3992
Investigating the Effect of Positive Airways Pressure on Venous Oxygenation in Sickle Cell Anemia with Quantitative Susceptibility Mapping1Department of Medical Physics and Biomedical Engineering, University College London, London, United Kingdom, 2Imaging and Biophysics, Developmental Neurosciences, UCL Great Ormond Street Institute of Child Health, London, United Kingdom
Synopsis
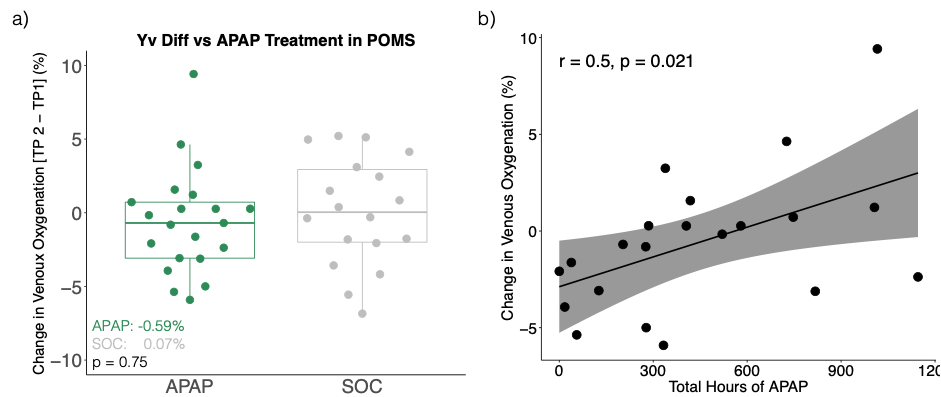
In 88 sickle cell anaemia (SCA) patients and 30 healthy controls, quantitative susceptibility mapping (QSM) showed significantly lower venous oxygen saturation (Yv) in the superior sagittal sinus of SCA patients. SCA subjects with silent cerebral infarcts (SCI) showed significantly lower Yv relative to those without SCI. 39 SCA subjects participated in a clinical study investigating the effect of auto-adjusting positive airways pressure (APAP) over a period of six months. No significant Yv differences were observed between 21 patients receiving APAP and 18 receiving standard care. In the APAP group, treatment compliance was positively correlated with increases in Yv.
Introduction
Sickle Cell Anaemia (SCA) is an inherited red blood cell disorder, characterized by cerebral vasculopathy, haemolytic anaemia and cognitive impairment. Silent cerebral infarcts (SCI) consistent with small vessel disease are the most common neurologic injury in SCA and their presence is used as an indicator of stroke risk. Reduced venous oxygenation (Yv) (due to compromised oxygen delivery) has been suggested as a more robust indicator of increased stroke risk.Studies investigating Yv in SCA relative to healthy controls (HC) have found contrasting results, perhaps caused by differences in calibration models used to convert MRI measures to Yv1,2. Quantitative Susceptibility Mapping (QSM) shows promise for measuring Yv in SCA as the magnetic susceptibility (χ) of venous blood depends linearly upon oxygen saturation3 and previous studies showed no difference in the χ of sickle and healthy red blood cells4. Here, we used QSM to measure Yv in the superior sagittal sinus (SSS) of SCA subjects and HC.
SCA and HC subjects were recruited from two clinical studies: the Sleep and Asthma Cohort (SAC) and Prevention of Morbidity in SCA (POMS)5,6. In POMS, SCA subjects were divided between two groups: i) the treatment group received nighttime Auto-Adjusting Positive Airways Pressure (APAP) over six months and ii) the control group received standard of care (SOC) treatment. APAP aims to prevent low nighttime oxygen levels and reduce red blood cell sickling associated with complications in SCA. Therefore we might expect it to boost arterial oxygen content and Yv. SAC subjects underwent a single MRI examination whilst POMS participants had scans before and after the treatment period with multiple blood draws performed throughout.
We aimed to investigate the effect of 1) SCA upon Yv and examine relationships with the presence of silent cerebral infarcts (SCI) and cognitive performance and 2) APAP treatment upon Yv in SCA; and treatment compliance upon Yv changes.
