3923
High dual-contrast putamen MRI at 1.5T: Application to intraoperative MRI during neurosurgical procedure
Chan Hong Moon1, Krystof Bankiewicz2, Paul Larson2, Adrian Kells3, Alastair J. Martin2, Stephen Mancuso4, and Mark Richardson5
1University of Pittsburgh, Pittsburgh, PA, United States, 2University of California San Francisco, San Francisco, CA, United States, 3Voyager Therapeutics Inc., Cambridge, MA, United States, 4UPMC, Pittsburgh, PA, United States, 5Massachusetts General Hospital, Boston, MA, United States
1University of Pittsburgh, Pittsburgh, PA, United States, 2University of California San Francisco, San Francisco, CA, United States, 3Voyager Therapeutics Inc., Cambridge, MA, United States, 4UPMC, Pittsburgh, PA, United States, 5Massachusetts General Hospital, Boston, MA, United States
Synopsis
Neurosurgical planning/targeting/monitoring by MRI requires high contrast and excellent anatomical feature. Inversion recovery MRI, e.g., MPRAGE is known to be superior to T1w SPGR in making high contrast of WM vs. GM. However, it is not optimized for putamen/globus pallidus, i.e., important target nuclei in PD surgery, particularly iMRI scanner 1.5T (not 3T). In this study, we developed new dual-contrast MPRAGE and maximized T1 contrast in putamen as well as good anatomy of whole brain without additional acquisition compared to conventional MPRAGE. The proposed methods were applied to 1.5T iMRI during neurosurgical procedure of PD patients.
Introduction
Targeting/monitoring of a specific brain region, e.g., putamen (Put) by interventional MRI (iMRI) during neurosurgical procedure requires high contrast 3D anatomy imaging within reasonable time, <4min. Conventional T1w MRI (e.g., SPGR or MPRAGE) at 1.5T is applied for targeting Put of Parkinson’s disease (PD) patient during neurosurgical procedure for enzyme Aromatic L-Amino Acid Decarboxylase (AADC) gene delivery because of its high resolution and overall good contrast over whole brain[1,2]. However, current T1w MRI cannot produce high contrast of Put against neighboring WM. In this study, dual T1 contrast MPRAGE sequence was developed at clinical 1.5T, and the imaging parameters were optimized to obtain the highest contrast in Put as well as good anatomy of whole brain. The optimized Put MRI sequences were applied to neurosurgical targeting, planning and monitoring for infusions of gene therapeutic agents during iMRI.Methods
All MR measurements were performed at Siemens 1.5T with 4ch flexible coil (wrapped around posterior or anterior head). Two healthy subjects were recruited for optimization of new sequence parameters and the evaluation of the image quality. Two PD patients were recruited for AADC gene therapy study and had neurosurgical operation with infusion of AADC viral VY-AADC01 vector during iMRI. Optimal TI of MPRAGE was simulated for Put, caudate (CA) and globus pallidus (GP) at 1.5T[3,4]. In addition, to expedite empirical optimization of TI in IR sequence, 2D MPRAGE sequence with same contrast as in 3D MPRAGE was designed. Fast 2D MPRAGE parameters were axial slice, FOV 240x195mm2, matrix 256x156, PE PF 7/8, BWP 200Hz, TR/TE/TI = 2,400/2.32/200 – 850ms, and slice thickness 5.5mm. Dual T1 contrast 3D MPRAGE was implemented by adding two SPGR acquisitions at different TI per same TR; FOV RO 240mm, FOV PE1 81.3%, PE1 resolution 82%, matrix size 171x256, PE1 PF 7/8, BWP 200Hz, TR/TE/TI = 2,400/2.67/330 – 880ms, slice thickness 1.2mm, slices per slab 112 with OS 14.3%, slice encoding (PE2) resolution 66%. In 2D MPRAGE, the axial plane in the middle of Put was chosen and the imaging was repeated 10 times and averaged. ROIs of Put, GP and adjacent WM were manually drawn, and the mean signals within the ROIs were used to calculate the contrast based on |IPut/GP - IWM|/|IPut/GP + IWM|, where IPut/GP and IWM is the mean image intensity in Put or GP and WM. The criteria of optimal TI were the highest contrast and difference signal; when TIs of peak contrast and difference are not matched, approximately middle of two TIs was chosen. For iMRI for AADC viral vector infusion, PD patient’s head was fixed in an MR compatible stereotactic frame in supine or prone position, and the cannula trace was guided by ClearPoint system (MRI INTERVENTIONS, CA) under anesthetic condition. The proposed 3D dual T1 contrast MPRAGE was acquired pre- and post-neurosurgical procedure. Other MR images were compared regarding the contrast of Put and the brain anatomy.Results
