4012
Comparison of Diffusion Tractography and fMRI-based Targeting for MRgFUS Treatment of Essential Tremor1Electrical Engineering, Stanford University, Stanford, CA, United States, 2Biophysics, Stanford University, Stanford, CA, United States, 3Bioengineering, Stanford University, Stanford, CA, United States, 4Radiology, Stanford University, Stanford, CA, United States
Synopsis
Probabilistic diffusion tractography and fMRI are two alternative methods for targeting the ventral intermediate nucleus of the thalamus in patients with essential tremor (ET) for treatment with transcranial magnetic resonance imaging-guided focused ultrasound (tcMRgFUS). In this study, three ET subjects underwent MRgFUS thalamotomy with traditional targeting using anatomic landmarks. Tractography and fMRI targeting were compared retrospectively to determine how they relate to one another and to the targets selected by the surgeon. Two of the three subjects showed a consistent spatial relationship between fMRI, tractography and anatomical targets.
Introduction
Transcranial magnetic resonance imaging-guided focused ultrasound (tcMRgFUS) thalamotomy is a non-invasive surgical technique used to treat essential tremor (ET). The treatment aims to lesion the ventral intermediate nucleus (Vim) of the thalamus to suppress tremor symptoms. Since the Vim cannot be directly visualized on a structural MRI, the most common targeting method is based on population-based coordinates relative to the anterior commissure-posterior commissure (AC-PC) line1. However, this does not account for anatomical or functional variability between patients and lacks specificity of the hand-motor representation within the Vim. Here, we retrospectively compare two alternative targeting methods seeking to overcome these limitations: probabilistic diffusion tractography2,3 and functional magnetic resonance imaging (fMRI).Methods
