4066
Pilot contrast-free MRI reveals significantly impaired calf skeletal muscle perfusion in diabetes with incompressible peripheral arteries1Washington University in St. Louis, St. Louis, MO, United States, 2MR Innovations Inc, Bingham Farms, MI, United States, 3Wayne State University, Detroit, MI, United States
Synopsis
The purpose of this study is to investigate whether individuals with diabetes mellitus and incompressible arteries will have lower skeletal muscle microcirculation during a moderate isometric exercise. Healthy volunteers, diabetes with normal artery, and diabetes with incompressible arteries underwent MR angiography and calcification imaging, and skeletal muscle microcirculation imaging at rest and during an isometric contraction exercise. Significantly lower perfusion reserve and its association with higher ABI were observed in diabetes with incompressible arteries. Despite lack of apparent arterial stenosis, calcification can be readily visualized in 2 patients.
Purpose
Patients with diabetes mellitus (DM) are more likely to have below-the-knee (BTK) tibial peripheral arterial disease with densely calcified recalcitrant atherosclerotic lesions.1 Compared to patients with no or mild peripheral calcification, patients with severe peripheral arterial calcification had significantly higher rates of amputation, cardiac mortality, and significant morbidity and disability. Calcification develops in arterial intima and media, which results in decreased arterial compliance (incompressible arteries) and surrounding tissue perfusion. The purpose of this study is to investigate whether individuals with DM and incompressible arteries will have lower skeletal muscle microcirculation during a moderate isometric exercise compared to individuals with DM and normal arteries, as well as individuals without DM.Methods
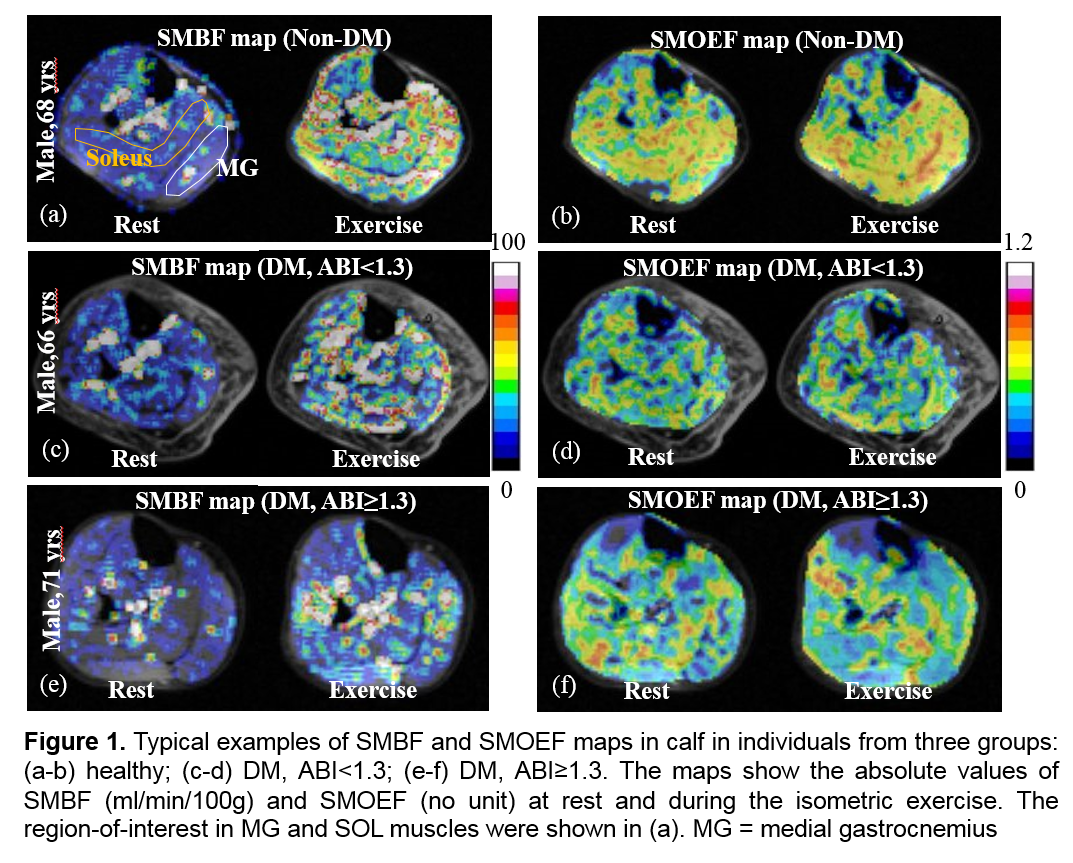
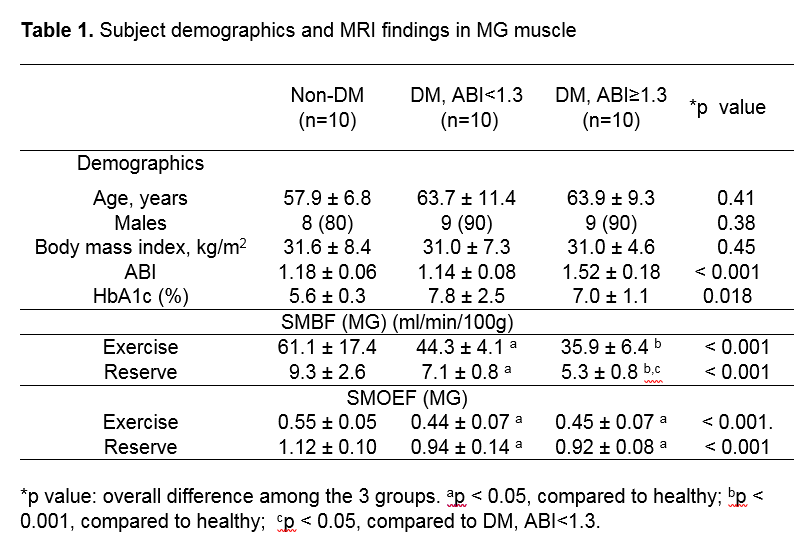
This study protocol was approved by the Human Research Protection Office at the local institute and all subjects provided written informed consent prior to participation. Thirty subjects were recruited with matched age, sex, and body mass index (BMI) and had ankle-brachial-index (ABI) to determine the stiffness of the peripheral arteries. They were separated into three groups: (1) 10 subjects with DM and ABI ≥ 1.3 (DM, ABI ≥ 1.3), (2) 10 subjects with DM and ABI between 0.91 and 1.3 (DM, ABI<1.3) and (3) 10 healthy subjects without DM (Healthy).The MRI system was a 3 T Prisma system (Siemens Healthcare, Erlangen, Germany).The measurements for assessing microcirculation was performed in calf muscle, at rest and during an isometric plantarflexion contraction within the MRI bore.2 First, a contrast-free arterial spin labeling method was applied to obtain skeletal muscle blood flow (SMBF) data (2). The SMBF reserves were calculated from the ratio of exercise SMBF divided by the resting SMBF. Second, another contrast-free MR technique using a 2-dimensional, triple-echo, asymmetric spin-echo sequence was applied to measure skeletal muscle (SMOEF) with the magnetic susceptibility effect of deoxyhemoglobin (2).
