4087
Synthetic DWI in prostate
Yu Ueda1, Tsutomu Tamada2, Makoto Obara1, Tetsuo Ogino1, Daisuke Morimoto-Ishikawa3, Hiroyasu Sanai2, Koji Yoshida2, Ayumu Kido2, Tomoko Hyodo4, Kazunari Ishii4, Masami Yoneyama1, and Marc Van Cauteren5
1Philips Japan, Tokyo, Japan, 2Department of Radiology, Kawasaki Medical School, Okayama, Japan, 3Radiology Center, Kindai University Hospital, Osaka, Japan, 4Department of Radiology, Kindai University, Osaka, Japan, 5BIU MR Asia Pacific, Philips Healthcare, Tokyo, Japan
1Philips Japan, Tokyo, Japan, 2Department of Radiology, Kawasaki Medical School, Okayama, Japan, 3Radiology Center, Kindai University Hospital, Osaka, Japan, 4Department of Radiology, Kindai University, Osaka, Japan, 5BIU MR Asia Pacific, Philips Healthcare, Tokyo, Japan
Synopsis
The usefulness of short TR DWI in prostate has been reported. However, care should be taken when setting TR as DWI with shorter TR suffers from low SNR. It would be beneficial to generate an additional DWI with shorter TR (e.g. 1000ms) from DWIs with two different TR (e.g. conventional [long] and short TR such as 6000 and 2000ms). The synthetic DWI at b = 1000 s/mm2 (DWI1000) with shorter TR of 1000ms calculated from DWIs with TR of 6000 and 2000ms had a tendency to show better diffusion contrast compared to the real-acquired DWI1000 with long TR of 6000ms.
Introduction
DWI and ADC maps are key components of multiparametric MRI (mp-MRI) in the prostate1, 2. Recently, it has been shown that T1 may help to differentiate prostate cancer (PCa) from normal prostate tissue (NPT)3-5. We hypothesized that this T1 difference between PCa and NPT can be exploited to improve diffusion contrast, and reported the usefulness of short TR DWI6, based on the specific feature that T1 of PCa is lower than that of NPT (T1 in lesions is typically longer than in normal tissue of other organs). It has been suggested that short TR (of 1850ms) DWI in prostate has the potential to replace conventional (long TR) DWI6. DWI with shorter TR of less than 1850ms enables to improve contrast further, however it suffers from reduced SNR, which results in decreased accuracy of ADC. Therefore, it might be difficult to replace conventional DWI with DWI using shorter TR of less than 1850ms. We explored the possibility of generating an additional DWI with shorter TR (e.g. 1000ms) based on DWIs with two different TR (e.g. conventional [long] and additional short TR such as 6000 and 2000ms). We refer to this as synthetic DWI (synDWI). ADC can be calculated from DWI with conventional TR (6000ms). The goal of this study is to investigate clinical feasibility of synDWI for PCa.Methods
The study was approved by the IRB, and written informed consent was obtained from all subjects. Three patients underwent mp-MRI on an Ingenia Elition 3.0T with an anterior coil and posterior built-in coils (Philips Healthcare, Best, The Netherlands). DWI was scanned with TR of 6000ms (dynamic1) and 2000ms (dynamic2) in one single scan with the following parameters: TE 70ms, FOV 300mm, acquisition voxel size 3.1 x 3.1 x 3.0 mm3, the number of packages 1, the number of slices 20, b-values 0-1000 s/mm2, NSA 4(b=0) 10(b=1000). synDWI can be calculated on a pixel-by-pixel basis from DWIs with two different TRs, following the procedure below. The signal intensity (SI) of spin echo type DWI is given bySI = cte PD×(1-e-TR/T1)×e-TE/T2×e-bD (1)
The T1 value can be determined dividing equations 2 and 3, keeping TE and b constant:
SI in DWI with long TR = cte PD×(1-e-long TR/T1)×e-TE/T2×e-bD (2)
SI in DWI with short TR = cte PD×(1-e-short TR/T1)×e-TE/T2×e-bD (3)
Next, the [cte PD × T2 term × diffusion term] factor can be calculated using the SI, rewriting e.g. Eq. 2 as
cte PD×e-TE/T2×e-bD = SI in DWI with long TR / (1-e-long TR/T1) (4)
Finally, SI in DWI with any TR can be calculated according to Eq.1. This procedure was implemented in Python (Python 3.8). synDWI at b = 1000 s/mm2 (synDWI1000) with TR of 500, 1000, 2000, and 4000ms were generated, and contrast ratio (CR) in synDWI1000 with TR of 500, 1000, 2000, and 4000ms were compared in each patient. Moreover, CR and visual scoring were compared between synDWI1000 with TR of 1000ms and DWI1000 with TR of 6000ms.