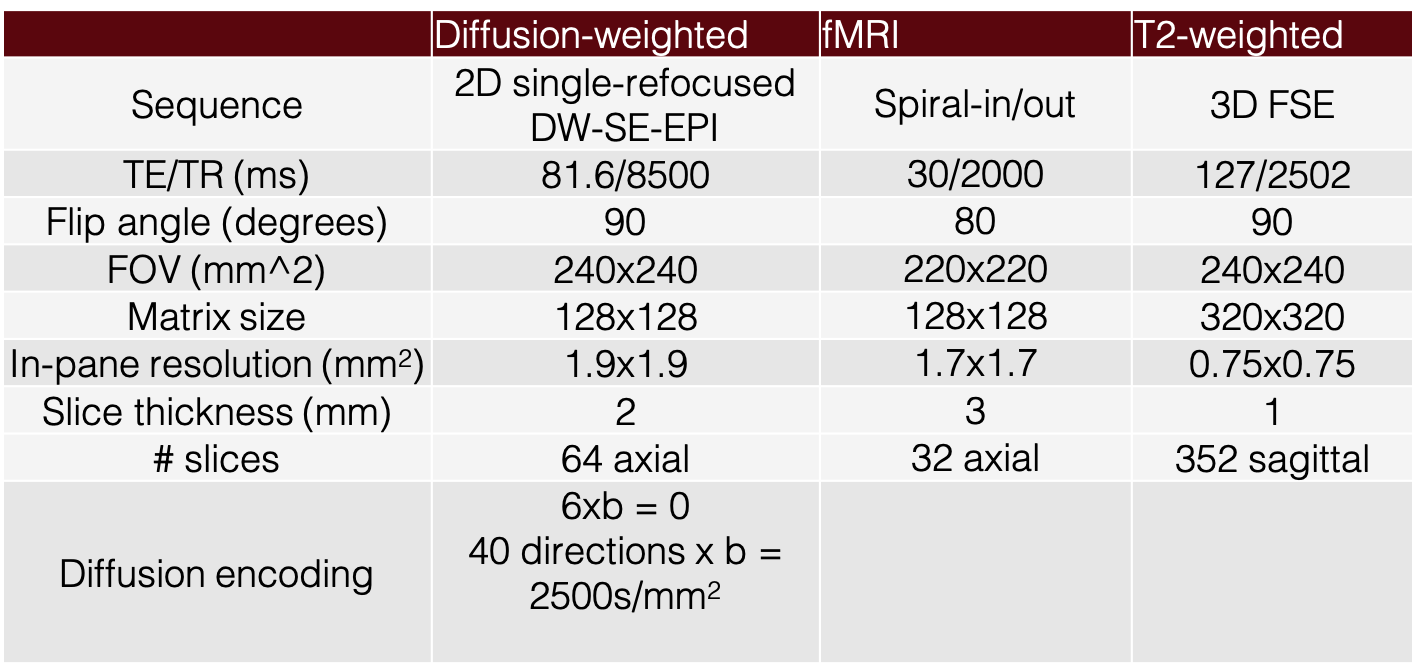
Three patients with medication-refractory ET were treated with tcMRgFUS thalamotomy targeting the Vim. Lesioning was performed using a 3T GE Signa Premier MRI system (GE Healthcare, Milwaukee, Wisconsin) and a clinical system for focused ultrasound surgery (ExAblate Neuro 4000, InSightec, Haifa, Israel). Traditional population-based targeting was used for the procedure and the location of each imaging target was compared retrospectively. In this study, four different locations were compared: probabilistic tractography target, fMRI target, traditional target and induced lesion.MRI scans were performed on the same clinical 3T MRI system equipped with a 48-channel head coil. Data acquisition included whole-brain diffusion, fMRI and structural MRI (Table 1). Diffusion-weighted MRI and fMRI data were acquired pre-treatment using a 2D single-refocused diffusion-weighted spin-echo echo-planar imaging sequence and a spiral-in/out imaging sequence respectively, while T2-weighted structural data was acquired both pre- and post-treatment using a 3D fast spin-echo sequence. A motor planning task was used for the fMRI acquisition in which the subjects pressed specific buttons in response to alternating numbers displayed on a screen (block design; 15s task/15s rest; 24 blocks).
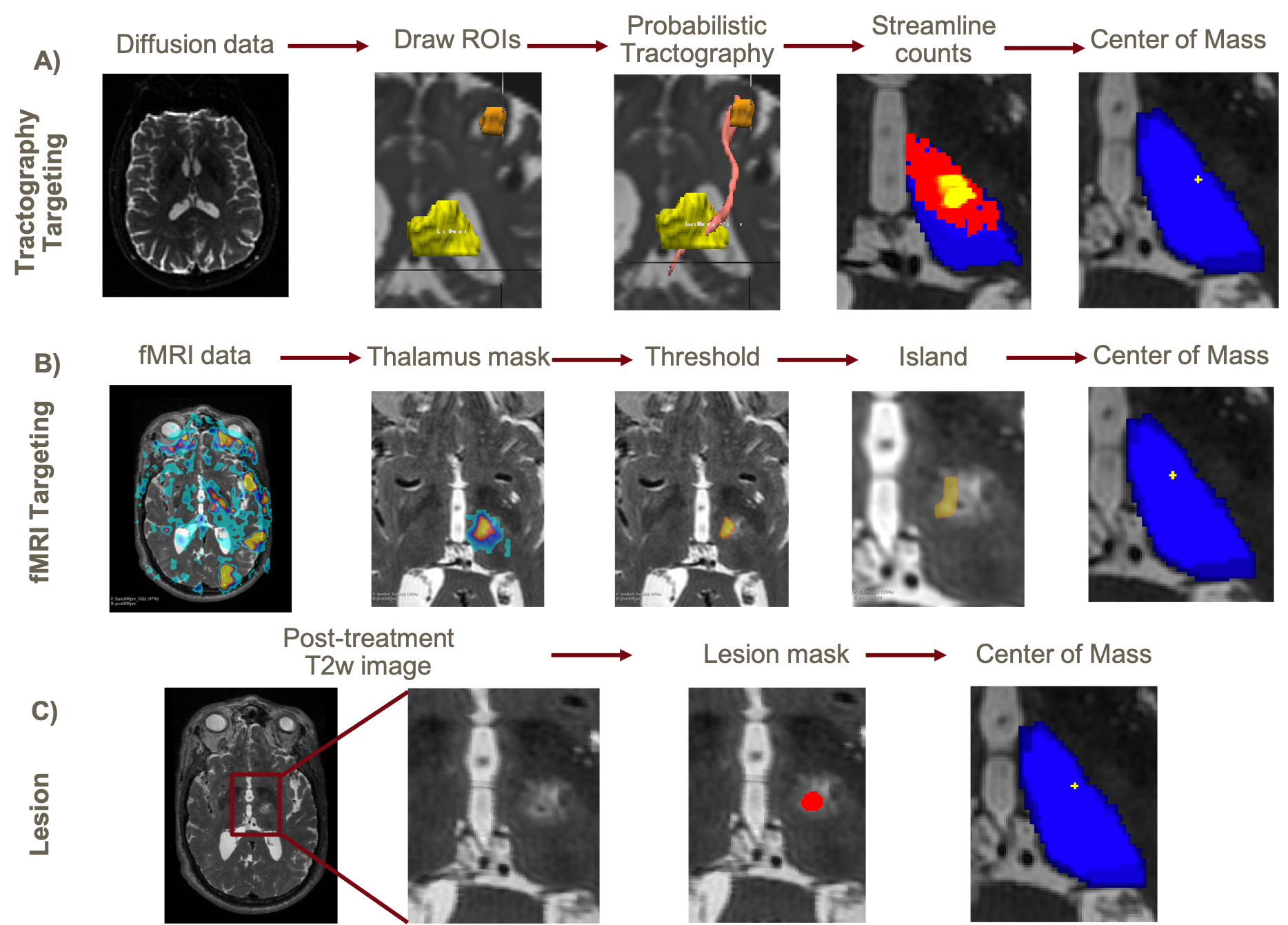
