4089
Prostate MRI at 3-T: clinical impact of ultra-high b value (3,000 s/mm2) diffusion-weighted MR imaging compared to high b value of 2,000 s/mm2
Ayumu Kido1, Tsutomu Tamada1, Yu Ueda2, Masami Yoneyama2, and Akira Yamamoto1
1Radiology, Kawasaki Medical School, Okayama, Japan, 2Philips Japan, Tokyo, Japan
1Radiology, Kawasaki Medical School, Okayama, Japan, 2Philips Japan, Tokyo, Japan
Synopsis
High b value DWI (b2000) shows insufficient image contrast between benign and malignant tissues and much overlap between ADCs of low grade and those of high-grade prostate cancers (PCs). Forty-nine patients with PC underwent multiparametric MRI including ultra-high b value DWI (b3000) and high b value DWI. Signal intensity of normal prostate was significantly lower in b3000 than in b2000. Other image quality parameters, tumor detection ability, and discrimination ability of PC aggressiveness between b3000 and b2000 were comparable. Compared with high b value DWI, ultra-high b value DWI could not contribute to increased diagnostic performance in PC.
INTRODUCTION:
Diffusion-weighted imaging (DWI) is key components of prostate multiparametric MRI.1-3 High b value DWI such as b value of 2,000 s/mm2, which is commonly used in daily clinical practice shows insufficient image contrast between benign and malignant tissues and much overlap between ADCs of low grade prostate cancers (PCs) and those of high-grade PCs.4 Therefore, higher b value DWI is needed to improve the clinical performance of PC detection and ADC measurements. In the acquisition of higher b value DWI, a state-of-the-art 3-T MRI with the extremely high gradient waveform fidelity (≈100%) resulting from improved eddy current calibration and the maximum gradient strength alongside maximum slew rate due to precisely calculated coil design and high cooling efficiency may improve signal to noise ratio (SNR) of DWI and has potential for clinical application of ultra-high b value DWI. Thus, the aim of this study was to compare the image quality, PC detection ability, and discrimination ability of tumor aggressiveness in PC between ultra-high b value DWI and high b value DWI using 3-T system.METHODS:
Forty nine patients (mean age, 72 years) with pathologically proven PC who underwent multiparametric MRI on a 3T system (Ingenia Elition 3.0T; Philips Healthcare, Best, The Netherlands) with a 32-channel phased array coil were included in the study. Axial fat-suppressed single-shot echo-planar DWI was acquired with b values of 0, 2000, and 3000 s/mm2 [TR/TE 5000/69 ms; slice thickness 3 mm; no intersection gap; FOV 300×300 mm, matrix 80×80, in-plane resolution 3.75×3.75 mm2, parallel imaging factor 2]. In qualitative visual assessment, anatomical distortion score of prostate (AD, 1=severe; 2=moderate, 3=mild; 4=none), signal intensity (SI) of normal prostate (PSI, 1=very high; 2=moderately high, 3=slightly high; 4=iso intensity), and lesion conspicuity score (LCS, 1=invisible for surrounding normal site; 2=slightly high, 3=moderately high; 4=very high) were assessed, and in quantitative analysis, SNR (SNR= normal prostate SI (mean) / internal obturator muscle SI (standard deviation (SD)), contrast to noise ratio (CNR= lesion SI (mean) - normal prostate SI (mean) / internal obturator muscle SI (SD)), and mean apparent diffusion coefficient (ADC, ×10-3 mm2/s) of the lesion (lADC) and normal peripheral zone (PZ) (nADC) were measured.RESULTS:
The 49 PCs comprised GS=3+3 (GG1) in 9 tumors, GS=3+4 (GG2) in 22 tumors, GS=4+3 (GG3) in 9 tumors, GS=4+4 (GG4) in 3 tumors, and GS=4+5 (GG5) in 6 tumors. PSI was significantly higher in b3000 than in b2000 (3.06 ± 0.52 vs. 2.27 ± 0.57, P < 0.001) (Figure). AD, LCS, SNR, and CNR were comparable between b3000 and b2000 (P = 0.180 to P = 0.665). On the other hand, in both b3000 and b2000, lADC was significantly lower than nADC (0.56 ± 0.09 vs. 1.03 ± 0.12, P < 0.001 and 0.68 ± 0.13 vs. 1.40 ± 0.27, P < 0.001). There was significant negative correlation between lADC and GG in both b2000 and b3000 (ρ= - 0.336, P = 0.018 andρ= - 0.290, P = 0.043, respectively). In comparison of lADC between tumors with ≤ GG2 and tumors with ≥GG3, both b3000 and b2000 had significant difference (0.72 ± 0.12 vs. 0.62 ± 0.11, P = 0.007 and 0.59 ± 0.09 vs. 0.52 ± 0.08, P = 0.021). In ROC analysis, the AUC for separating tumors with ≤ GG2 from tumors with ≥GG3 was 0.731 in b2000 and 0.699 in b3000, and there was no significant difference in the AUC between both b values (P = 0.161).DISCUSSION:
In the comparison of image quality using AD and SNR, b3000 was equivalent to b2000. SI of normal prostatic parenchyma in b3000 was lower than that in b2000. These results suggest that ultra-high b value DWI at b3000 using a state-of-the-art 3-T MRI system has image quality that can be applied clinically and strong suppression effect of background signal which is expected to improve contrast with lesions. However, the results of qualitative and quantitative tumor detection ability using LCS, CNR, and ADCmean between normal PZ and PC was comparable between b3000 and b2000. In addition, qualitative discrimination ability between clinically significant PC (tumors with ≥GG3) and clinically insignificant PC (tumors with ≤ GG2) using ADC was also comparable between b3000 and b2000. Therefore, even the ultra-high b value DWI at b3000, which has the same or better image quality as the b2000 and higher diffusion-weighted effect failed to show improved the PC detection ability and the discrimination ability of risk stratification in PC compared to b2000. In other words, in current daily clinical practice, the optimal b value of prostate DWI for PC tumor detection and assessment of tumor aggressiveness in PCwill be around b=0, 2000 s/mm2.CONCLUSION:
The present findings suggest that a state-of-the-art 3-T MRI was able to achieve the acquisition of ultra-high b value DWI at b values of 0 and 3000 s/mm2, which has strong background signal suppression effect while maintaining the same image quality as high b value DWI. However, compared with high b value DWI, ultra-high b value DWI could not contribute to increased diagnostic performance including PC detection and assessment of tumor aggressiveness in PC.Acknowledgements
No acknowledgement found.References
- Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019;76(3):340-351.
