3946
Intra-oral flexible coil for improved visibility of dental root canals in MRI1Dept. of Radiology, Medical Physics, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 2Department of Oral and Maxillofacial Surgery, Medical Center – University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany, 3German Consortium for Translational Cancer Research Partner Site Freiburg, German Cancer Research Center (DKFZ), Heidelberg, Germany
Synopsis
Accurate detection of dental root canals is vital to avoid complications in endodontic therapy; however, it is difficult to locate the root canals with their sub-millimeter diameter in dental CT. To display root canals with MRI, ex-vivo and in-vivo measurements were performed with a newly developed intra-oral flexible coil and were compared to conventional head and surface coil images. Ex-vivo, a minimum SNR gain of 6 could be achieved with the intra-oral coil setup, and in a volunteer a gain of 2.7 was seen with an improved delineation of the root canals.
Introduction
Dental caries can cause advanced bacterial infections which lead to root canal treatments. However, residual contamination can cause reinfection that leads to complications such as revisions, apicoectomies and extractions. Thus, there is an increased interest in non-invasive imaging methods to accurately depict root canals for improved prognosis of endodontic treatments. The current gold standard for 3D dental imaging is cone beam computed tomography (CBCT)1 which depicts mainly solid tooth structures. Dental MRI offers the advantage of an improved periapical soft tissue contrast leading to a better root canal visibility and an improved prognosis of vitality2–5. In periapical