3936
Compressed Sensing vs. Conventional Parallel Imaging: Utility of Head and Neck MRI for Image Quality and Inspection Efficacy1Radiology, Fujita Health University School of Medicine, Toyoake, Japan, 2Canon Medical System Corporation, Otawara, Japan, 3Joint Research Laboratory of Advanced Medical Imaging, Fujita Health University School of Medicine, Toyoake, Japan, 4Fujita Health University Hospital, Toyoake, Japan
Synopsis
There have been no major reports for assessing the utility of Compressed Sensing (CS) with Parallel Imaging (PI) as compared with routinely applied conventional PI for head and neck MR imaging. We hypothesized that a newly developed CS with PI could shorten examination time and improve the image quality for head and neck MR imaging as compared with conventional PI. The purpose of this study was to directly compare the capability for examination time shortening and image quality improvement of head and neck 3T MR imaging between CS with PI and conventional PI.
Introduction
Since the beginning of the 2000s, improving temporal and spatial resolution for MR imaging have been tested, not only by using image domain-based parallel imaging (PI) techniques, but also the k-space domain-based parallel imaging technique for 1.5 and 3 Tesla (T) MR systems.1 However, it has been suggested that the advantages of a reduction in examination time and improvements in temporal and spatial resolution by using conventional PI are limited due to the increase in the number of coil elements. Compressed sensing (CS) has recently been introduced as a new method for reducing the number of k-space samples by exploiting compressibility or sparsity in an appropriate transform domain.2 However, it has been found that one of the drawbacks of simply reducing k-space sampling for CS may be relatively lower signal-to-noise ratio (SNR) than conventional PI. This situation led to the recent development of new CS methods by a few MR vendors. These methods were combined CS with PI and clinically tested for body MR imaging in various organs. In contrast with routinely applied PI, however, no major studies have been reported for assessing the utility of CS with PI for head and neck MR imaging.3 We hypothesized that a newly developed CS with PI could improve the image quality and shorten examination time for head and neck MR imaging as compared with conventional PI. The purpose of this study was thus to directly compare the capability for examination time shortening and image quality improvement of head and neck 3T MR imaging between CS with PI and conventional PI.Materials and Methods
Thirty consecutive patients underwent head and neck MR imaging by CS with PI (Compressed SPEEDER: Canon Medical Systems Corporation, Otawara, Japan) and conventional PI (SPEEDER: Canon Medical) using a 3T system (Vantage Galan 3T / ZGO, Canon Medical). In each patient, examination times for CS with PI and conventional PI were recorded. For quantitative image quality assessment, signal-to-noise ratio (SNR), percentage of coefficient of variation (%CV) and contrast-to-noise ratio (CNR) were calculated. For qualitative assessment, two board certified radiologists with more than 10 years