CR = (PCaave-NPTave) / (PCaave+NPTave)
where PCaave and NPTave is the average signal in cancerous and normal tissue respectively.
Visual evaluation for comparison of contrast between PCa and NPT was conducted by a radiologist with twenty-four years of experience in MRI. It was graded using a 3-pont scale, where 1 = weak; 2= moderate; 3 = strong contrast.
Results and Discussion
CR in synDWI1000 had a tendency to show higher value in shorter TR (Figure 1). Figure 2 and 3 show representative clinical cases with PCa. synDWI1000 with shorter TR provided better contrast compared to DWI1000 with long TR. CR in synDWI1000 with TR of 1000ms was higher than that of DWI1000 with TR of 6000ms in all three patients (Figure 4a). Visual scoring in synDWI1000 with TR of 1000ms was equal to or greater than that of DWI1000 with TR of 6000ms (Figure 4b). These results indicated that shorter TR had improved clinical value of DWI, probably thanks to shorter T1 value in PCa compared to NPT. Further clinical investigation is ongoing.Conclusion
Our preliminary results show that synDWI1000 with shorter TR of 1000ms had a tendency to have better diffusion contrast compared to DWI1000 with long TR of 6000ms. Further clinical investigations are needed to assess if synDWI with shorter TR can provide better diagnostic performance than DWI with long TR.Acknowledgements
No acknowledgement found.References
- Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019;76(3):340-351.
- Tamada T, Sone T, Jo Y, et al. Diffusion-weighted MRI and its role in prostate cancer. NMR Biomed. 2014;27(1):25-38.
- Baur ADJ, Hansen CM, Rogasch J, et al. Evaluation of T1 relaxation time in prostate cancer and benign prostate tissue using a Modified Look-Locker inversion recovery sequence. Sci Rep. 2020;10(1):3121.
- Obmann VC, Boyacioglu R, Panda A, et al. T1 imaging of transition zone prostate cancer: why quantitative maps but not T1 weighted images are helpful. Proceedings of the 27th Annual Meeting of ISMRM, 2019 #1837.
- Panda A, Jiang Y, Margevicius S, et al. MR fingerprinting and ADC mapping for characterization of lesions in transitional zone of prostate. Proceedings of the 26th Annual Meeting of ISMRM, 2018 #4502.