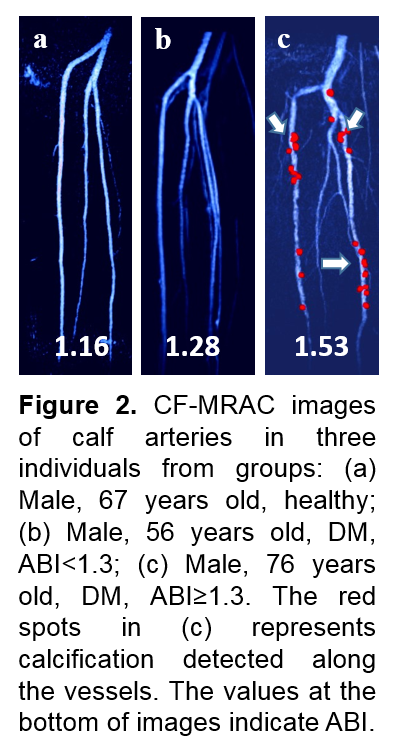
Nine subjects underwent a newly developed contrast-free 3D MR angiography and calcification imaging (CF-MRCA) at rest. This technique allows simultaneous data collection for angiography, phase images, and susceptibility weighted imaging mapping (SWIM) with only approximately 6-min scan of the calf arteries and an isotropic image resolution of 0.9 x 0.9 x 0.9 mm3. The sequence is a single 3D excitation interleaved rephrased/dephased 3-echo gradient-echo sequence (TE1/TE2/TE3 = 2.5/17.5/17.5 msec). By subtracting the flow-dephased images at TE3 from the flow-rephased images at TE2 with the same echo time, a MR angiogram (MRA) can be created. The SWIM data generated from the phase image of the short echo TE1 can be used to assess substances with high susceptibility values such as calcification and hemorrhage.
The source images from both SMBF and SMOEF measurements were processed using custom software to create respective maps. Two regions-of-interest (ROIs) around the soleus and medial gastrocnemius (MG) muscle were drawn on both maps to obtain mean SMBF and SMOEF values. The SMBF and SMOEF reserves were calculated as the ratio of exercise/rest from the ROI data. CF-MRAC was only assessed by visual inspection as presence or absence of stenosis and calcification.
Results
Table shows the demographics of the subjects and MRI findings. All exercise SMBF, SMOEF, and their reserve values were lower in both DM groups than those in the healthy group. Figure 1 shows the examples of SMBF and SMOEF maps in subjects from all three groups. For the comparison between two DM groups, the SMBF reserve in MG was significantly lower in the DM, ABI≥1.3 group than in the DM, ABI<1.3 group (p = .02). This difference remained significant after the adjustment for smoking, PN, and foot ulcers (p = .03). No differences were observed for all SMOEF indexes between the two DM groups. The exercise SMBF in both MG and soleus was moderately and negatively correlated with ABI (r = -0.53 for MG and -0.4 for soleus). This correlation was even stronger for the SMBF reserve in the MG (r = -0.62), but not in soleus.None of 9 subjects who had CF-MRAC showed apparent arterial stenosis in their calf arteries by visual inspection. Only the two subjects in the DM, ABI≥1.3 group had evidence of arterial calcification (Figure 2).
Conclusion
This study provides the first evidence demonstrating the potential impact of incompressible and/or calcified tibial arteries (as demonstrated on conventional ABI measurements) on the severity of local skeletal muscle microcirculation in the setting of DM. These findings may provide future better strategies for accurate diagnosis, risk stratification, and therapeutic interventions in individuals who are traditionally at higher risk for limb amputation and disease morbidity.Acknowledgements
This study was supported in part by research grants from National Institute of Health R21AR065672, R01DK105322, and R03EB028415. The authors would like to thank Darrah Snozek and Katherine Love for coordinating the recruitment of participants.References
1. Abbott, RD., Brand FN, Kannel WB. Epidemiology of some peripheral arterial findings in diabetic men and women: experiences from the Framingham Study. Am J Med. 1990; 88: 376-381.
2. Zheng J, An H, Coggan AR, Zhang X, Bashir A, Muccigrosso, D, Peterson LR, Gropler RJ. Noncontrast skeletal muscle oximetry. Magn Reson Med, 2014; 71: 318-325.
Figures
Table