Methods
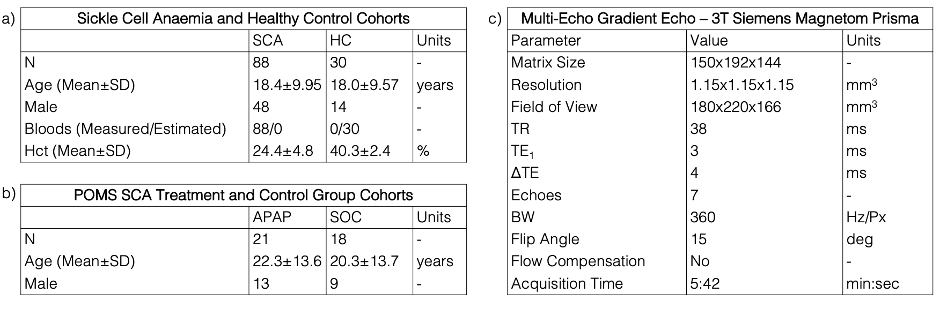
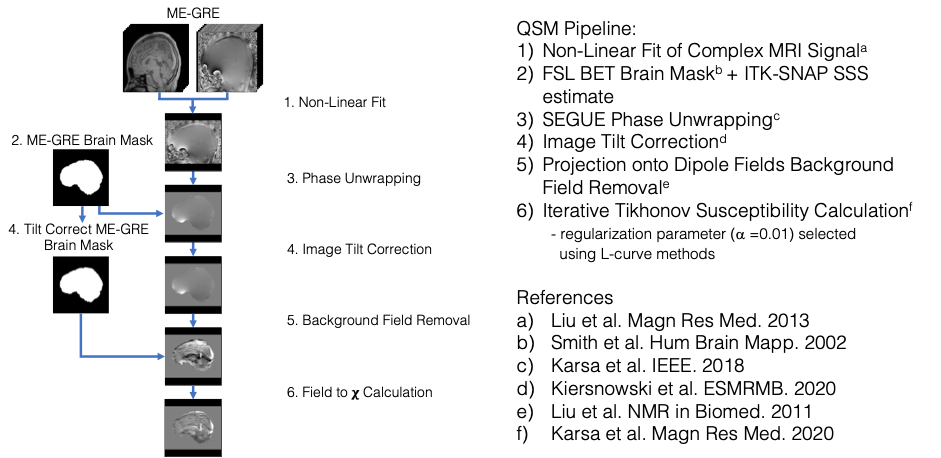
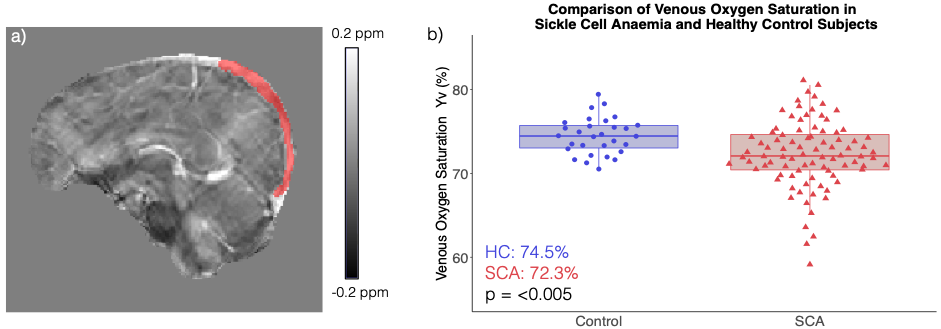
All participants underwent brain MRI on a 3T Siemens Magnetom Prisma. The subject cohort is described in Figure 1a. QSM was calculated from the multi-echo gradient-echo sequence described in Figure 1b. Figure 2 shows the optimised QSM pipeline.A single SSS region of interest (ROI) was segmented from the susceptibility maps using a semi-automated method in ITK-SNAP7 [Figure3a]. ROI mean (Δχvein-water) and standard deviations were calculated and Yv estimated using3:
$$Y_{v} = 1 - \frac{\Delta \chi_{vein-water} - (\Delta \chi_{oxy-water} \cdot Hct)}{(\Delta \chi_{do} \cdot Hct) }$$
Where Δχdo is the oxygenated - de-oxygenated haemoglobin χ difference (0.27x4π ppm [SI]), Δχoxy-water is the χ difference between water and oxygenated haemoglobin (-0.03x4π ppm [SI]), and Hct is blood hematocrit.
For each SCA subject, Hct was measured in the blood drawn closest to the MRI examination. For HC subjects, Hct was estimated based on age and sex8. Cognitive performance was assessed in all participants using the Wechsler Intelligence Scales9. The presence of SCI was identified by a neuroradiologist on T2-weighted FLAIR images. In POMS subjects, total hours of APAP treatment was used as a measure of treatment compliance.
ANOVA was performed to evaluate the effect of SCA on Yv, and to examine the effect of SCI in both SCA and HC subjects. Because no significant effect of age on Yv was observed, it was not included as a covariate. A trend to lower Yv was observed in male SCA subjects (p<0.1), therefore sex was included as a covariate.
