3916
DiffusionGo: A fully automatic fiber tracking software for neurosurgeon
Shin Tai Chong1, Jianping Song2, Kuan-Tsen Kuo3, Yu-Ting Ko3, Sanford PC Hsu4, Jinsong Wu2, and Ching-Po Lin1
1Institute of Neuroscience, National Yang-Ming University, Taipei, Taiwan, 2Department of Neurosurgery, Huashan Hospital, Shanghai Medical College, Fudan University, Shanghai, China, 3ABC Solution Co., Ltd, Shanghai, China, 4Department of Neurosurgery, Neurological Institute, Taipei Veterans General Hospital, Taipei, Taiwan
1Institute of Neuroscience, National Yang-Ming University, Taipei, Taiwan, 2Department of Neurosurgery, Huashan Hospital, Shanghai Medical College, Fudan University, Shanghai, China, 3ABC Solution Co., Ltd, Shanghai, China, 4Department of Neurosurgery, Neurological Institute, Taipei Veterans General Hospital, Taipei, Taiwan
Synopsis
DiffusionGo is an in-house developed software specially designed for neurosurgeons, which integrated a reliable pre-processing pipeline, fully automatically fiber reconstruction algorithm, and multimodalities imaging information to achieve easy modeling and precision surgery.
Introduction
Diffusion tensor imaging (DTI) has been widely used to reveal and visualize the three-dimensional white matter trajectories in the human brain. This neural tracking technique provides neurosurgeons a new horizon for surgical planning to obtain a complete resection and minimize the functional loss. Although there were quite a few useful and powerful software (such as MRtrix3, FSL, DSI-studio, 3D-Slicer, etc.) have abilities to reconstruct the fiber tracts, however, the operation of these software is complicated, which needed a well-trained technician or surgeon to integrate across different software for surgical planning1. DiffusionGo is an in-house developed software specially designed for neurosurgeons, which integrated a reliable pre-processing pipeline, fully automatically fiber reconstruction algorithm, and multimodalities imaging information to achieve easy modeling and precision surgery.Method
Three-dimension T1-weighted image (T1WI) and diffusion-weighted images (DWI) were required for the following pipeline. First, all images were co-registered with DWI by using Advanced Normalization Tools (ANTs, http://stnava.github.io/ANTs/). All DWIs underwent diffusion pre-processing pipeline with MRtrix3 (https://www.mrtrix.org) and FSL (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki): 1. DWI denoising, 2. Gibbs-ringing removing, 3. Susceptibility distortion correction (process if opposite polarity data was acquired), 4. Eddy current and motion correction, 5. Bias correction, and 6. DTI fitting. A patent-protected multiple assigned criteria (MAC) algorithm for fiber tracking was used2. The motor pathway (corticospinal tract, CST), language pathway (arcuate fasciculus, AF, superior longitudinal fasciculus, SLF, frontal aslant tract, FAT, inferior longitudinal fasciculus, ILF, inferior fronto-occipital fasciculus, IFOF, and uncinate fasciculus, UF), and visual pathway (optic radiation, OR) were segmented automatically. The cortical surface was reconstructed by FreeSurfer (version 7.1, https://surfer.nmr.mgh.harvard.edu). The workflow was demonstrated in Figure 1.Results
Two demo cases application were shown in the following: The first case was a 60-year-old male with left frontal brain arteriovenous malformations (bAVM). The bAVM (32mm in diameter) had a close relationship to the language area and classified as a Modified Spetzler-Martin Grade III+ lesion with high surgical risk. Multimodality-guide awake surgery for language function mapping and preservation was used. The language task blood oxygen level-dependent (BOLD) activation map, DTI fiber tractography, and digital subtraction angiography (DSA) were integrated with DiffusionGo for surgical planning (Figure 2). Speech arrest was defined as discontinuation in number counting without simultaneous motor response by direct cortical stimulation (DCS). In the phase of language mapping, we found that the eloquence area of speech arrest was not located in the classic Broca area, but one gyrus posterior to the bAVM. The bAVM was removed and kept the language area intact. There was no language dysfunction during the whole procedure, and the intra-operative angiography shown total obliteration of the lesion.The second case was a 41-year-old female. Glioblastoma was diagnosed, 55mm in diameter, over the left temporal lobe with mild perifocal edema. She could not write or read the words which she learned before. Ignoring the objects at her right side was also noted. DTI fiber tractography of language pathways (AF, SLF II, ILF, IFOF, and UF) were reconstructed and displayed in DiffusionGo. Superior displacement of left Wernicke’s area was identified with intact AF projecting to left premotor and left Broca areas (Figure 3). After a complete survey, the surgery of craniotomy was done without any neurological deficit postoperatively. Following MRI of the brain revealed total gross removal without residual tumor.