lesions MRI could show all lesions seen in CBCT, but it also provides a significantly more accurate representation of the expected demineralization size3. Regarding periapical histology, MRI offered a closer prognosis estimation6. In addition, MRI can visualize lesions and cracks in solid tissues with ultra-short T2* on clinical MR systems7,8. However, conventional MRI coils offer a limited sensitivity for dental imaging, resulting in insufficient visibility and SNR for root canal depiction.Dedicated dental coils are located extra-orally with multi-elements covering both dental arches9,10, or intra-oral coils are used which are e.g. inductively-coupled to an external receive coil11. Here, we present a new design of a slim and flexible inductively-coupled intra-oral coil which is better adapted to the dental anatomy and which has an improved sensitivity for dental pulp and root canal visibility.
Materials and Methods
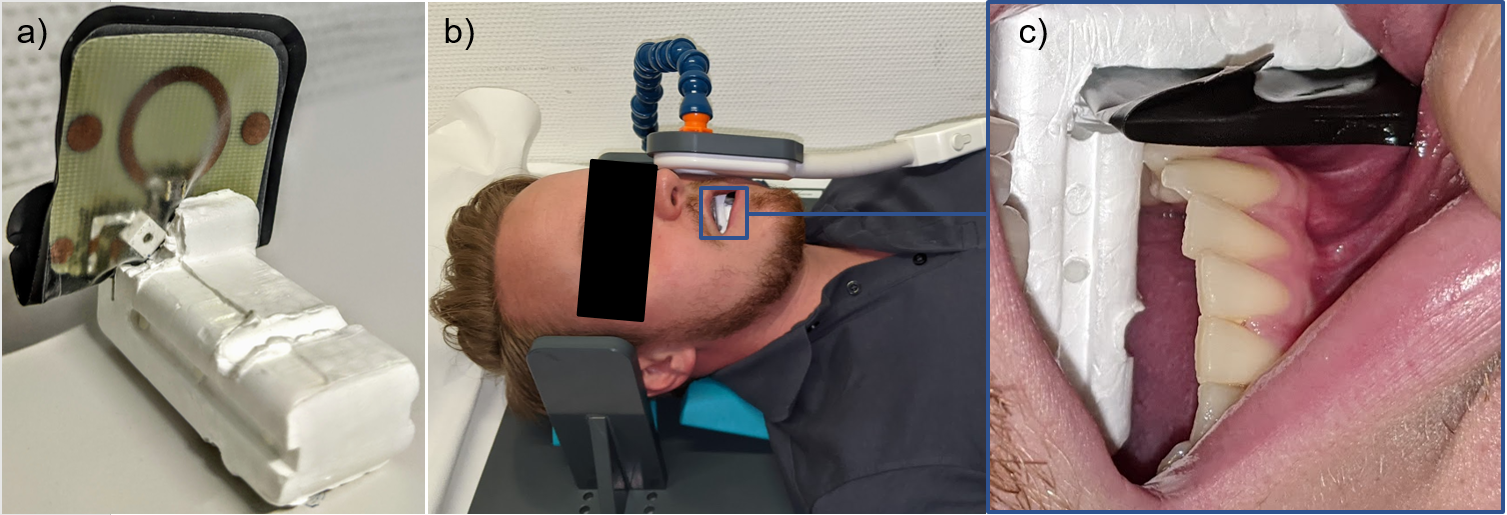
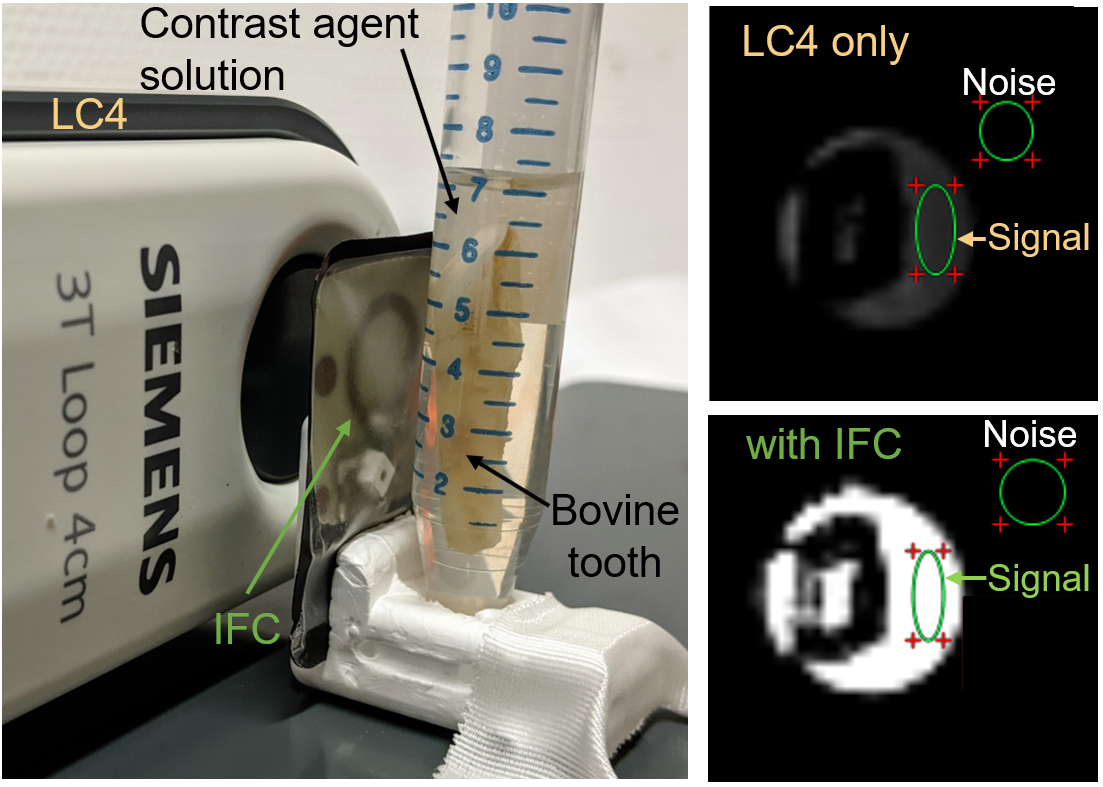
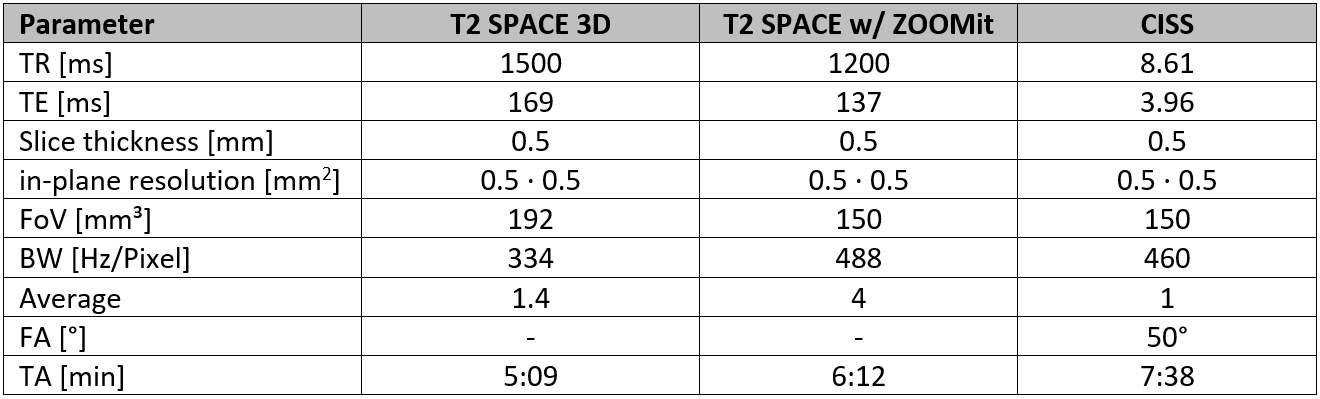
An inductively-coupled flexible coil (IFC) was fabricated on flexible PCB (Figure 1a). The coil had a diameter of 15 mm, an unloaded Q factor of 47 and was tuned to a resonant frequency of 123.2 MHz. A pair of crossed diodes was integrated for detuning during RF excitation with the body coil. The IFC was placed in a disposable dental X-ray film sleeve (Henry Schein Dental Deutschland GmbH) to prevent saliva from entering the coil. For fixation within the intra-oral cavity polystyrene bite blocks were used. For an SNR comparison, MRI experiments were performed at a 3T clinical MR system (PrismaFit, Siemens) with three different coil setups for