Probabilistic tractography analysis was performed using FMRIB Software Library4 (FSL) with the thalamus as the “seed” and the ipsilateral hand-knob region of the motor cortex as the “target”. The “seed” and “target” region of interests (ROIs) were hand-drawn by a radiologist (Figure 1A). The number of streamlines connecting each thalamic voxel within the targeted region was found and the MRgFUS target was defined as the center of mass (COM) of the streamline counts.
To produce the fMRI target, an MNI template was registered to the structural data acquired in the same session and a MNI thalamic atlas (DISTAL)5 was used to mask out the “non-thalamic” voxels in the fMRI activation map (Figure 1B). The remaining voxels were thresholded at p < 3e-4. The fMRI target was defined as the COM of the largest contiguous island that survived the threshold.
An ROI of the lesion was hand-drawn based on the T2-weighted post-treatment scan taken the day of the treatment (Figure 1C). The ROI was defined as the necrotic core and the region of cytotoxic edema that surrounds it6. Voxel magnitudes within the ROI were inverted to give the most hypointense voxels the largest weight and the lesion location was defined as the COM of the ROI.
To compare locations of different imaging targets, the post-treatment, diffusion and fMRI data were co-registered to the pre-treatment T2-weighted image.
Results and Discussion
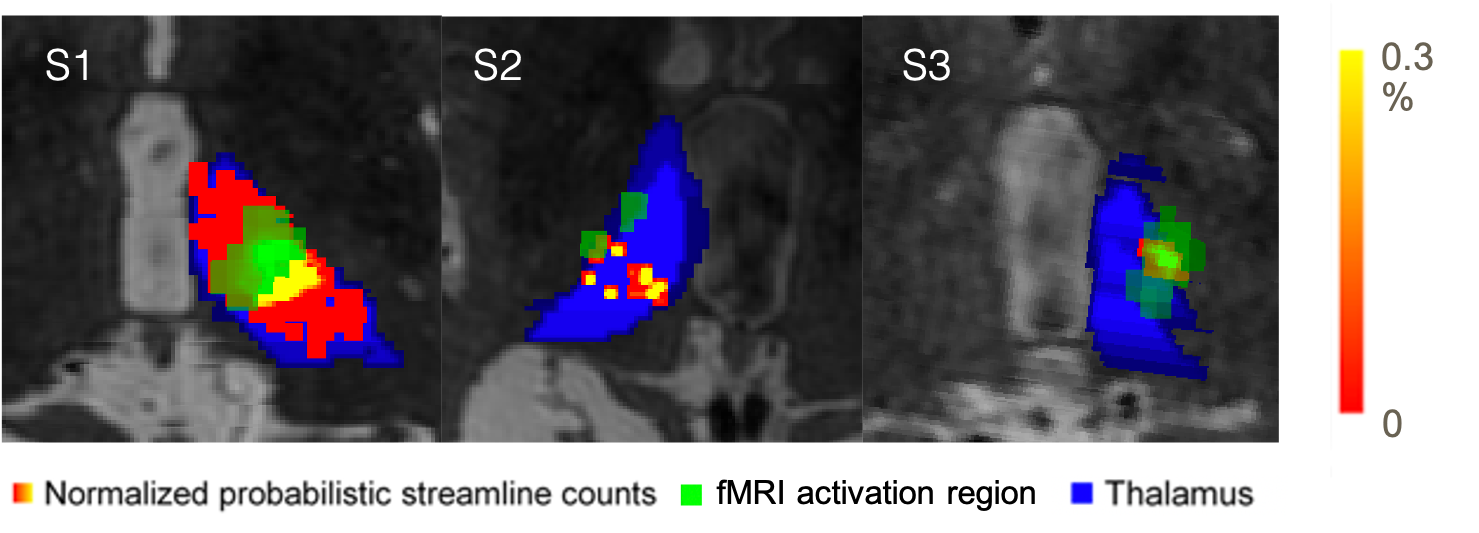
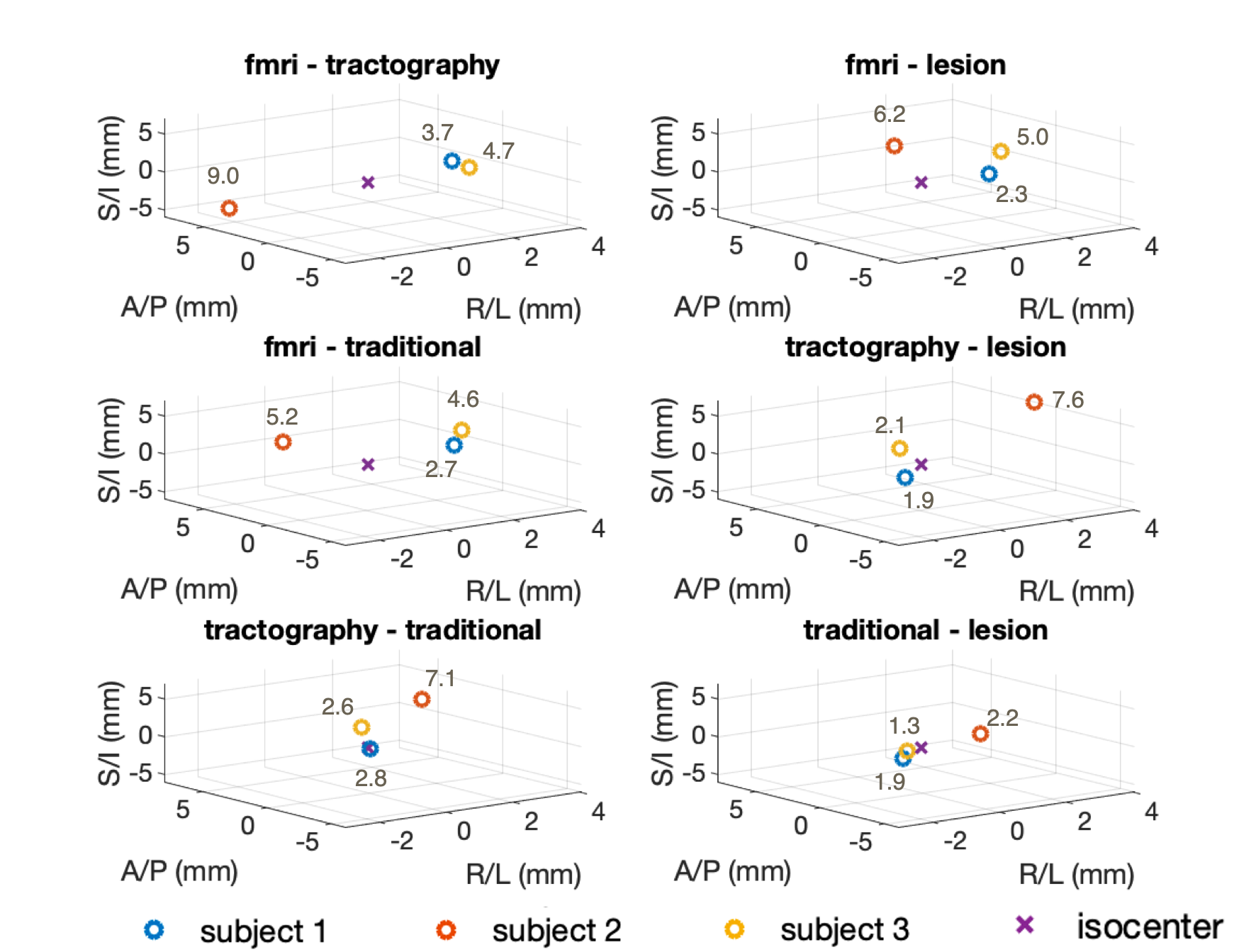
Figure 2 shows the normalized probabilistic streamline count map and thresholded fMRI activation region within the treated thalamus overlaid on the pre-treatment T2-weighted images. There is a good overlap between the tractography and fMRI targets for subjects 1 and 3. The results from subject 2 were unexpected as there was no dominant island of activation or streamline counts within the thalamus. Therefore, the COM