experiences assessed overall image quality, artifacts and diagnostic confidence level using a 5-point scoring system. Then, each final score was determined by consensus of two readers in all subjects. To determine the capability for examination time shortening by CS with PI, mean examination time was compared between two methods by Wilcoxon signed-rank test. To evaluate the utility of CS with PI for quantitative image quality improvement, the paired t-test was used to compare SNR of CS with PI and conventional PI. In addition, %CV and CNR of the two methods were compared by using the Wilcoxon signed-rank test. As for qualitative image quality, inter-observer agreement for each index was evaluated by applying the χ2 test to the kappa statistics. Finally, the Wilcoxon signed-rank test for the two methods was then used to compare each qualitative index obtained with the two methods.Results
A Representative case is shown in Figure 1. Mean examination time for CS with PI (83.5±11.0s) was significantly shorter than that for conventional PI (173.0±54.4s, p<0.0001). A comparison of quantitatively assessed image quality is shown in Figure 2. SNR, %CV and CNR of CS with PI (SNR: 11.2±3.6, %CV: 9.6±3.0, CNR: 7.7±2.9) were significantly better than those of conventional PI (SNR: 8.9±2.6, p<0.0001; %CV: 11.9±3.5, p<0.0001; CNR: 6.1±2.2, p<0.0001). Figure 3 shows the inter-observer agreements for all qualitative image quality indexes for CS with PI and conventional PI. Inter-observer agreements of each category on both methods were assessed as significant and substantial (overall image quality: 0.67<κ<0.71, p<0.0001; artifact: 0.65<κ<0.81, p<0.0001; diagnostic performance: 0.62<κ<0.73, p<0.0001). Figure 4 shows the results of comparison for each qualitative image quality index between the two methods. There were no significant differences between the two methods in overall image quality (CS with PI vs. conventional PI: 4.3±0.9 vs. 4.5±0.7, p=0.15), artifact (CS with PI vs. conventional PI: 2.3±0.9 vs. 2.1±0.7, p=0.30) and diagnostic confidence level (CS with PI vs. conventional PI: 4.8±0.5 vs. 4.9±0.3, p=0.18).Conclusion
Compressed sensing with parallel imaging has a better capability than conventional parallel imaging for improving head and neck MR imaging with a shorter examination time and quantitatively better image quality and without any significant deterioration of qualitative image quality for head and neck MR examinations. In addition, compressed sensing with parallel imaging can be used as a substitute for conventional parallel imaging in routine clinical practice.Acknowledgements
No acknowledgement found.References
1. Deshmane A, Gulani V, Griswold MA, et al. Parallel MR imaging. J Magn Reson Imaging 2012; 36:55-72
2. Feng L, Benkert T, Block KT, et al. Compressed sensing for body MRI. J Magn Reson Imaging 2017; 45:966-987
3. Touska P, Connor SEJ. Recent advances in MRI of the head and neck, skull base and cranial nerves: new and evolving sequences, analyses and clinical applications. Br J Radiol 2019; 92:20190513
Figures
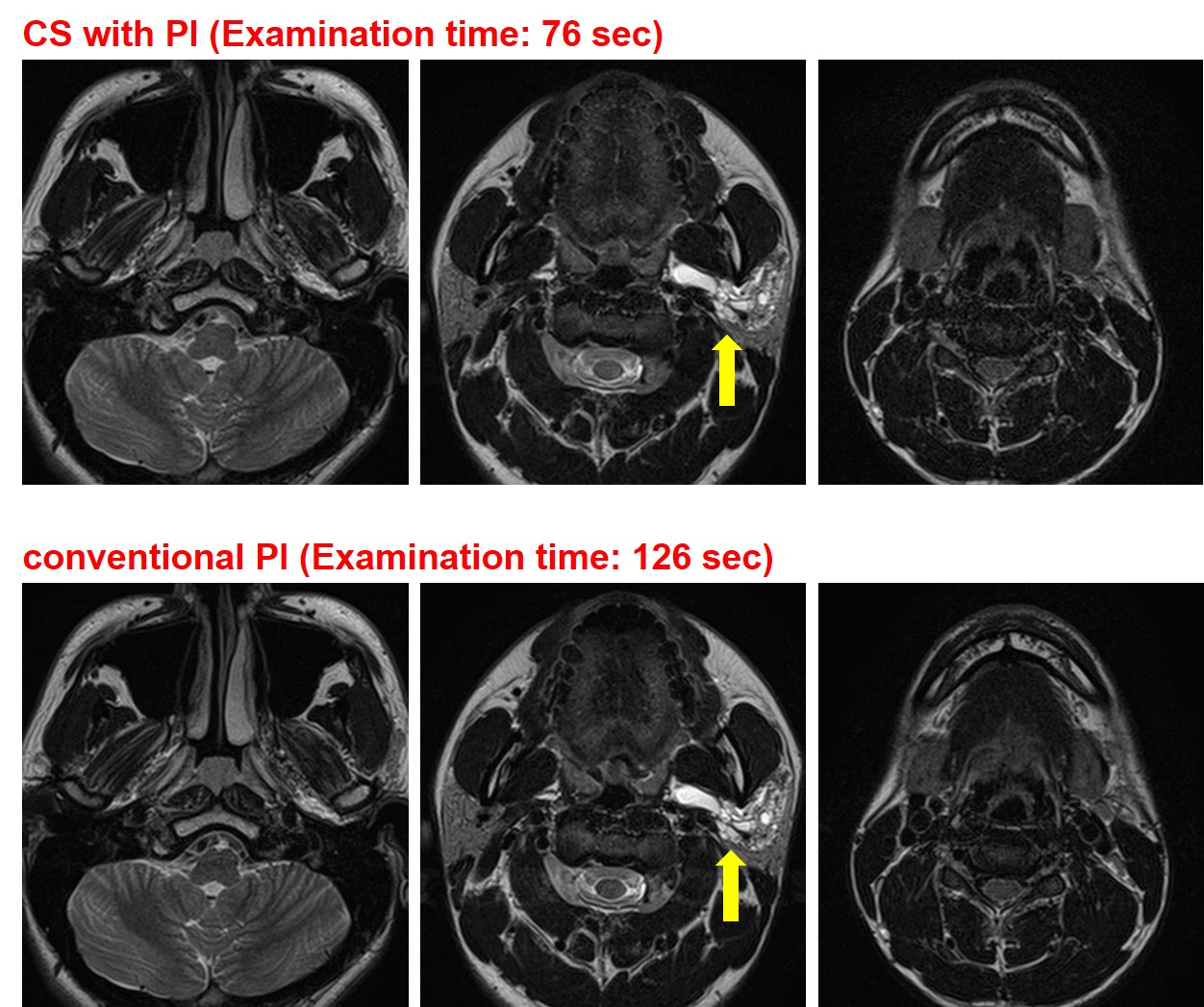
Figure1. 21-year-old male with lymphatic malformation (L to R: cranial to caudal level).