- Ueda Y, Tamada T, Yoshida K, et al. Short TR DWI in prostate. Proceedings of the 28th Annual Meeting of ISMRM, 2020 #2423
Figures
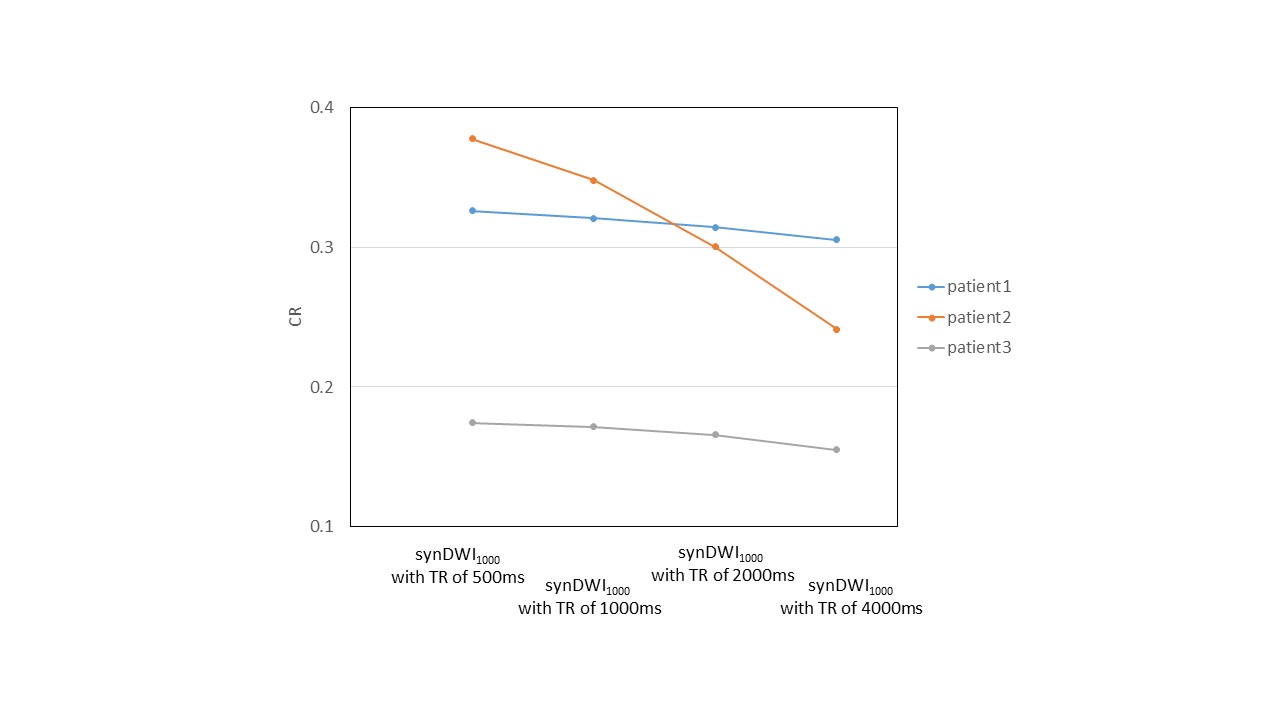
Figure 1. Comparison of contrast
ratio (CR) of prostate cancer among synDWI1000 with TR of 500, 1000, 2000, and 4000ms in three patients
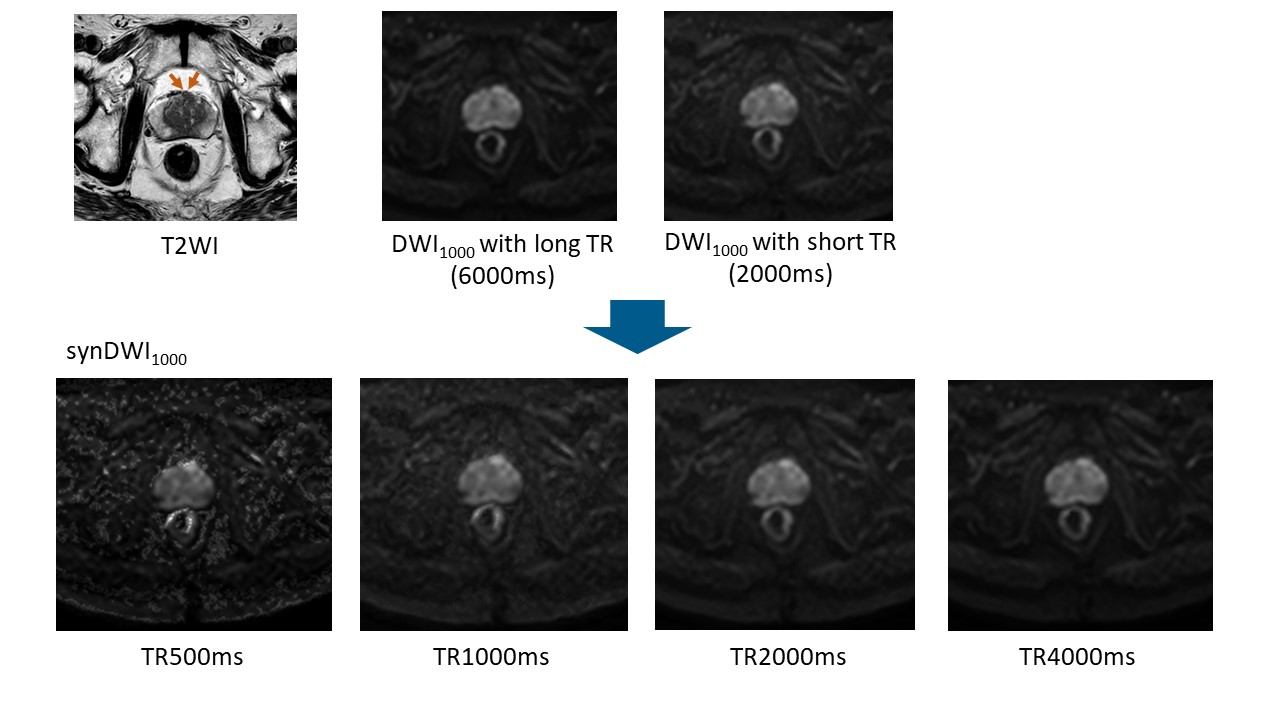
Figure 2. Prostate cancer in transitional zone. Cancer lesion
is shown as a homogeneous hypointense lesion with mass effect on T2WI (arrow). synDWI1000
