovascularization evaluation. Magnetic resonance elastography (MRE) generates quantitative information of shear modulus (µ) from the displacement tensor (u) obtained with a sequence that uses a motion-encoding gradient (MEG) to characterize the movement. The vector µ is found from the Helmholtz equation, taking into account local homogeneity, negligible contributions of longitudinal waves and tissue incompressibility.Several challenges exist for the assessment of prostate MRE. Difficulties with wave propagation due to the central location of the prostate, have induced the development of different techniques including transurethral and endorectal drivers. The approach of endorectal drivers allows application of higher mechanical vibrations but is more invasive than approaches as trans-pelvic drivers with externally placed drivers.
The objectives of this work were to study the 3.0 Tesla trans-pelvic MRE performance in PCa at a standard excitation frequency (⍵) of 60 Hz (spin echo -SE- and gradient echo -GRE-), as well as the reproducibility of µ at different ⍵ values.
METHODS
This is a prospective randomized evaluation approved by the institutional review board. A total of 43 patients (mean age: 67±9 years), during a 3 years period, were referred to our institution because of increased PSA serum levels or suspicious digital exam. A complete mpMR was performed using a 3.0T PET-MRI General Electric scanner. All lesions were characterized following the PI-RADS v2 guidelines. The MRE were acquired using five 2D-SE sequences (⍵ values: 40, 50, 60, 70 and 80 Hz) and GRE 2D sequences. A circular passive driver was placed in the abdominal wall at the hypogastrium over the pubic symphysis. Two independent abdominal radiologists (4 years of expertise on MRE) evaluated the studies. The mpMR was classified as suspicious when PR-4/5, indeterminate when PR-3 or non-suspicious when PR-1/2. Readers manually trace a ROI in areas of normal and suspicious tissue in accordance with the confidence map (CMp) and following the PI-RADS segmentation.The results were compared with the mpMR protocol and biopsy. The use of the Shapiro-Wilk test led to the implementation of ANOVA test. Groups were compared using a F Two-Sample test. A ROC curve was used to find the cutoff value and p<0.05 was considered statistically significant.
RESULTS
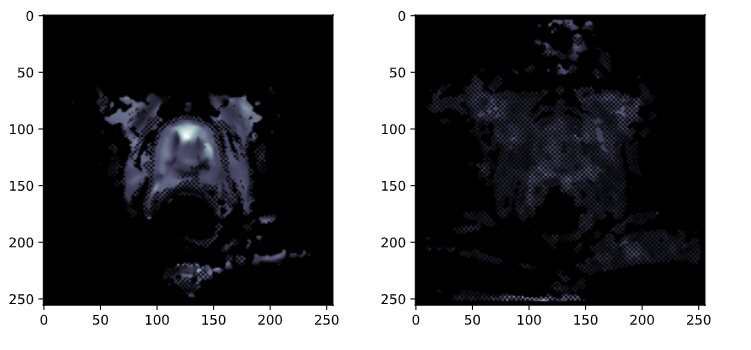
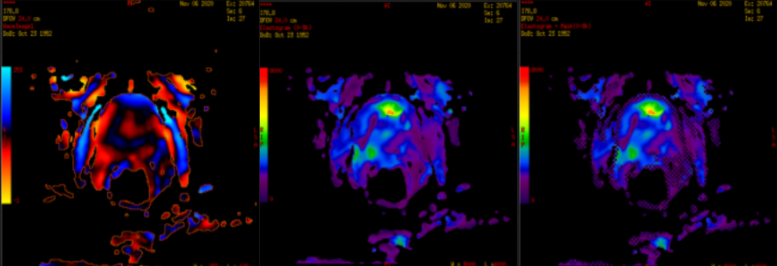
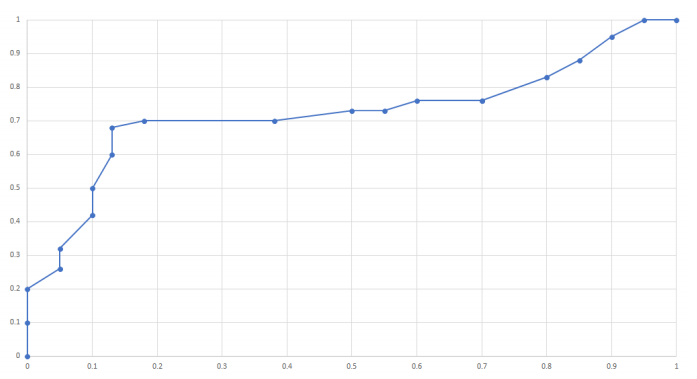
Analyzing the mpMR, 66 lesions were evaluated in 43 subjects; 6 lesions (4 patients) were not characterized by MRE (incorrect setup). From the 60 lesions with corresponding µ values, 30 were classified as PR4/5, 7 as PR3 and 23 as PR1/2. In the 60 Hz 2D-SE-MRE protocol, there was a 100% agreement between both readers; a significantly higher µ was found in nodules classified as PR-4/5 or biopsy-proven cancer, compared with PR-1/2 group (p<0.0001); while no significant difference was found comparing PR-4/5 with PR-3 (p=0.1) and