T2-weighted images obtained with CS with PI and with conventional PI clearly demonstrate the multiple cystic lesions extending from parotid space to parapharyngeal space (arrows). Neither image showed significant artifacts and both had the same overall image quality. The examination time of CS with PI (76 sec) was much shorter than that of conventional PI (126 sec).
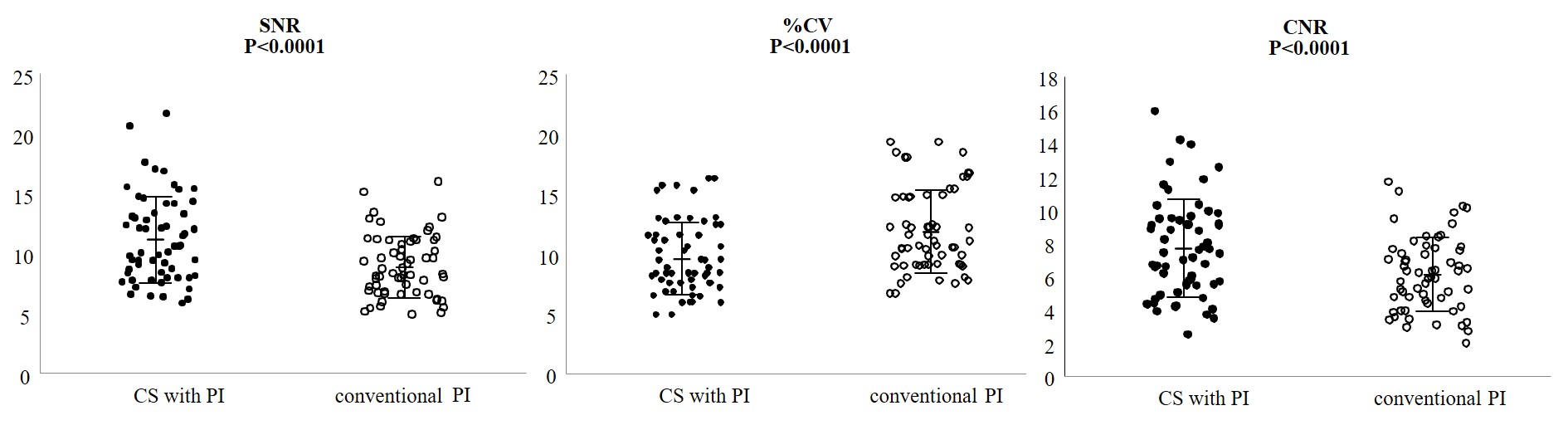
Figure 2. Results of comparison for each quantitative image quality index among CS with PI and conventional PI.
SNR of CS with PI (11.2±3.6, mean ± standard deviation) was significantly higher than that of conventional PI (8.9±2.6, p<0.0001). %CV of CS with PI (9.6±3.0) was significantly lower than that of conventional PI (11.9±3.5, p<0.0001). CNR of CS with PI (7.7±2.9) was significantly higher than that of conventional PI (6.1±2.2, p<0.0001).