calculation as a potential target location must be treated with skepticism. Subject 2's result could be due to significant motion during fMRI scans and difficulties in drawing the “target” ROI for probabilistic tractography due to abnormalities in the structural scans.Figure 3 shows the distances between the different target locations for each subject in RAS coordinates. Subjects 1 and 3 have similar results across all comparisons. The fMRI target was about [3 mm, 2 mm, -1 mm] to the tractography target. The fMRI and tractography targets were about [3 mm, 1 mm, 1 mm] and [-0.5 mm, -1 mm, 2 mm] to the traditional target respectively. Distances in the R/L direction for subject 2 were inverted since the treatment was on the right while treatment for subjects 1 and 3 were on the left. Based on physician assessments within 1-year post-treatment, subject 1 had mild improvement after treatment, subject 2 benefitted, but with significant side effects while subject 3 had excellent results.
Conclusion
We retrospectively compared two alternative targeting methods for tcMRgFUS thalamotomy: probabilistic tractography and fMRI. Preliminary results indicate a consistent spatial location for the relative location of the targets to i) each other, ii) the traditional anatomical targets and iii) lesion locations in two of the three subjects. Future directions include collecting more data with pre- and post-treatment tremor scores to establish the significance and relevance of both functional and tractography-based targets for the treatment. More work will be needed to assess whether either of these targets, or some function of them, will yield a superior starting point for ultrasound ablation of the Vim than the current landmark-based approach.Acknowledgements