- Le Bihan D. Apparent diffusion coefficient and beyond: what diffusion MR imaging can tell us about tissue structure. Radiology. 2013;268(2):318–322.
- Tamada T, Sone T, Jo Y, et al. Diffusion-weighted MRI and its role in prostate cancer. NMR Biomed. 2014;27(1):25-38.
- Tamada T, Kanomata N, Sone T, et al. High b value (2,000 s/mm2) diffusion-weighted magnetic resonance imaging in prostate cancer at 3 Tesla: comparison with 1,000 s/mm2 for tumor conspicuity and discrimination of aggressiveness. PLoS One. 2014;9(5):e96619.
Figures
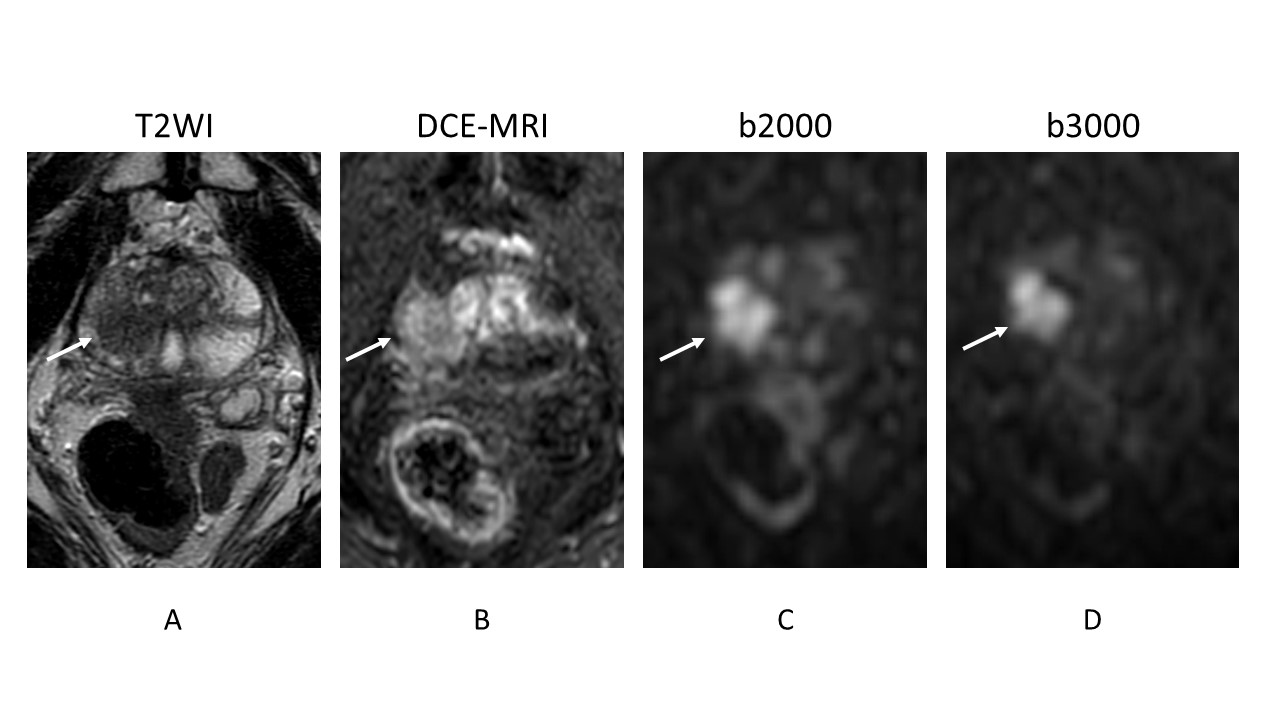
Prostate cancer lesion is shown as a homogeneous hypointense lesion with mass effect on T2-weighted imaging (arrow) (A) and focal early enhancement on dynamic contrast-enhanced MR imaging (arrow) (B). Signal intensity of normal prostate is lower in b3000 (D) than in b2000 (C). However, the lesion conspicuity between b2000 (arrow) and b3000 (arrow) is almost equivalent.