4011
MR guided Focused Ultrasound as a Non-Invasive Surgical Treatment of Lung Cancer
Jaime Mata1, Lauren Powlovich2, David Moore2, and Linda Martin1
1University of Virginia, Charlottesville, VA, United States, 2Focused Ultrasound Foundation, Charlottesville, VA, United States
1University of Virginia, Charlottesville, VA, United States, 2Focused Ultrasound Foundation, Charlottesville, VA, United States
Synopsis
Malignant lung cancer carries a poor prognosis with a 5-year survival rate of about 18%. This new method proposes an innovative minimally invasive procedure for the transcutaneous ablation of lung tumor masses with complete removal or significant debulking of the masses. This new procedure could increase lung cancer survival rates and at the same time decrease morbidity and side effects associated with current treatment therapies. It will also provide a viable treatment for a large group of patients that cannot tolerate resection surgery, radiotherapy and chemotherapy, or who have had prior radiation and cannot have additional radiation to that region.
Introduction
Malignant lung cancer carries a poor prognosis (median survival of about 10 months) with rare cases of complete cure and a 5-year survival rate of about 18 percent. Surgical resection therapy was shown to have the greatest impact on survival and consists of removing the entire lobe or segment of the affected region of the lung, but unfortunately the majority of the lung cancer patients (about 60-70%) do not qualify for or cannot tolerate surgery. This method proposes an innovative minimally invasive procedure for the transcutaneous ablation of lung tumor masses with complete removal or significant debulking of the masses, without the use of traditional open lung resection surgery. This technique does not require flooding of the lung in order to get an acoustic window for the Focused Ultrasound (FUS), which can pose serious immediate and long term risks for the patient (i.e. pneumonia, sepsis, among other complications).Materials & Methods
Two Yucatan mini pigs (~30Kg) had both main bronchi selectively intubated, and while the left lung was mechanically ventilated, the right lung was purposely collapsed, followed by a controlled right hydrothorax in the chest cavity with saline in order to create an acoustic window for the FUS beam. At the end of the MR guided Focused Ultrasound (MRgFUS) ablation, the saline was drained in a method identical to the drainage of a clinical pleural effusion. Animal #1 received six transcutaneous MRgFUS ablations of the right lung, in six different locations. Each location received a different amount of acoustic power in order to determine the optimal power with minimal side effects (i.e. skin burns). Animal #2 received two transcutaneous MRgFUS ablations on two large areas of the upper lobe of the right lung. An intercostal approach was used in order to target the transcutaneous beam without distortion and attenuation caused by the ribs. One week after the ablation, each animal received a MRI of the lung to assess the success of the ablation; animals were then euthanized and a histopathological examination of the lungs was performed to correlate with the results of the MRI.Results
Ablations were done successfully on both animals. The locations and sizes of the ablations as determined by post treatment MRI and gross histology, correlated well with the initial target locations and the power doses applied (Figs 1-2). The escalation test done on animal #1, was very useful to determine the power and the duration of the treatments. This information was used on animal #2 with immediate success (Figs 1-2) but further refinement of the doses and treatment times is necessary to avoid skin lesions. This should be accomplished in the near future on new animal studies. Immediately after MRgFUS treatment, the saline in the chest cavity was drained with only a small volume of ~10% (~60cc) remaining inside the cavity. Both animals recovered very well from the MRgFUS treatment with no significant side-effects besides a skin lesion on animal #2 at the place where the transducer was located.Discussion
These preliminary results are very encouraging. This new procedure could increase lung cancer survival rates and at the same time decrease morbidity and side effects associated with current treatment therapies like radiosurgery and chemotherapy, since it will permit nonsurgical tumor ablation or tumor debulking. It will also provide a viable treatment for a large group of patients that cannot tolerate resection surgery, radiotherapy and chemotherapy, or who have had prior radiation and cannot have additional radiation to that region. For this large segment of the patient population, palliative care, not full treatment, was traditionally the therapy of choice. The proposed procedure may create new hope for these patients and improved palliation for others.Conclusion
Non-invasive ablation and debulking of lung tumors seems possible with the novel method proposed using MRgFUS. We successfully ablated lung tissue deep in the lung without incisions, reducing the risk for infection and other complications.Acknowledgements
Supported in part by a grant from the Focused Ultrasound Foundation.References
No reference found.Figures
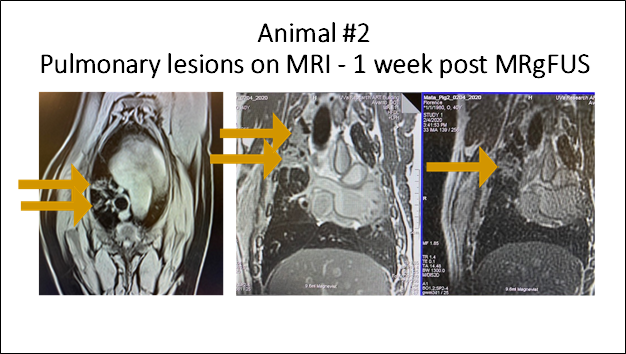
Figure 1 - Multiple
MR images taken one-week post MRgFUS treatment of animal #2. Pulmonary lesions produced by MRgFUS marked
with arrows.
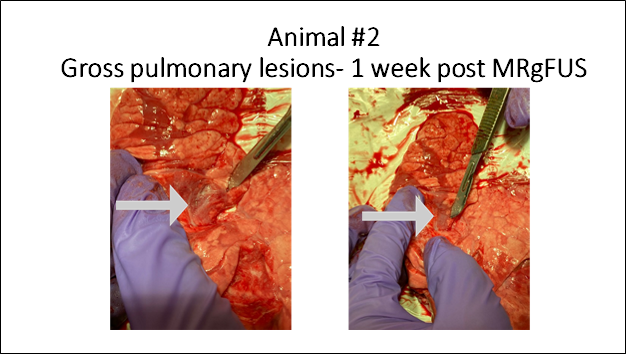
Figure 2 - Gross
pulmonary lesions marked with arrow. These lesions correlate with the lesions
marked on the MR images of Figure 1.