signal reception: (1) a 32ch head coil alone, (2) a 4cm surface loop (LC4) alone, and (3) the intra-oral IFC in combination with the LC4 loop coil. Measurements were conducted in a phantom (bovine tooth in water, Fig. 2) and in a healthy volunteer. A custom-built coil holder was used which provides reproducible positioning of the external LC4 adjacent to the left mandible, and the IFC was placed next to tooth 36 (Figure 1b,c).The following imaging protocols were used: a 3D T2 SPACE (modified Fast Spin Echo) without and with parallel transmit for Field-of-View (FoV) reduction (ZOOMit)12 and a constructive interference steady state (CISS) sequence (Table 1). For reference, a CBCT data set was acquired (Orthophos SL, Dentsply Sirona, Germany) with a dose of 943 mGycm2, tube voltage 85 kV, tube current 6 mA.
Results
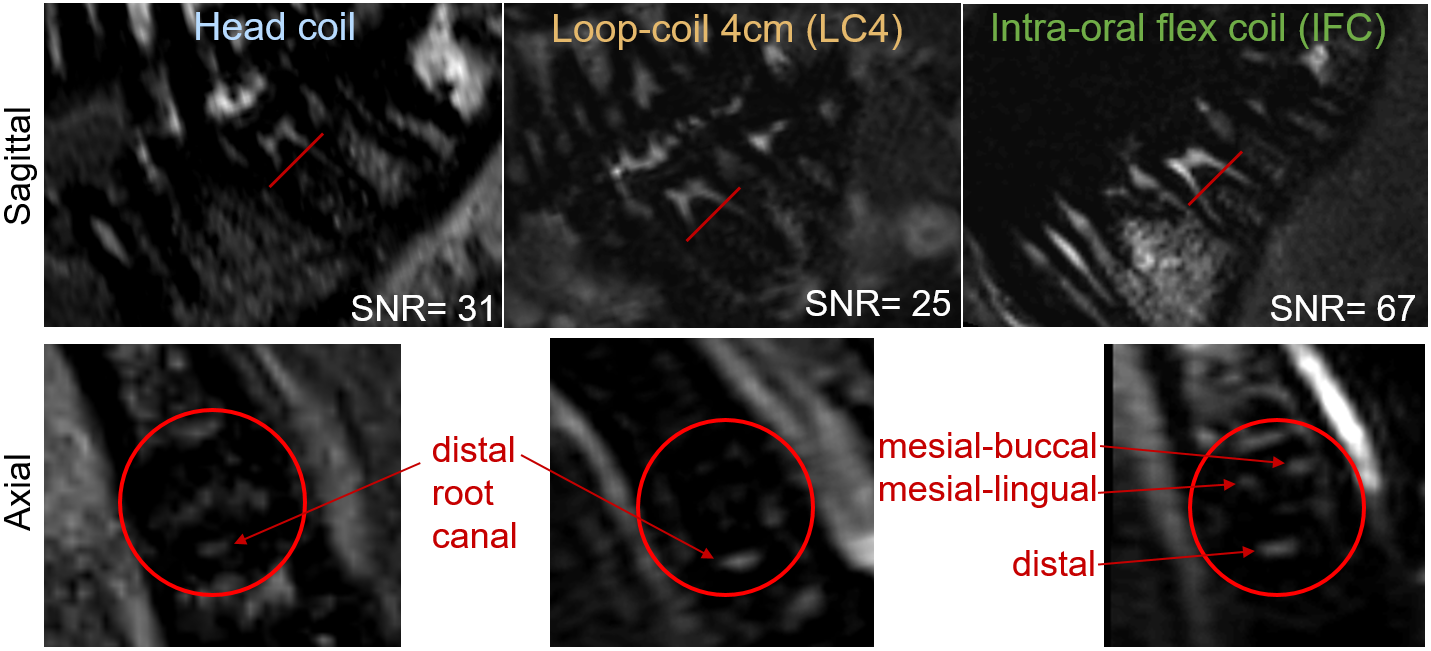
Ex-vivo T2 SPACE measurements resulted in an SNR of 53 for LC4 alone, and of 315 in combination with the IFC (gain: 6). In the volunteer similar SNRs were obtained with the external coils alone (head coil/LC4: SNR = 31/25) while the addition of the IFC improved the SNR by about 2.7 (Figure 3). ZOOMit and CISS sequences show clear visibility of the pulp throughout the root canals with comparable quality to the CBCT in clinically relevant scan times.Discussion
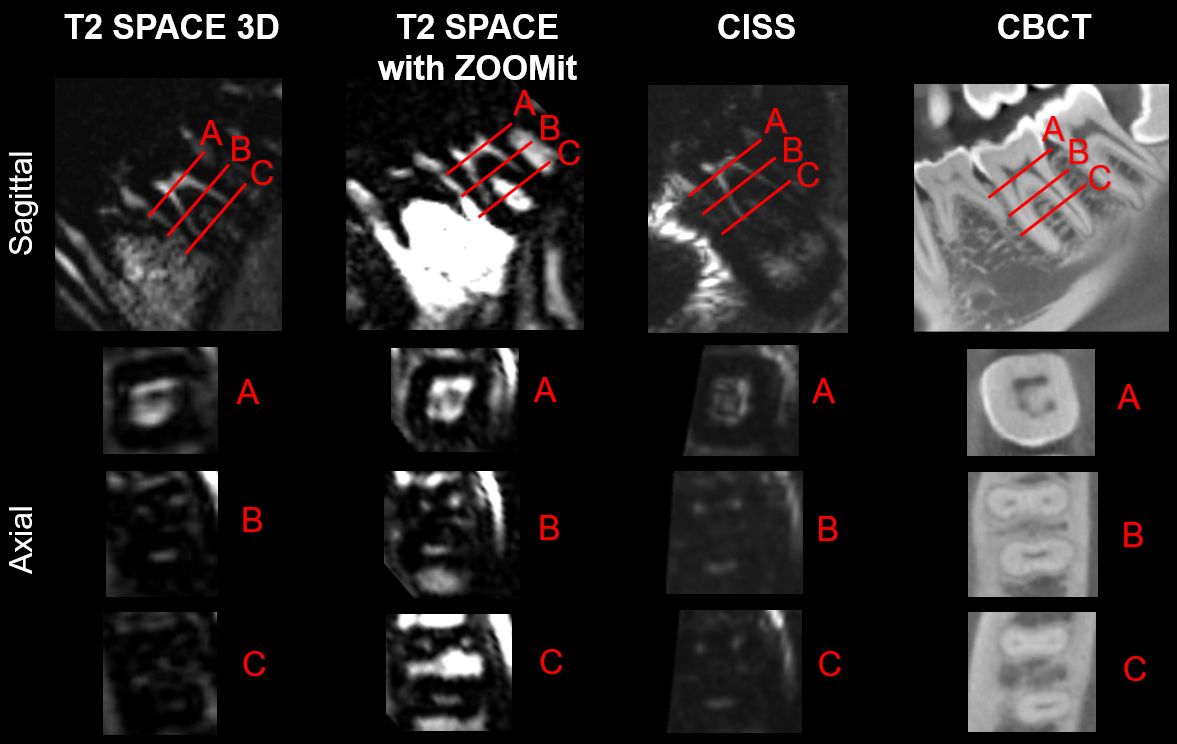
As expected, the high proximity of the IFC to the tooth maximizes SNR compared to external coils. In axial slice orientation the IFC showed superior performance with a clear visibility of the mesial-lingual, mesial-buccal and the distal root canal,whereas only the distal root canal with a width of around 0.7 mm at the center was visible