4065
Discussion the Value of ADC in Bone Contusions and Bone Marrow Lesions in Osteoarthritis of Knee Joint1Affiliated Hospital of Guizhou Medical University, Guiyang, China, 2592159673@qq.com, Guiyang, China, 3GE Healthcare, MR Research China, Beijing, China
Synopsis
The current study aims to investigate the application value of ADC in Bone Contusions and Bone Marrow Lesions in Osteoarthritis of Knee Joint. It was concluded that ADC value has the potential value to differentiate the two kinds of lesions.
Introduction
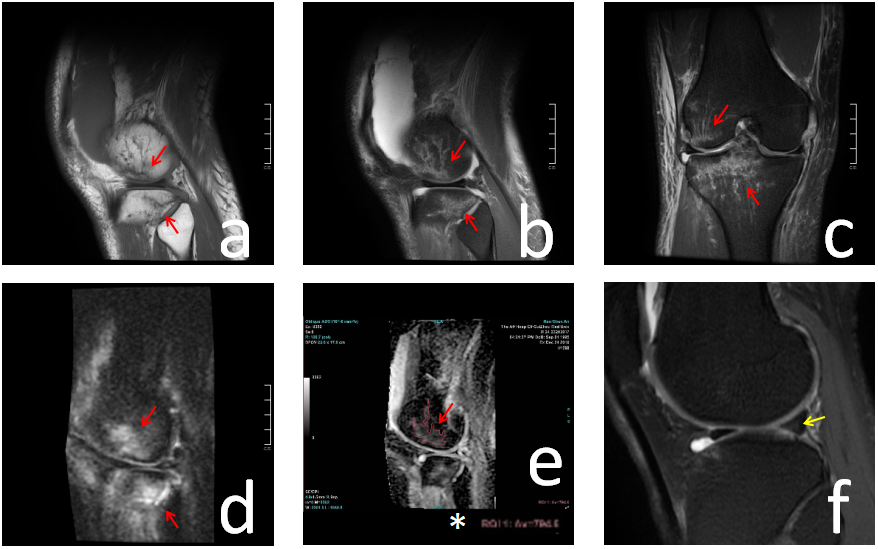
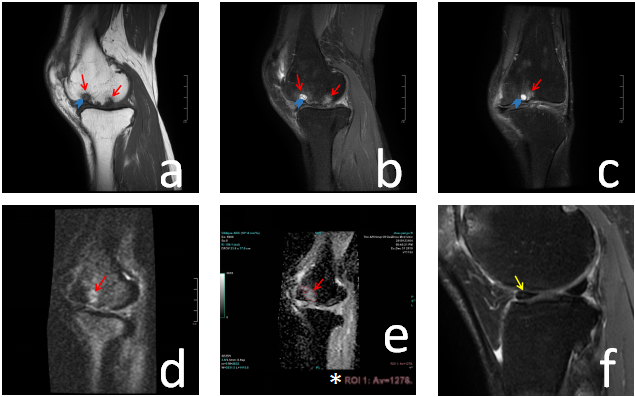
Traumas of the knee joint often result in bone fractures and contusions, meniscus injury and soft tissue injury [1]. OAis a kind of bone and joint disease caused by articular cartilage degeneration[2]. Previous studies[3] have found that the pathological factors of bone contusions is mainly bone marrow edema and cell content displacement, while bone marrow lesions in OA is mainly multiple non-specific histological abnormalities[4], including bone marrow necrosis, bone marrow fibrosis and trabecular bone remodeling. The area of actual bone marrow edema only accounts for 4% of the abnormal MR signal area. Although their pathological changes are very different, they both show high signal on DWI[5, 6].Therefore, in this study, ADC values of bone contusions and bone marrow lesions in OA of the knee joint were measured and their statistical differences were analyzed, so as to further explore their differences in imaging.Materials and methods
This study was approved by the institutional review board, and written informed consent was obtained from all patients. From September 2019 to January 2020, 44 patients (male=13, female=31, age 58.9±6.7 years) with OA and 17 patients with bone contusions (male=12, female=5, age 41.4±11.6 years) were enrolled prospectively.All subjects underwent preoperative T1-FSE, PD-TSE FS, DWI on a 3.0 T MRI scanner(Discovery MR 750W, GE Healthcare, Waukesha, USA). And the data were sent to the workstation after being obtained for post-processing. The ADC values of the lesions with definite manifestations were measured and recorded. 17 knees of the bone contusion group were scanned effectively, and 36 regions of interest (ROIs) were measured and calculated. In the OA group, 31 knees were scanned effectively, and 66 ROIs were measured and calculated. P < 0.05 was considered as statistically significant. Independent sample t tests was carried out to compare the difference of ADC values.