NIH P41EB015891, Focused Ultrasound Foundation, GE Healthcare, Knight-Hennessy Scholars ProgramReferences
1. Ghanouni, P., Pauly, K.B., Elias, W.J., Henderson, J., Sheehan, J., Monteith, S., et al., 2015. Transcranial MRI-guided focused ultrasound: a review of the technologic and neurologic applications. Am. J. Roentgenol. 205 (1), 150–159.
2. Tian, Q., et al., 2018. Diffusion MRI tractography for improved transcranial MRI-guided focused ultrasound thalamotomy targeting for essential tremor. Neuroimage: Clinical, 19, 572–580.M.W.
3. Thaler C, Tian Q, Wintermark M, Ghanouni P, Halpern CH, Henderson JM, Airan RD, Zeineh M, Pauly KB, McNab JA. White matter fibre tract changes in patients treated with MR imaging-guided focused ultrasound are associated with lesion location and clinical outcome. Electronic Poster. International Society for Magnetic Resonance in Medicine Annual Scientific Meeting: Paris, France, June 2018.
4. Woolrich, S. Jbabdi, B. Patenaude, M. Chappell, S. Makni, T. Behrens, C. Beckmann, M. Jenkinson, S.M. Smith. Bayesian analysis of neuroimaging data in FSL. NeuroImage, 45:S173-86, 2009
5. Ewert, S., Plettig, P., Li, N., Chakravarty, M.M., Collins, D.L., Herrington, T.M., Kühn, A.A., Horn, A., 2018. Toward defining deep brain stimulation targets in MNI space: A subcortical atlas based on multimodal MRI, histology and structural connectivity. NeuroImage 170, 271–282.
6. Keil V.C., et al., MRI follow-up after magnetic resonance-guided focused ultrasound for non-invasive thalamotomy: the neuroradiologist's perspective. Neuroradiology. 2020 Sep;62(9):1111-1122. doi: 10.1007/s00234-020-02433-9. Epub 2020 May 3. PMID: 32363482; PMCID: PMC7410861.
Figures