Results
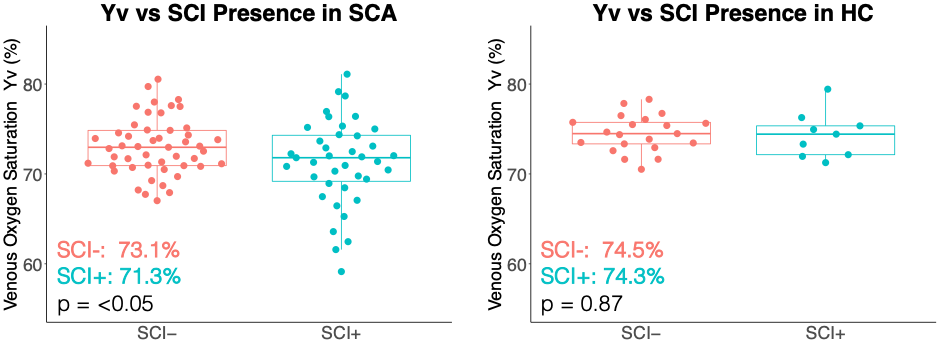
Significantly lower SSS Yv was measured in SCA subjects relative to HC (72.3 vs 74.5 %, p<0.005) [Figure 3b]. Within the SCA cohort, subjects with SCI had significantly lower Yv than those without (71.3 vs 73.1 %, p = <0.05) [Figure 4]. In the HC cohort, no Yv differences were observed between subjects with and without SCI. There was no significant correlation between measures of Yv and cognitive performance indicators in the SCA, HC or combined groups [not shown].No significant Yv difference was observed between the SCA APAP and SOC groups. However, within the APAP group, changes in Yv were positively correlated with total hours of APAP [Figure 5].
Discussion
The diminished Yv observed in SCA relative to HC agrees with previous studies1,4 and may result from haemolytic anaemia reducing the arterial oxygen content, causing a greater oxygen extraction fraction and lowering Yv. The further decrease in Yv observed in SCA subjects with SCI supports the hypothesis that SCI presence is linked to haemodynamic stress. The significant differences we observed in QSM Yv are relatively small, possibly because Yv was measured within the large SSS. More localized upstream changes in Yv could be examined by segmenting smaller venous structures.Although they were receiving APAP treatment, some participants showed decreases in Yv similar to those seen in many SCA patients given standard care during the same time-period. Alternative measures of compliance, including days since last APAP treatment and distribution of treatment hours may provide more insight into the observed Yv changes.
Conclusion
Quantitative Susceptibility Mapping showed significantly lower venous oxygenation (Yv) in subjects with sickle cell anaemia (SCA) relative to healthy controls. SCA subjects with silent cerebral infarcts (SCI) showed reduced Yv relative to patients without SCI. In SCA subjects receiving automatic positive airways pressure treatment, changes in Yv were positively correlated with treatment compliance.Acknowledgements
Dr Karin Shmueli is supported by European Research Council Consolidator Grant DiSCo MRI SFN 770939. Hanne Stotesbury was funded by Action Medical Research (GN2509) and Jamie Kawadler was funded by Great Ormond Street Children’s Charity (V4615). The National Institute for Health Research (UK; PB-PG-1112-29099) and NHLBI (R01HL079937) provided funding for patient recruitment. The work was supported by the National Institute for Health Research and Biomedical Research Centre at Great Ormond Street Hospital for Children NHS Foundation Trust and the Institute of Child Health (IS-BRC-1215-20012).References
1. Jordan LC, Gindville MC, Scott AO, et al. Non-invasive imaging of oxygen extraction fraction in adults with sickle cell anaemia. Brain. 2016;139(3):738-50.
2. Bush AM, Coates TD, Wood JC. Diminished cerebral oxygen extraction and metabolic rate in sickle cell disease using T2 relaxation under spin tagging MRI. Magnetic resonance in medicine. 2018;80(1):294-303.
3. Weisskoff R, Kiihne S. MRI Susceptometry: Image-Based Measurement of Absolute Susceptibility of MR Contrast Agents and Human Blood. Magnetic resonance in medicine. 1992;383(24):375–83.
4. Guilliams KP, Fields ME, Ragan DK, et al. Red cell exchange transfusions lower cerebral blood flow and oxygen extraction fraction in paediatric sickle cell anaemia. Blood. 2018;131(9):1012–21.
5. Howard J, Inusa B, Liossi C, et al. Prevention of Morbidity in sickle cell disease - qualitative outcomes, pain and quality of life in a randomised cross-over pilot trial of overnight supplementary oxygen and auto-adjusting continuous positive airways pressure (POMS2a): Study protocol for a randomised controlled trial. Trials. 2015;16(1):376.
6. Vanderbilt University School of Medicine Department of Pediatrics. The Sleep and Asthma Cohort (SAC) Study [Internet]. 2011. p. https://pediatrics.mc.vanderbilt.edu/interior.php? Available from: https://pediatrics.mc.vanderbilt.edu/interior.php?
7. Yushkevich PA, Piven J, Hazlett HC, et al. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage. 2006;31(3):1116–28.
8. Castro OL, Haddy TB, Rana SR. Age- and sex-related blood cell values in healthy black Americans. Public Health Reports; 1987;102(2):232–237.
9. Wechsler D. Wechsler Memory Scale (WMS- III): Administration and Scoring Manual. 3rd ed. San Antonio, TX: Psychological Corp; 1997.
Figures