Discussion and conclusion
We demonstrated the application of DiffusionGo in two classical language-related cases. The fully automatically processing pipeline provided the technician or surgeon with a solution that can reduce time cost and operating error. Apart from this, the results showed robust consistency with the surgical finding. We believe that this technique can improve care quality and surgical procedure quality across different facilities.Acknowledgements
No acknowledgement found.References
- Pujol S, Wells W, Pierpaoli C, et al. The DTI Challenge: Toward Standardized Evaluation of Diffusion Tensor Imaging Tractography for Neurosurgery. Journal of Neuroimaging 2015;25:875–882. doi: 10.1111/jon.12283.
- Lin CP, Chong ST, Luo CY. Method and Apparatus of Fiber Tracking, and Non-transitory Computer-readable Medium Thereof. United States Patent. US 10,497,120 B2.
Figures
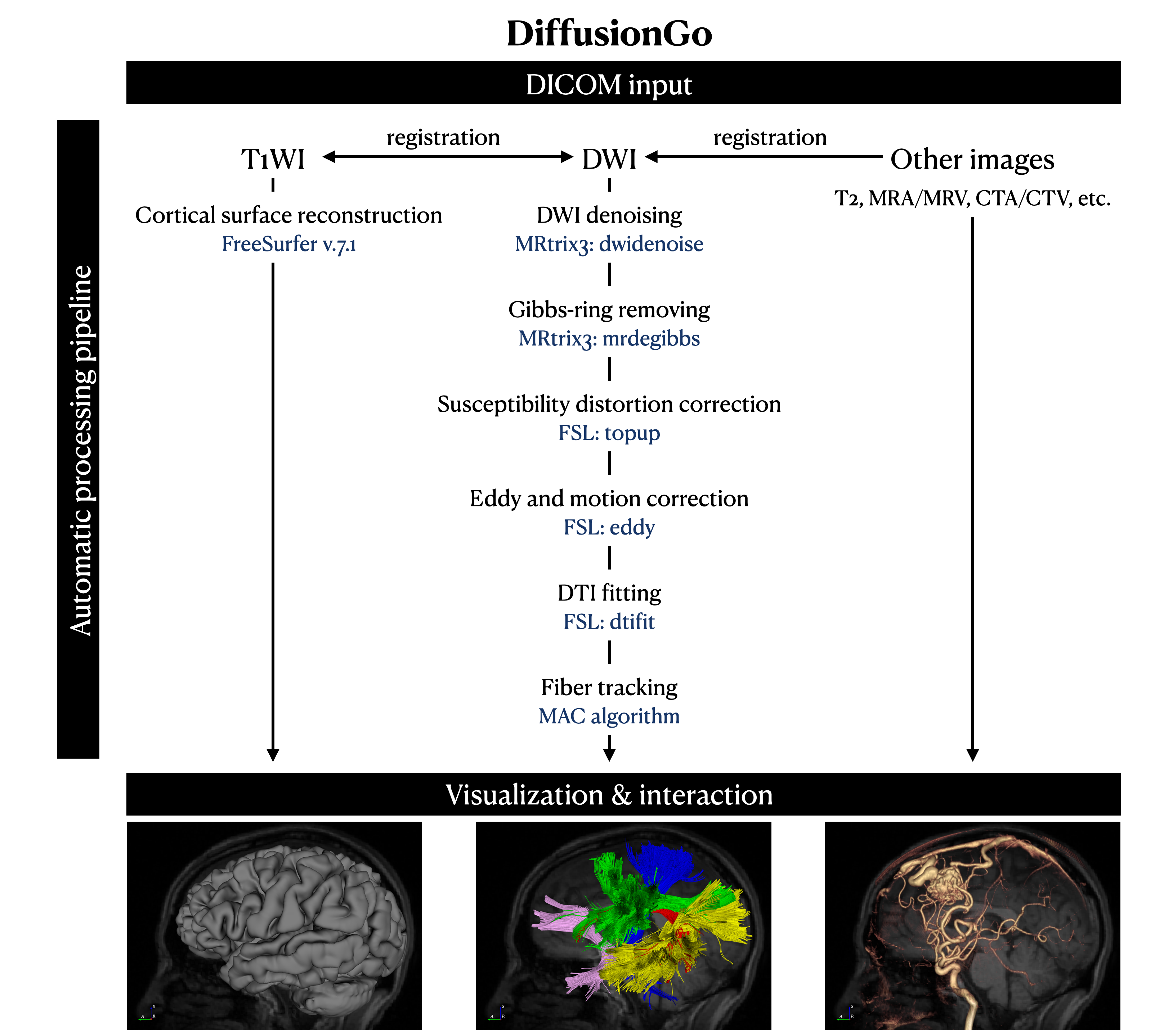
The workflow of DiffusionGo. DiffusionGo provided a fully automatic processing pipeline, 3D visualization, and interaction platform.
