4073
Diagnostic performance of zero echo time imaging and T1-weighted fast spin echo on sacroiliac joint bone erosions using CT as the gold standard1Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China, 2MR Research, GE Healthcare, Beijing, China
Synopsis
Detection of sacroiliac joint (SIJ) bone erosions may improve diagnostic performance of axial spondyloarthritis (axSpA) as CT is the gold standard. Zero echo time (ZTE) MRI technique can acqire CT-like bone contrast and has been applied to bone imaging of many other body parts. Our research explored the ability of ZTE to detect SIJ bone erosions and conduct comparison of ZTE and conventional T1-weighted fast spin echo (T1 FSE). We found that ZTE had superior detection performance to T1 FSE and might be an effective supplement to routine MRI protocol in SIJs.
Introduction
Bone erosion of the sacroiliac joint (SIJ) is one of the most important manifestations of chronic structural lesions in axial spondyloarthritis (axSpA). The recommendation of bone erosion included in diagnosis could potentially improve diagnostic utility of axSpA.1,2 Computed tomography (CT) is widely regarded as the gold standard for evaluating erosions, but elevates cancer risk with times of exposure to ionizing radiation. Zero echo time (ZTE) magnetic resonance imaging (MRI) enables to capture short-T2 bone signal and thus provides CT-like bone contrast without ionizing radiation. ZTE has previously been used for bone imaging at the shoulder3 and hip.4 In this study, we assessed the detection performance of ZTE on bone erosions in SIJs using CT as the reference standard and compared it to T1-weighted fast spin echo (T1 FSE), which is the current conventional MRI sequence for structural lesions.Methods
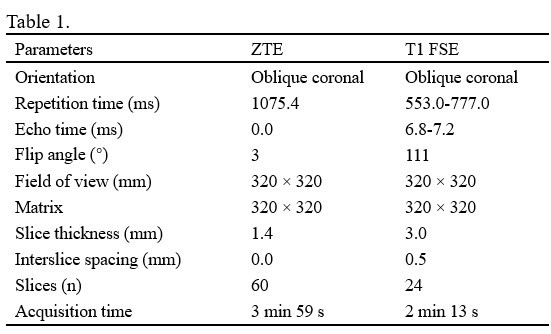
After obtaining the institutional review board approval of our hospital, 14 SIJs of 7 patients (6 males and 1 female; mean age 26.29 years; range 17-44 years) with the suspicion of axSpA were included in this study. All subjects underwent both CT and MRI (including ZTE and T1 FSE) within two weeks. CT was performed by using a 64-row scanner as described in details;5 MR images were carried out on a 3.0 T MRI system (Signa Pioneer, GE Healthcare, Milwaukee, USA) with a body coil and bed spine coil. The main parameters of ZTE and T1 FSE are presented in Table 1.Two readers who were blinded to the clinical diagnostic information assessed bone erosions of SIJs on CT, ZTE, ZTE with postprocessing,4 and T1 FSE, respectively. As described by Diekhoff et al.,6 each SIJ was divided into 12 subregions (4 quadrants in anterior, medial and posterior position), and erosions were scored 0-3 per region. In this research, erosion scores were summed on the basis of bone level (the articular surfaces of sacrum and ilium that compose SIJs)5. An erosion score of 2 or higher in any of the 6 regions was defined as positive. The sensitivity, specificity, and accuracy were calculated and CT was the reference standard; and the consistency of diagnostic results between CT and MRI was evaluated by Cohen’s κappa test. Cohen’s κappa test was also performed for assessing diagnostic agreement between two readers. The inter-image and inter-reader reliability for the erosions sum scores were evaluated using the intraclass correlation coefficient (ICC).