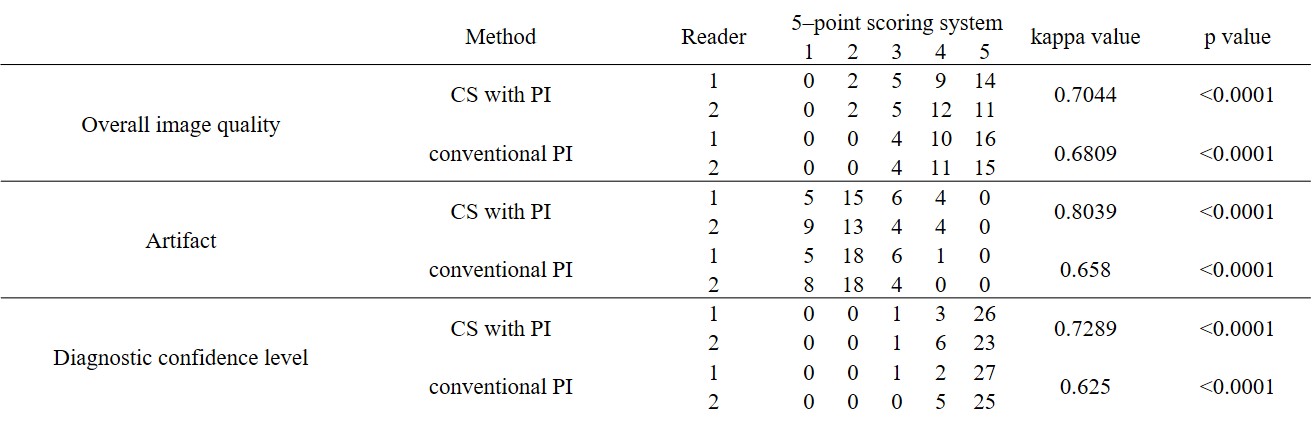
Figure 3. Results of inter-observer agreements for each quality index between two leaders on CS with PI and conventional PI
All interobserver agreements for CS with PI (overall image quality: κ=0.70, p<0.0001; artifact: κ=0.80, p<0.0001; diagnostic confidence level: κ=0.73, p<0.0001) and conventional PI (overall image quality: κ=0.68, p<0.0001; artifact: κ=0.66, p<0.0001; diagnostic confidence level: κ=0.63, p<0.0001) were assessed as significant and substantial.
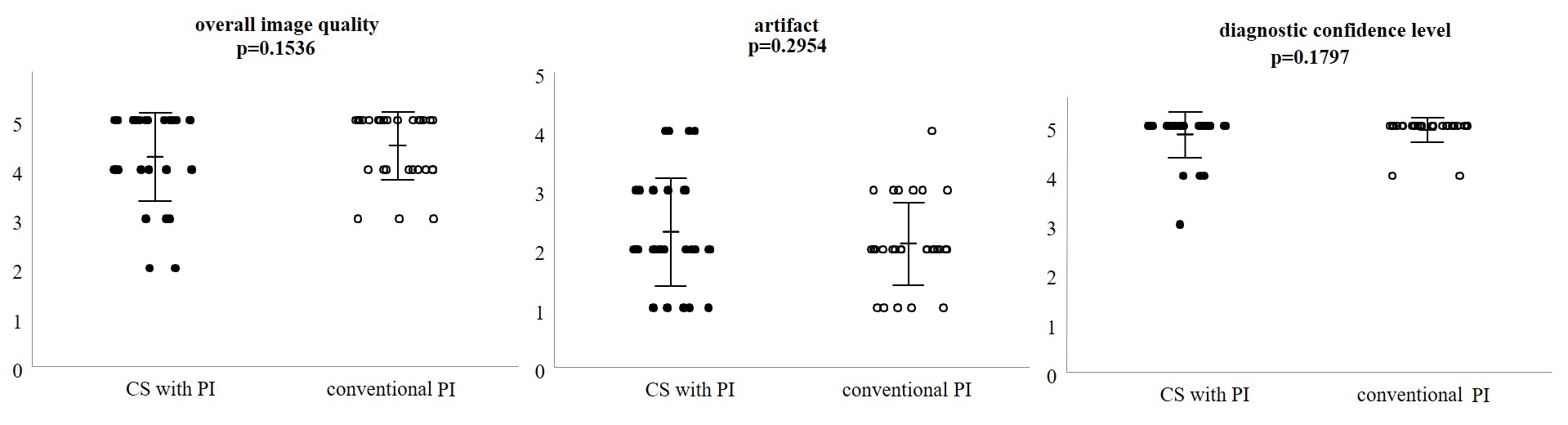
Figure 4. Individual qualitative image quality indexes for CS with PI and conventional PI
Overall image quality of CS with PI (4.3±0.9, mean ± standard deviation) had no significant difference with that of conventional PI (4.5±0.7, p=0.15). Artifact of CS with PI (2.3±0.9) had no significant difference with that of conventional PI (2.1±0.7, p=0.30). Diagnostic confidence level of CS with PI (4.8±0.5) was not significantly different from that of conventional PI (4.9±0.3, p=0.18).