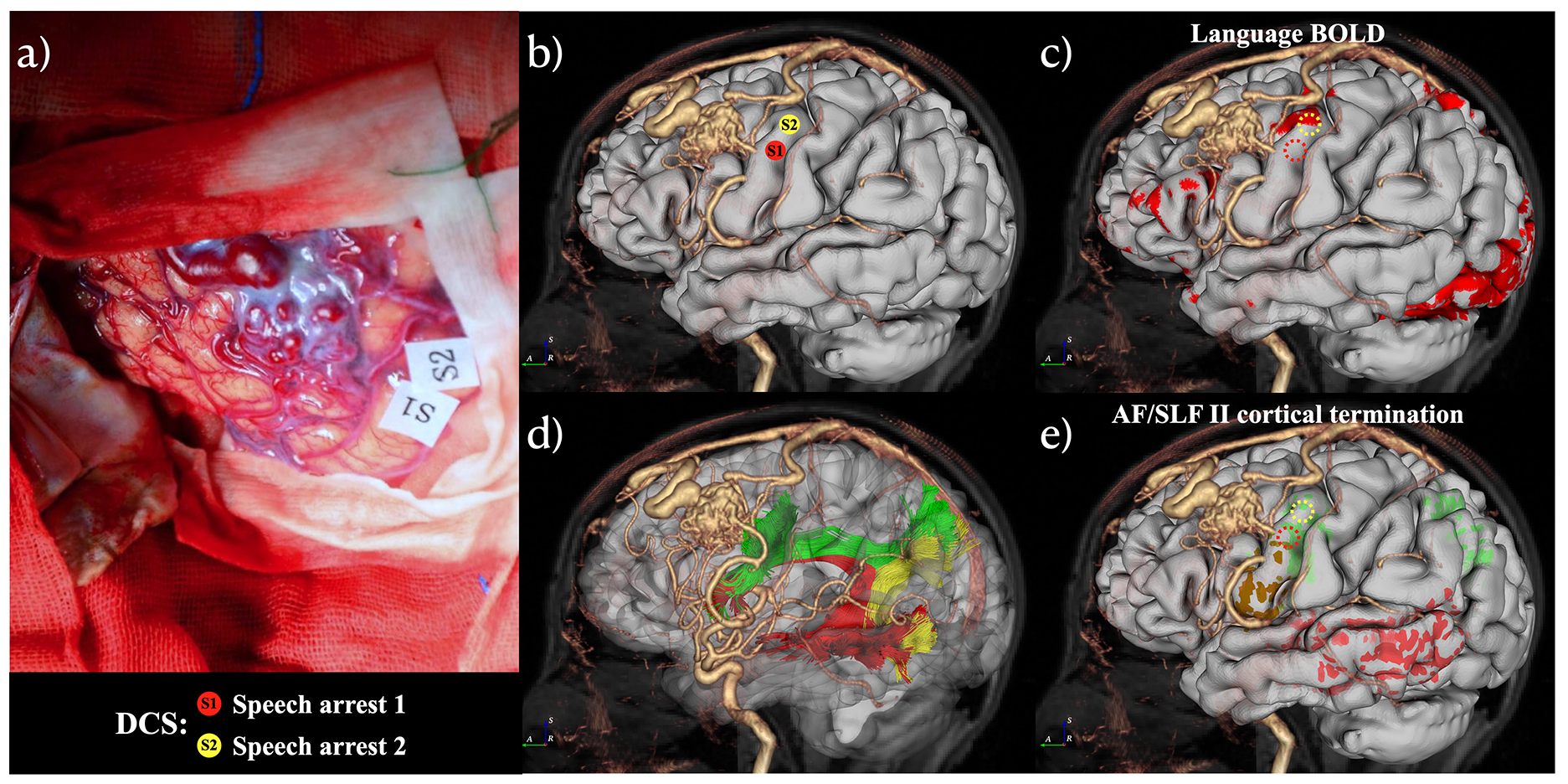
Multimodalities integration in a 60-year-old male with left frontal bAVM in DiffusionGo. S1 and S2 Speech arrest was defined as discontinuation in number counting without simultaneous motor response by DCS (a). AF (red), SLF II (green), and posterior segment of SLF (yellow) were automatically reconstructed (d). Comparing with language BOLD functional activation (c), Tract-based cortical termination (AF termination in red; SLF II termination in green; orange color represented the overlap of AF and SLF II) has more sensitivity to manifest with DCS results (e).