for the external coils. However, intra-oral coil placement affected the Q factor and the coil coupling which required re-positioning of the LC4 readout coil to optimize the SNR. T2 SPACE images had the highest SNR and clear visibility of surrounding tissue but showed a lower root canal visibility in axial orientation. The CISS data demonstrated high root canal visibility throughout all axial planes; however, in sagittal orientation, CISS suffered from banding artefacts through the pulp and the surrounding gum. The T2 SPACE with ZOOMit had the highest contrast of root canal visibility and the further reduction of FoV allowed for accurate visualization through all axial slices (cf. slice A, B and C in Figure 4). We showed that the pulp consisting of branch tissue can be visualized up to the tip of the root. Compared to X-Ray, which depends on the demineralization of the mineralized tissue, pathologies could be displayed at an earlier point in time4.Conclusion
Dental MRI with an intra-oral flexible coil allows clear visualization of dental root canals within clinically relevant scan times (5-7 min) for in-vivo with comparable results to CBCT. An isotropic resolution of 0.5 mm can be achieved which allows to visualize root canals in both sagittal and axial orientation up to the root tip.Acknowledgements
Grant support from the Deutsche Forschungsgemeinschaft (DFG) under grant numbers BO 3025/8-1 and UL 1187/6-1 is gratefully acknowledged.References
1. Chauhan, V. & Wilkins, R. C. A comprehensive review of the literature on the biological effects from dental X-ray exposures. Int J Radiat Biol 95, 107–119 (2019).