Results
The average ADC value was (0.93 ± 0.22) × 10-3mm2/S of the bone contusion group, and (1.14 ± 0.24) ×10-3mm2/S of bone marrow lesions of the OA group. K-S test showed that data were normal. By independent sample t test, the difference between the groups was statistically significant (t = 4.29, P = 0.00).Discussion
This study found that the ADC value of bone marrow lesions in OA was higher than that of bone contusions, which may be related to the following three causes. Firstly, the development of lesions is different. The direct cause of bone contusions is sudden violence, which usually lasts for a short time. Strict immobilization is advocated during the treatment, so the lesions will recover soon[7]. However, OA is a kind of chronic disease with a long course of disease[8]. It is difficult to maintain strict immobilization during the treatment, thus cartilage and subchondral bone injury is often difficult to be inhibited. Secondly, the pathological components of the lesions are different. Although their MRI manifestations are similar, the edema area of the bone marrow lesions in OA is actually very small, which is mainly multiple non-specific histological abnormalities[4], including bone marrow necrosis, bone marrow fibrosis and trabecular bone remodeling, but the pathological changes of bone contusions are mainly bone marrow edema and cell content displacement. Their different pathological bases may be one of the causes for the difference in ADC values. Thirdly, there are cystic lesions in or around bone marrow lesions of OA. In this study, 28 patients of the OA group were combined with cystic degeneration (accounting for 63.6% of the OA group). Although the cystic part was avoided in the measurement of ADC values as far as possible, some small cystic changes were still difficult to identify and exclude, which may be contained in ROIs, resulting in the increase in ADC value.Conclusions
The ADC value of bone marrow lesions in OA is higher than that in bone contusions, with a statistical difference. ADC value has the potential value to differentiate the two kinds of lesions.Acknowledgements
Thanks to my mentor, classmates, and everyone who helped me in the research process.
References
[1] Lal N R , Jamadar D A , Doi K , et al. Evaluation of bone contusions with fat-saturated fast spin-echo proton-density magnetic resonance imaging.[J]. Canadian Association of Radiologists Journal, 2000, 51(3):182-185.
[2] Tamm A , Lamson L , Lintrop M , et al. Knee injury and osteoarthritis outcome score (koos) in a 34-54 old population with early stages of knee osteoarthritis: a follow-up study[C]// Congress of the European-federation-for-research-in-rehabilitation. 2007.
[3] Escalas F, Curell R. Occult posttraumatic bone injury[J]. Knee Surgery Sports Traumatology Arthroscopy, 1994, 2(3):147-149.
[4] Zanetti M, Bruder E, Romero J , et al. Bone marrow edema pattern in osteoarthritic knees: correlation between MR imaging and histologic findings.[J]. Radiology, 2000, 215(3):835.
[5] Lal, Nirish, R, et al. Evaluation of bone contusions with fat-saturated fast spin-echo proton-density magnetic resonance imaging.[J]. Canadian Association of Radiologists Journal, 2000.
[6] Klengel A, Stumpp P, Klengel S, et al. Detection of Traumatic Bone Marrow Lesions after Knee Trauma: Comparison of ADC Maps Derived from Diffusion-weighted Imaging with Standard Fat-saturated Proton Density–weighted Turbo Spin-Echo Sequences[J]. Radiology, 2016:160306.
[7] Boks S S , Vroegindeweij D , Koes B W , et al. MRI follow-up of posttraumatic bone bruises of the knee in general practice.[J]. Ajr Am J Roentgenol, 2007, 189(3):556-562.
[8] Spector T D , Dacre J E , Harris P A , et al. Radiological progression of osteoarthritis: an 11 year follow up study of the knee.[J]. Annals of the Rheumatic Diseases, 1992, 51(10):1107-1110.
Figures