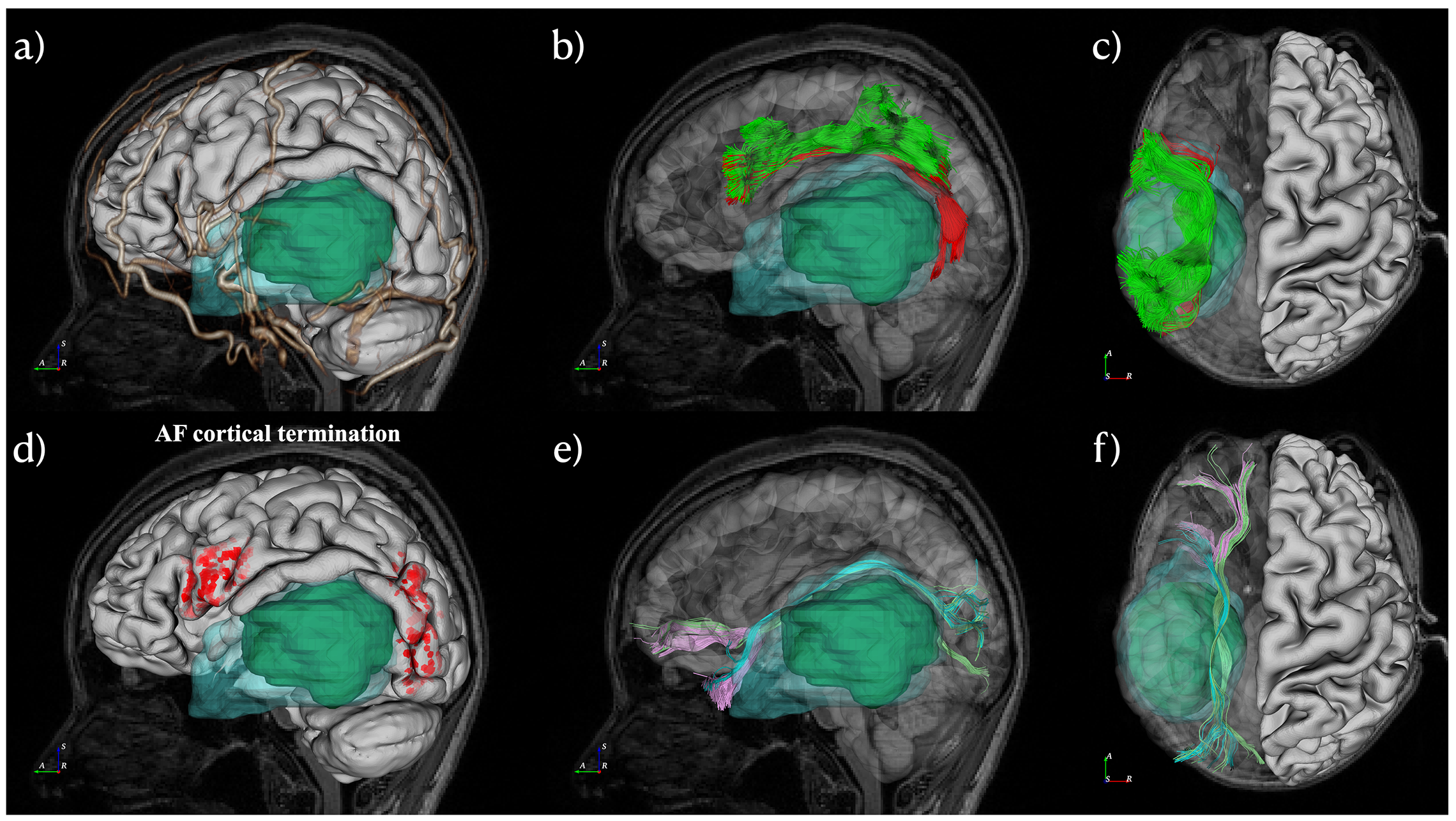
A 41-year-old female with temporal lobe glioblastoma was reconstructed and displayed in DiffusionGo. Cortical surface (white), blood vessel (gold), tumor (green), and peritumoral edema (light blue with translucent) were integrated (a). The lateral view and superior view of the tumor, dorsal language pathway (AF, red; SLF II, green), and ventral language pathway (IFL, light blue; IFOF, light green; UF, pink). The termination projection of AF was shown in d. Superior displacement of left Wernicke’s area was identified with intact AF projecting to left premotor and left Broca areas.