4091
Comparison of single-shot EPI DWI, multi-shot EPI DWI, and single-shot EPI DWI using Compressed SENSE framework in prostate
Ayumu kido1, Tsutomu Tamada1, Yu Ueda2, Masami Yoneyama2, Jaladhar Neelavalli3, and Akira Yamamoto1
1Kawasaki Medical School, Okayama, Japan, 2Philips Japan, Tokyo, Japan, 3Philips India, Bangalore, India
1Kawasaki Medical School, Okayama, Japan, 2Philips Japan, Tokyo, Japan, 3Philips India, Bangalore, India
Synopsis
Single-shot EPI (sshEPI) DWI still suffers from distortion and blurring. Multi-shot EPI (mshEPI) DWI called IRIS and sshEPI DWI using C-SENSE (a combination of parallel imaging and compressed sensing) enables to reduce distortion and blurring. A total of 14 prostate cancer (PC) patients underwent mpMRI including sshEPI DWI, IRIS, and sshEPI DWI using C-SENSE under the same scan time. The sshEPI DWI has comparable the diagnostic performance of PC equivalent to sshEPI DWI using C-SENSE and IRIS, whereas sshEPI DWI using C-SENSE and IRIS improve the image distortion and image blurring compared to sshEPI DWI.
INTRODUCTION:
DWI is key component of multi parametric MRI (mp-MRI) in prostate1, 2. Single-shot EPI (sshEPI) DWI is the most commonly used in routine clinical examination thanks to high SNR, rapid acquisition, and insensitive to motion. On the other hand, drawbacks are mainly distortion due to B0 inhomogeneity and blurring due to T2* attenuation. Parallel imaging3, 4 made it possible to reduce distortion and blurring dramatically, but sshEPI DWI still suffers from them, especially in the presence of rectal gas and higher resolution image respectively. Multi-shot EPI (mshEPI) DWI called IRIS5, which acquires the k-space data in multiple excitations, can reduce distortion and blurring due to shorter shot length, whereas it is sensitive to motion due to phase differences between shots. IRIS can provide robust image quality even in the presence of tissue motion as rejection/reacquisition function is newly implemented. Recently, it has been reported that a combination of parallel imaging and compressed sensing (C-SENSE) could clearly reduce noise-like artifacts and significantly improve the image quality of EPI DWI6. Therefore, sshEPI DWI using C-SENSE enables to reduce distortion and blurring with higher reduction factor compared to conventional sshEPI DWI. The purpose of this study is to compare sshEPI DWI, IRIS, and sshEPI DWI using C-SENSE under the same scan time to investigate clinical feasibility of IRIS and sshEPI DWI using C-SENSE for prostate cancer (PC).METHODS:
A total of 14 patients with pathologically biopsy proven PC (mean age, 74 years) underwent mpMRI including DWI on a 3-T system with a32-channel phased-array coil (Ingenia Elition 3.0T; Philips Healthcare, Best, The Netherlands) before prostate biopsy. Axial sshEPI DWI, IRIS, and sshEPI DWI using C-SENSE were acquired with the imaging parameters described in Figure 1. The same parameters were used in this study except for the number of shots, EPI factor, number of signals averaged (NSA), and reduction factor. NSA in sshEPI DWI and sshEPI DWI using C-SENSE was optimized so that scan time in sshEPI DWI and sshEPI DWI using C-SENSE are the same as that of IRIS. In qualitative visual assessment, anatomical distortion score of prostate (AD, 1=severe; 2=moderate, 3=mild; 4=none), lesion conspicuity score (LCS, 1=invisible for surrounding normal site; 2=slightly high, 3=moderately high; 4=very high), and prostate edge clarity (PEC, 1=very poor; 2=poor, 3=moderate; 4=good) were assessed. In quantitative analysis, SNR (SNR= normal prostate SI (mean) / internal obturator muscle standard deviation (SD)), contrast to noise ratio (CNR= lesion SI (mean) - normal prostate SI (mean) / internal obturator muscle SD), and apparent diffusion coefficient (ADC, ×10-3 mm2/s) of the lesion (ADCmean) and normal peripheral zone (PZ) (ADCmean) were measured. AD, LCS, PEC, SNR, and CNR were compared between sshEPI DWI, IRIS, and sshEPI DWI using C-SENSE. In addition, ADCmean between normal PZ and lesion was compared in three group. Friedman and Wilcoxon signed rank tests were used for statistical analysis.RESULTS:
The PC was in the PZ in 36% (5 of 14), in the transition zone (TZ) in 57% (8 of 14), and in both PZ and TZ in 7% (1 of 14). First of all, IRIS provided robust image quality for respiratory and peristaltic motion in prostate thanks to rejection/reacquisition function. In analyses of image quality, there was significant difference among three acquisition methods for AD and PEC (P <0.01, both) (Figures 2 and 3). AD in IRIS was significantly higher than that of sshEPI DWI (3.36 ± 0.63 vs. 2.86 ± 0.53, P = 0.02). PEC in IRIS and sshEPI DWI using C-SENSE was significantly higher than that of sshEPI DWI (3.5±0.52 vs. 2.21±0.43, P<0.01 and 2.5±0.52 vs. 2.21±0.43, P=0.046). However, SNR and CNR in sshEPI DWI was significantly higher than those of IRIS and sshEPI DWI using C-SENSE (P=0.048 to <0.001 and P=0.019 to 0.001, respectively). In analyses of tumor detection ability, LCS was comparable among three groups (P=0.368). On the other hand, in sshEPI DWI, IRIS and sshEPI DWI using C-SENSE, lesion ADCmean was significantly lower than normal ADCmean (P=0.001, respectively). DISCUSSION: In comparison of the image quality, SNR and CNR were higher in sshEPI DWI than in IRIS and sshEPI DWI using C-SENSE under the same scan time, and the image distortion and image sharpness such as AD and PEC showed better results in IRIS and sshEPI DWI using C-SENSE than in sshEPI DWI. In comparison of the tumor detection ability in PC, LCS and tumor ADCmean were also comparable between sshEPI DWI, IRIS, and sshEPI DWI using C-SENSE. Interestingly, sshEPI DWI acquired over a little longer time (265 sec.) than usual clinical situation (about 2 min.) has the same diagnostic performance as IRIS and sshEPI DWI using C-SENSE which can reduce distortion and blurring. On the other hands, it is expected that IRIS and sshEPI DWI using C-SENSE which can reduce distortion and blurring compared to sshEPI DWI contribute to improved diagnostic performance of local staging such as extracapsular extension.CONCLUSION:
The present findings suggest that sshEPI DWI has comparable diagnostic performance of PC equivalent to sshEPI DWI using C-SENSE and IRIS, whereas sshEPI DWI using C-SENSE and IRIS improve the image distortion and image blurring compared to sshEPI DWI.Acknowledgements
No acknowledgement found.References
- Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019;76(3):340-351.
- Le Bihan D. Apparent diffusion coefficient and beyond: what diffusion MR imaging can tell us about tissue structure. Radiology. 2013;268(2):318–322.
- Pruessmann KP, Weiger M, Scheidegger MB et al. SENSE: Sensitivity encoding for fast MRI. Magn Reson Med. 1999;42(5):952-962.
- Griswold MA, Jakob PM, Heidemann RM et al: Generalized autocalibrating partially parallel acquisitions (GRAPPA). Magn Reson Med. 2002;47(6):1202-1210.
- Jeong HK, Gore JC, Anderson AW. High-resolution human diffusion tensor imaging using 2-D navigated multishot SENSE EPI at 7 T. Magn Reson Med. 2013;69(3):793-802.