Results
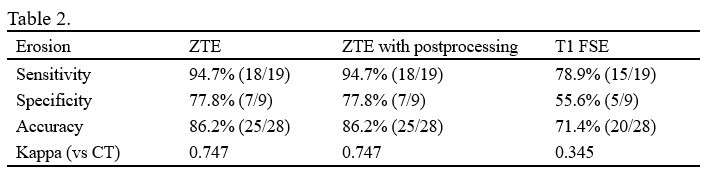
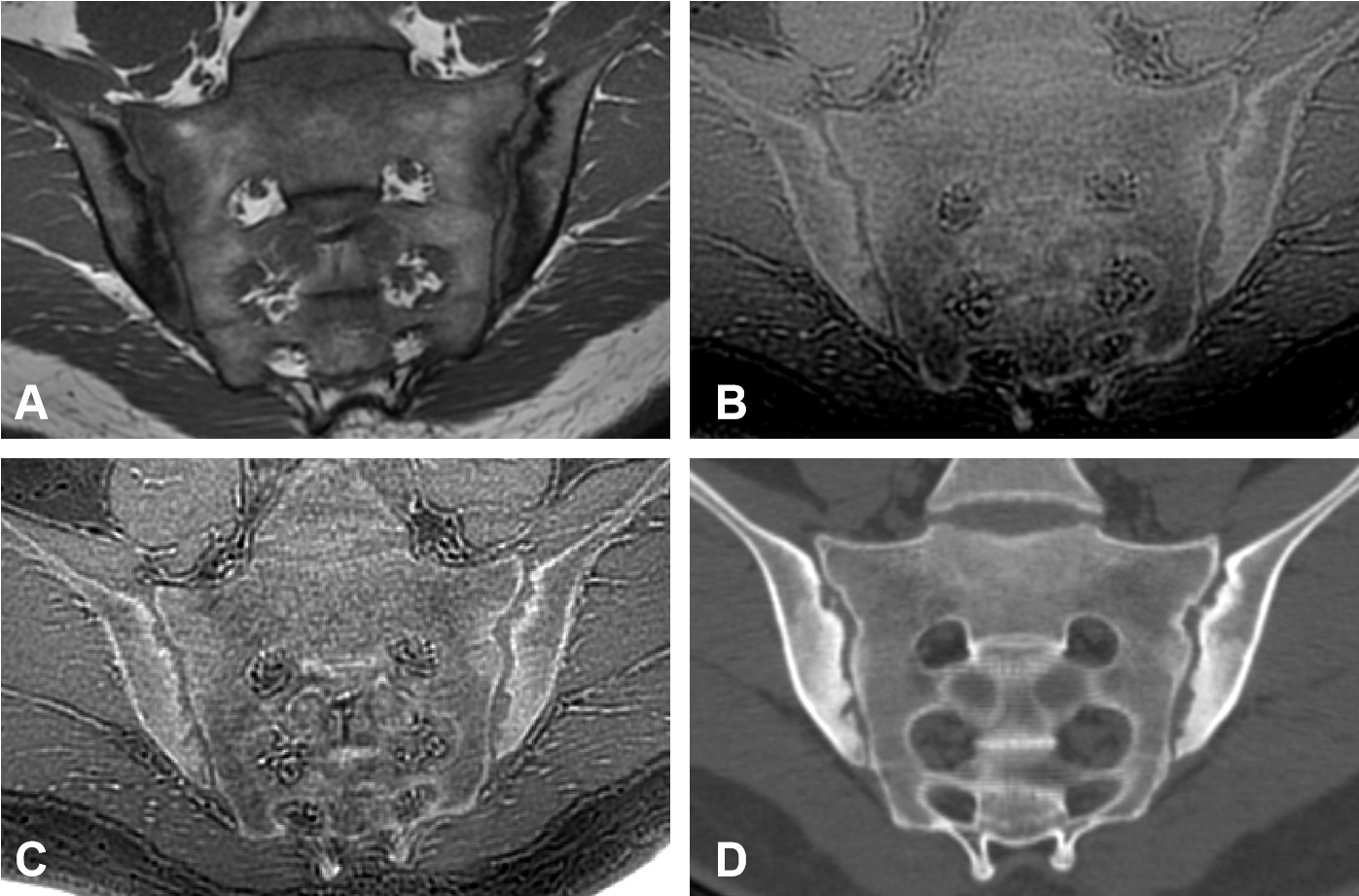
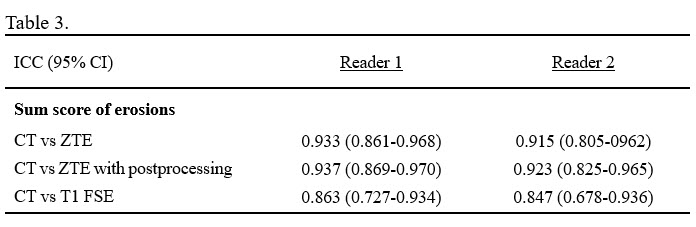
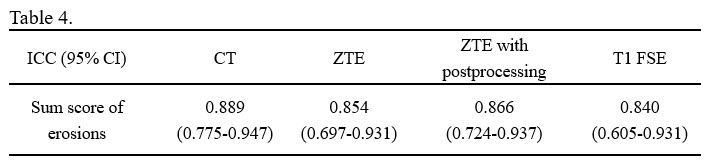
The sensitivity, specificity, and accuracy for erosion detection on bone level were shown in Table 2. The consistency between MRI and CT for positive erosion diagnosis was substantial for ZTE (κ = 0.747 both for ZTE with and without postprocessing), and fair for T1 FSE (κ = 0.345). Therefore, the diagnostic performance of ZTE was superior to T1 FSE (Figure 1). Slightly higher ICCs for erosions sum score based of ZTE than T1 FSE were shown in Table 3. The diagnostic agreement between two readers was substantial for both CT (κ = 0.747) and ZTE (κ = 0.704 and 0.727 for ZTE without postprocessing and ZTE with postprocessing) but fair for T1 FSE (κ = 0.279). ICCs for the erosions sum scores between two readers for all four images were presented in Table 4.Discussion
This is the first study to explore the feasibility of ZTE in the evaluation of bone structural lesions in SIJ. Both ZTE images with and without postprocessing were superior to conventional T1 FSE in sensitivity, specificity, and accuracy for detection of SIJ erosions on the articular surfaces of sacrum and ilium that constitute SIJs. The agreement between ZTE/post-processed ZTE and the current gold standard modality (CT) was good for detection of erosions. ZTE also represented better performance than T1 FSE in terms of inter-reader reliability. These findings suggest that ZTE could provide a better and more reliable detection of erosions in SIJ, meeting the clinical standard for assessment of erosions without ionizing radiation; and the postprocessing for ZTE may not influence its detection abilities but still slightly improve accuracy and reliability. The high contrast between bone and other tissues by direct acquisition of bone signal using ZTE, and thinner image slices of ZTE leading to high resolution may contribute to its superiority over conventional T1 FSE in erosion depiction. Further researches with larger sample sizes are needed to validate the findings of this study. In addition, the performance of ZTE for the detection of other chronic bone structural lesions in axial axSpA needs to be further studied to determine if ZTE has the potential to meet CT standards and be used as a clinical CT substitution in some cases.Conclusion