Optimal simulated TI for the highest contrast and singal of Put was ~330ms under applied MPRAGE parameters. The experimental optimal TI in 2D IR sequence was also similar to the simulation results (Fig. 1). 3D MPRAFGE images acquired at multiple TIs around the optimal TI ~330ms were acquired and compared to conventional MPRAGE image (Fig. 2). MPRAGE image at TI 330 and 350ms showed good morphology features of Put and also GP which is invisible in conventional MPRAGE image (Figs. 2A,D). With the increase of TI 370ms, WM intensity is recovered but still the contrast was superior to that of conventional MPRAGE (Fig. 2C). Ortho-planar images of optimal TI MPRAGE showed excellent 3D Put morphology (Figs. 2E,F). The new dual T1 contrast MPRAGE was applied to iMRI for neurosurgical planning and real-time monitoring of AADC infusion (Fig. 3). Note that new dual T1 MPRAGE at 1.5T can provide higher contrast of Put than that at 3T.Discussion/Conclusions
The proposed MRI method of striatum with TI optimized MPRAGE demonstrated high contrast of Put and GP by suppression of the surrounding WM. The proposed fast 2D MPRAGE method for empirical optimization of TI was validated through comparison with simulation, and could be applied to find subject-dependent optimal TI onsite during iMRI procedure, which is clinically valuable. In the study, two T1 contrasts can be simultaneously acquired by dual T1 contrast MPRAGE sequence, and was successfully applied to neurosurgical planning and procedure with AADC infusion study targeting Put and monitoring the agent infusion process. The developed method with flexible T1 contrast via TI control could be used for targeting other brain nuclei during iMRI, for example, SN.Acknowledgements
This work was supported by NCT01973543 and NCT03065192 sponsored by Voyager Therapeutics.References
1. Christine et al, Neurology, 2009; 2. Richardson et al, SFN,89,p141-151, 2011; 3. Deichman et al, NI,12, p112-127, 2000; 4. Wang et al, PLOS,5,e96899, 2014.Figures
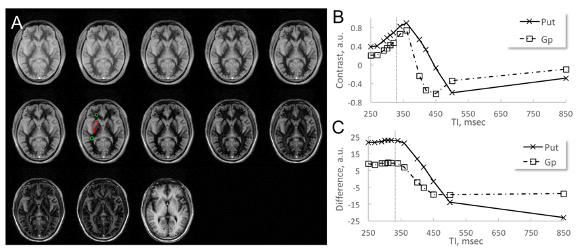
Fig. 1 Striatum contrast measurement with TI in 2D MPRAFGE imaging. A, IR MR images from TI 250 msec to 850 msec (from top-left to bottom-right). ROI of white mater, putamen and globus pallidus was manually drawn in each region. B and C, Contrast and difference of putamen and globus pallidus from white mater. Optimal TI ~330 msec (gray dotted lines in B and C) was selected between TIs of maximum contrast and signal difference.
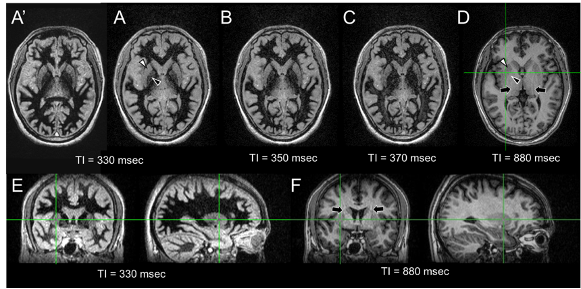
Fig. 2 3D MPRAFGE MR images at effective TI 330 (A and A’), 350 (B), 370 (C) and 880 msec (D) at kz = 0; only axial images are shown. The images in A and A’ were acquired at a week apart sessions. Black arrows indicate the aliasing artifact in conventional MPRAGE image. Note that the signal in the white mater at optimal TI ~330 msec is well suppressed and the contrast of putamen (white arrowhead) and glubus pallidus (black arrowhead) vs. white mater is much higher than those of conventional MPRAGE image at effective TI 880 msec. In addition, the optimal TI MPRAGE MRI is reproducible.
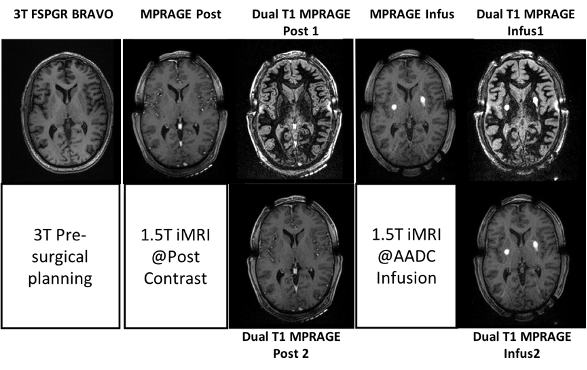
Fig. 3 T1 anatomy MRI; (from left) Pre-surgical @3T, Post contrast at1.5T (MPRAGE, dual T1 MPRAGEs) and AADC infusion at1.5T (MPRAGE, dual T1 MPRAGEs). Note that new dual T1 MPRAGE at1.5T can provide higher contrast of Put than that at 3T. In addition, dual T1 MPRAGE provides good whole brain anatomy. White spots are the targeted infusion regions.