- Yoneyama M, Morita K, Peeters J et al. Noise Reduction in Prostate Single-Shot DW-EPI utilizing Compressed SENSE Framework. Proceedings of the 27th Annual Meeting of ISMRM, 2019 #1634
Figures
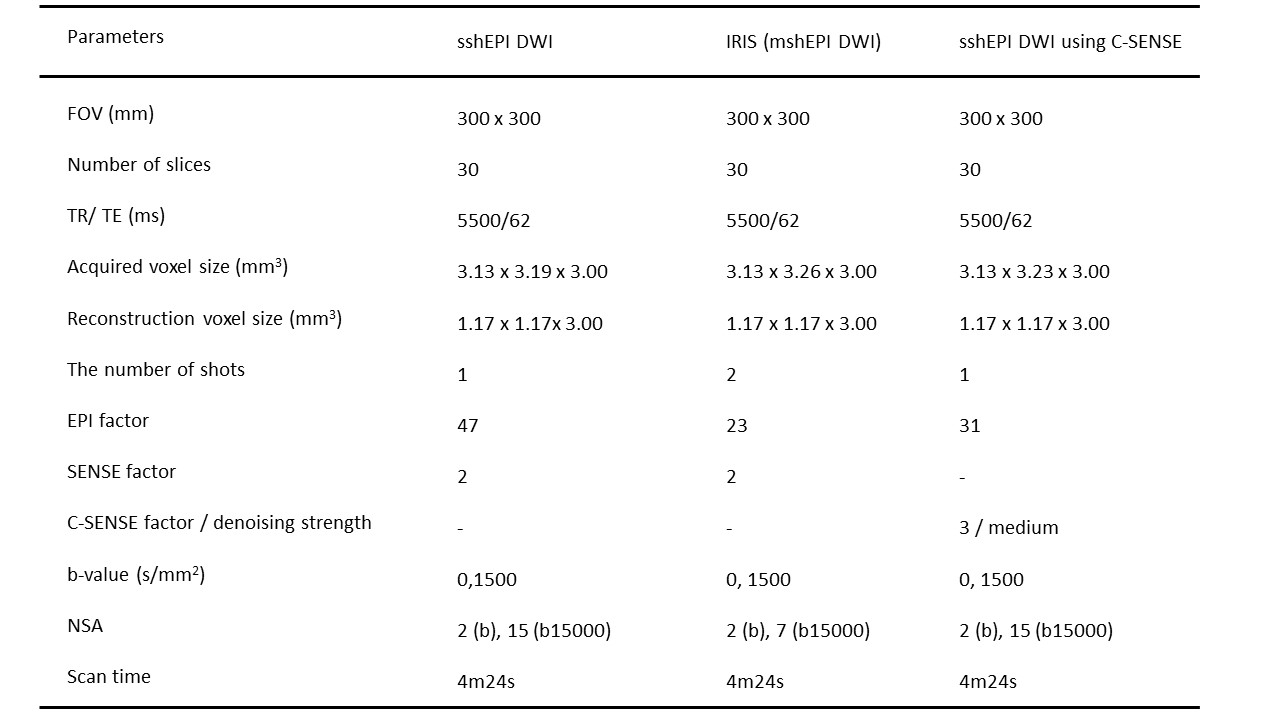
Details of the imaging parameters

A 80-year-old male with prostate cancer (PSA level of 13.69 ng/mL, Gleason score of 3+4) in the transitional zone. Cancer lesion is shown as a homogeneous hypointense lesion with mass effect on T2-weighted imaging (A). The lesion with focal hyperintensity is depicted clearly in the three DWI image (sshEPI DWI, sshEPI DWI using C-SENSE, and IRIS) (B, C and D). SNR and CNR is higher in sshEPI DWI than in sshEPI DWI using C-SENSE and IRIS, whereas sharpness in sshEPI DWI using C-SENSE and IRIS is better than sshEPI DWI.

A 83-year-old male with prostate cancer (PSA level of 6.6 ng/mL, Gleason score of 3+4) in the peripheral zone. Cancer lesion is not shown on three DW images. These images show distortion of the prostate caused by rectal air. IRIS (C) can reduce rectal gas induced distortion compared to sshEPI DWI (A) and sshEPI DWI using C-SENSE (B).