ZTE showed higher accuracy and reliability of SIJ erosion detection compared with conventional T1 FSE in patients with suspected axSpA regardless of postprocessing. Thus, ZTE may be a valuable supplement to routine a clinical MRI protocol for axSpA, which may improve diagnostic accuracy in the assessment of bone erosions.Acknowledgements
We thank for the support of the National Natural Science Foundation of China (NSFC) (No. 31630025 and 81930045).References
1. Weber U, Lambert R G, Østergaard M, et al. The diagnostic utility of magnetic resonance imaging in spondylarthritis: an international multicenter evaluation of one hundred eighty-seven subjects. Arthritis Rheum. 2010; 62(10): 3048-58.
2. Arnbak B, Grethe Jurik A, Hørslev-Petersen K, et al. Associations Between Spondyloarthritis Features and Magnetic Resonance Imaging Findings: A Cross-Sectional Analysis of 1,020 Patients With Persistent Low Back Pain. Arthritis Rheumatol. 2016; 68(4): 892-900.
3. Breighner R E, Endo Y, Konin G P, et al. Technical Developments: Zero Echo Time Imaging of the Shoulder: Enhanced Osseous Detail by Using MR Imaging. Radiology. 2018; 286(3): 960-966.
4. Breighner R E, Bogner E A, Lee S C, et al. Evaluation of Osseous Morphology of the Hip Using Zero Echo Time Magnetic Resonance Imaging. Am J Sports Med. 2019; 47(14): 3460-3468.
5. Xie R, Sun D, Morelli J N, et al. Recognition of sacroiliac joint structural lesions: Comparison of volumetric interpolated breath-hold examination (VIBE) sequences with different slice thicknesses to T1-weighted turbo-echo. Eur J Radiol. 2020; 124: 108849.
6. Diekhoff T, Hermann K G, Greese J, et al. Comparison of MRI with radiography for detecting structural lesions of the sacroiliac joint using CT as standard of reference: results from the SIMACT study. Ann Rheum Dis. 2017; 76(9): 1502-1508.
Figures