2. Assaf, A. T. et al. Evaluation of four different optimized magnetic-resonance-imaging sequences for visualization of dental and maxillo-mandibular structures at 3 T. Journal of Cranio-Maxillofacial Surgery 42, 1356–1363 (2014).
3. Geibel, M. A. et al. Assessment of Apical Periodontitis by MRI: A Feasibility Study. Rofo 187, 269–275 (2015).
4. Kress, B. et al. Quantitative analysis of MRI signal intensity as a tool for evaluating tooth pulp vitality. Dentomaxillofacial Radiology 33, 241–244 (2004).
5. Newton, C. W., Hoen, M. M., Goodis, H. E., Johnson, B. R. & McClanahan, S. B. Identify and Determine the Metrics, Hierarchy, and Predictive Value of All the Parameters and/or Methods Used During Endodontic Diagnosis. Journal of Endodontics 35, 1635–1644 (2009).
6. Geibel, M.-A. et al. Characterisation of apical bone lesions: Comparison of MRI and CBCT with histological findings - a case series. Eur J Oral Implantol 10, 197–211 (2017).
7. Bracher, A.-K. et al. Ultrashort echo time (UTE) MRI for the assessment of caries lesions. Dentomaxillofac Radiol 42, 20120321 (2013).
8. Idiyatullin, D. et al. Dental Magnetic Resonance Imaging: Making the Invisible Visible. Journal of Endodontics 37, 745–752 (2011).
9. Prager, M. et al. Dental MRI using a dedicated RF-coil at 3 Tesla. Journal of Cranio-Maxillofacial Surgery 43, 2175–2182 (2015).
10. Sedlacik, J. et al. Optimized 14 + 1 receive coil array and position system for 3D high-resolution MRI of dental and maxillomandibular structures. Dentomaxillofac Radiol 45, 20150177 (2016).
11. Ludwig, U. et al. Dental MRI using wireless intraoral coils. Scientific Reports 6, 23301 (2016).
12. Blasche, M et al. TimTX TrueShape and
syngo ZOOMit Technical and Practical Aspects. in MAGNETOM Flash #49
74–84 (2012).
Figures