PR-1/2 with PR-3 (p=0.23). The ROC curve determined a cut-off value between PR-1/2 and PR-4/5 of 4.4 kPa. With this value, the binary classifiers of both the standard mpMR and the mpMR combined with the MRE (mpMR+MRE) were evaluated. For mpMR: TPR 78%, TNR 89%, PPV 64% and NPV 92%, mpMR+MRE: TPR 89%, TNR 94%, PPV 84% and NPV 95%Only 5 lesions could be characterized with the GRE-MRE sequence based on the CMp, with a percentage difference of 9% compared to the 60 Hz SE-MRE. A root mean square adjustment of µ was carried out as a function of ⍵ for each pixel, considering the five frequencies used. Taking into account the speed of sound in a solid, a quadratic function was fitted to determine in which regions there were considerable variations of µ. The biggest changes were found in lesions with high µ values.
DISCUSSION
It is necessary to increase the amount of patients especially in the PR3 group (at least 20 more lesions), which reflects a difficulty for the radiologist due to the complex definition of injuries that this category involves . It is necessary to redesign the configuration of the MRE-GRE sequence and improve its signal noise ratio (SNR) at the cost of increasing its duration to a time similar to the MRE-SE sequence. This methodology would be a more appropriate way to compare these two techniques, since acquisition time is one of the variables that most influences the cost / benefit evaluation and the efficiency of a protocol.CONCLUSION
The speed of the MRE-GRE sequences is not a variable that symbolizes a higher medical gain than the better radiological performance of the MRE-SE sequences, in addition to the fact that the latter consumes an average of 40% more time. Regarding the results with MRE-SE, the cut-off value of 4.4 kPa makes it possible to establish that trans-pelvic prostate MRE is a method capable of differentiating malignant tissue from normal tissue. The mpMR + MRE values reflect an average increase close to 10% in the binary classifiers when the MRE is implemented in the standard mpMR protocol. Regarding the results with the frequency variations, it is necessary to take into account the tissue density in the calculation of µ since the stiffness was not kept constant in the regions of higher density.Acknowledgements
No acknowledgement found.References
[1] S. K. Venkatesh, M. Yin, and R. L. Ehman, “Magnetic resonance elastography of liver:Technique, analysis, and clinical applications,” Journal of Magnetic Resonance Imaging,vol. 37, no. 3, pp. 544–555, 2013.
[2] Hennedige Tiffany, HallinanJames Thomas Patrick Decourcy, “Comparison of magnetic resonance elastographyand diffusion-weighted imaging for differentiating benign and malignant liver lesions,”European Radiology, vol. 26, no. 2, pp. 398–406, 2016.
[3] S. Li, M. Chen, W. Wang, W. Zhao, J. Wang, X. Zhao, and C. Zhou, “A feasibilitystudy of mr elastography in the diagnosis of prostate cancer at 3.0t,” Acta Radiologica,vol. 52, no. 3, pp. 354–358, 2011. PMID: 21498375.
Figures