with shorter TR provided better contrast than DWI1000 with long TR,
whereas noise in synDWI1000 with TR of 500ms become more visible.
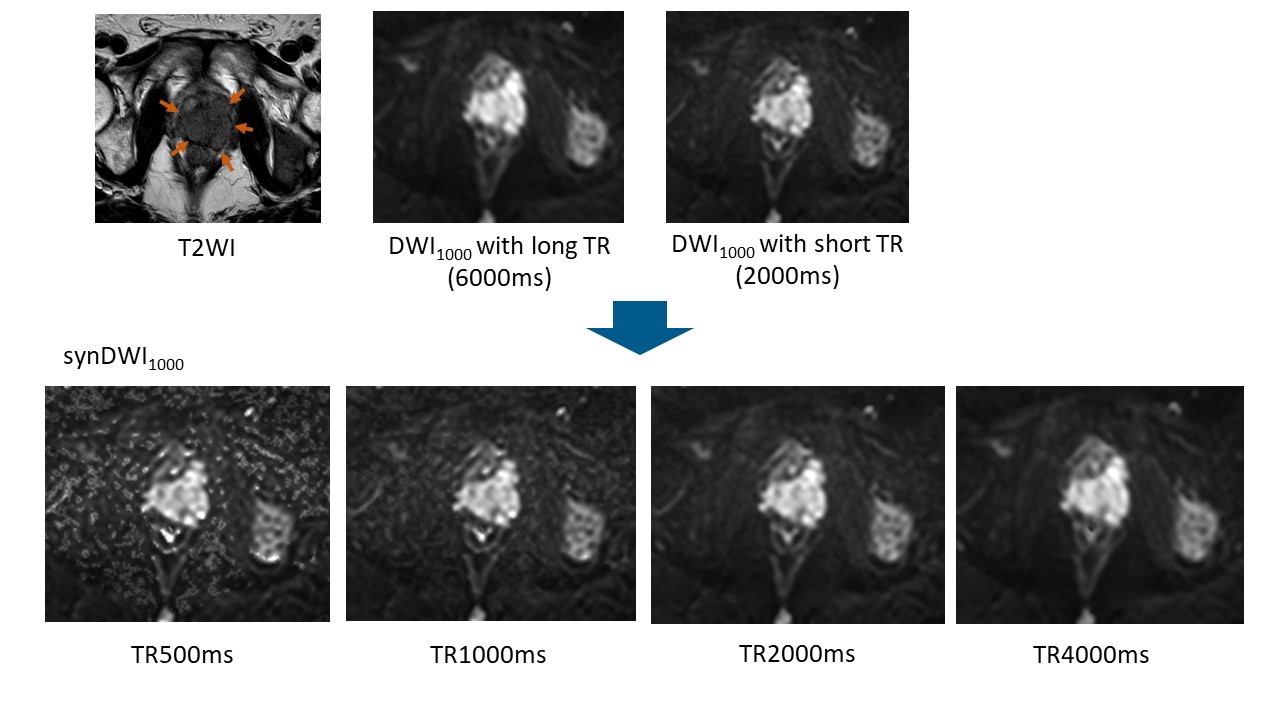
Figure 3. Prostate cancer in peripheral and transitional
zone. Cancer lesion is shown as a homogeneous hypointense lesion with mass
effect on T2WI (arrow). synDWI1000 with shorter TR provided better
contrast than DWI1000 with long TR, whereas noise in synDWI1000
with TR of 500ms become more visible.
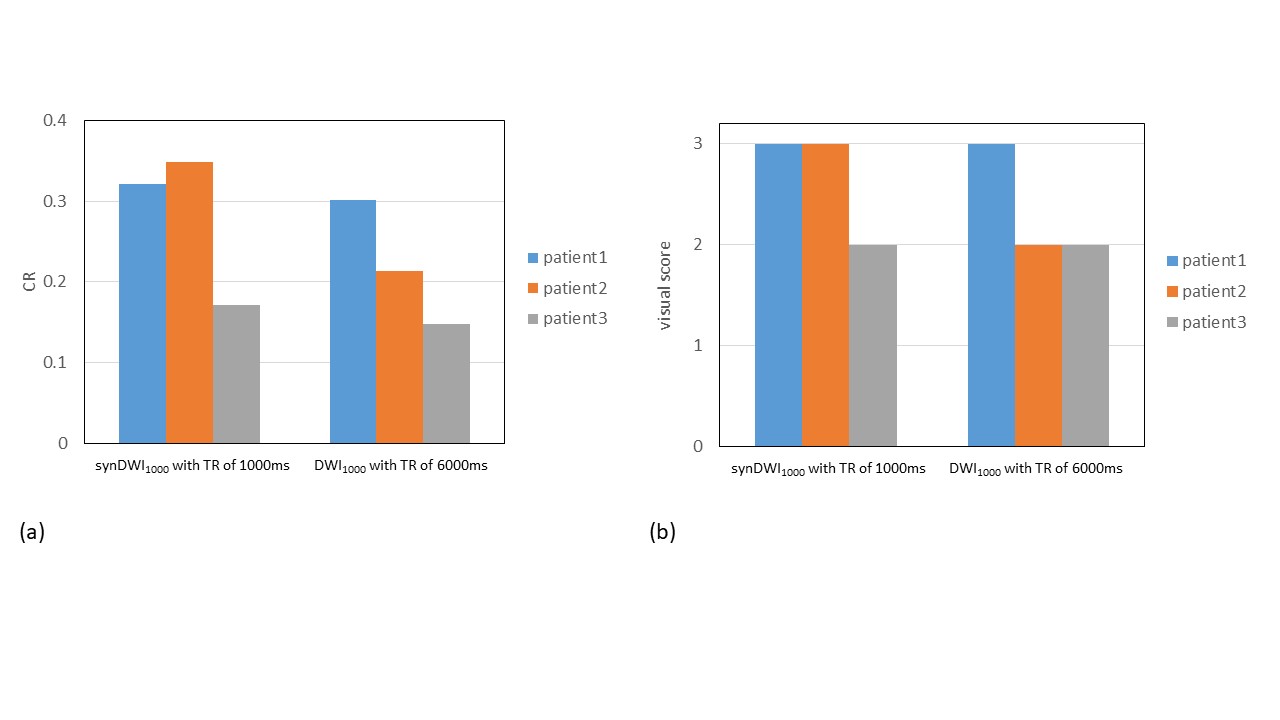
Figure 4. CR (a) and visual score (b) of prostate cancer between
synDWI1000 with shorter TR of 1000ms and DWI1000 with
long TR of 6000ms in three patients.