3901
The Usefulness of Variable-density Stack-of-Stars Acquisition in Dynamic Gadolinium-Enhanced MRI of Prostate Cancer: A Preliminary Study1Center for Radiology and Radiation Oncology, Kobe University Hospital, kobe, Japan, 2Department of Radiology, Kobe University Graduate School of Medicine, Kobe University Hospital, kobe, Japan, 3Philips Japan MR Clinical Science, tokyo, Japan
Synopsis
This study aimed to compare the image quality and the quantitative DCE-MRI parameters using the k-space weighted image contrast reconstruction with variable-density golden angle stack-of-stars acquisition (4D-FB) to those of the conventional 3D-T1W turbo field echo sequence (e-THRIVE) in prostate cancer (PCa). Image quality assessment and the receiver operating characteristic curve (AUC) analysis of quantitative DCE-MRI parameters in discrimination PCa from normal tissue were performed. 4D-FB showed significantly higher SNR compared to e-THRIVE. No significant differences were observed in AUCs for each quantitative DCE-MRI parameter. 4D-FB may improve image quality of DCE-MRI with keeping effective pharmacokinetic information in PCa assessment.
Introduction
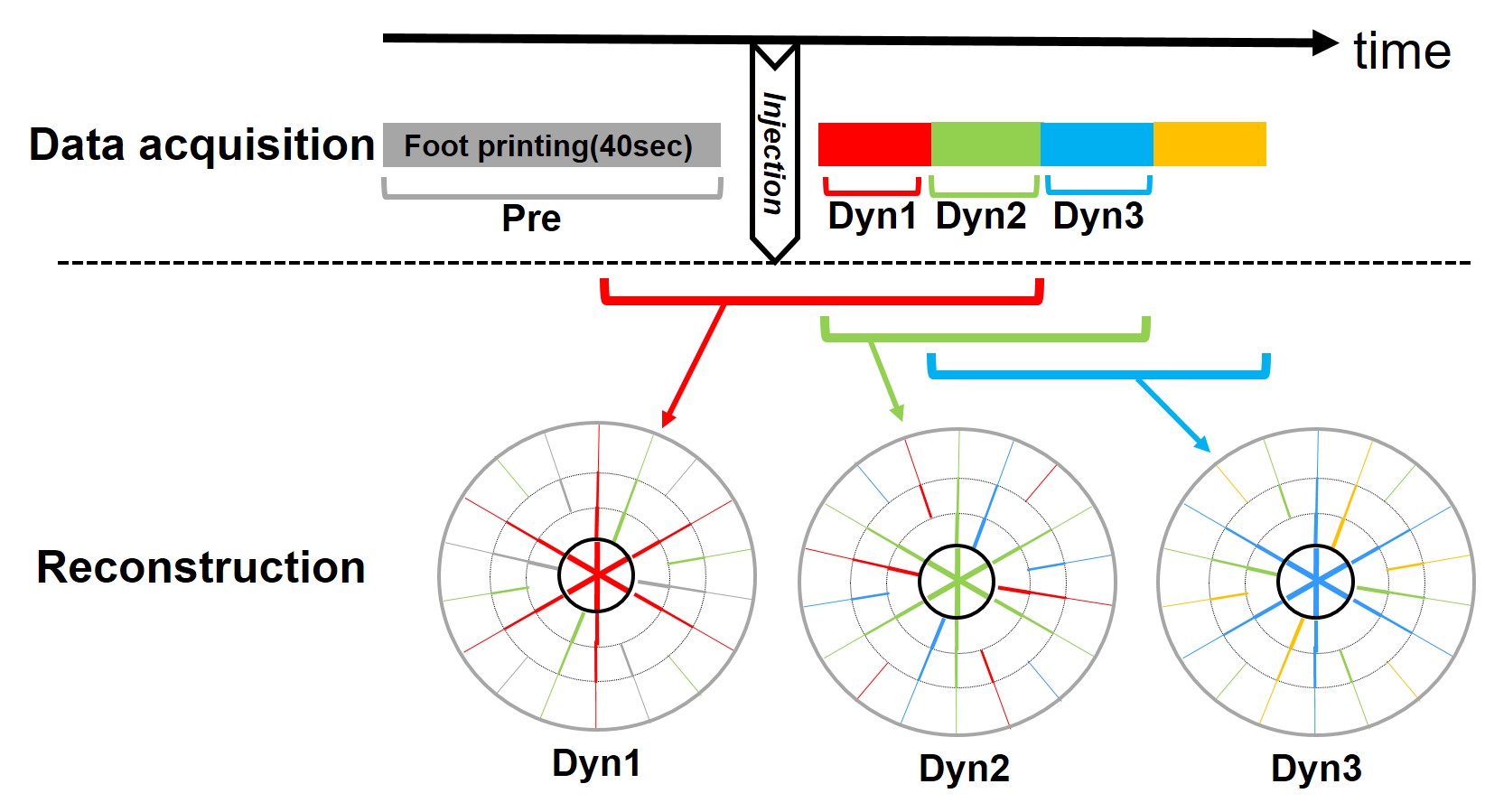
Dynamic contrast-enhanced MRI (DCE-MRI) has become an important component of the multiparametric strategy for evaluation of prostate cancer (PCa). During the past decade, the quantitative analysis of DCE-MRI has gained increasing application in prostate imaging 1,2. The quantitative approach is based on pharmacokinetic modeling techniques, which incorporates contrast media concentration and an arterial input function to calculate time constants for the rate of contrast agent wash-in (Ktrans), wash-out (Kep), and extracellular extravascular volume fraction (Ve). Ideally, the acquisitions for pharmacokinetic analysis should be obtained approximately every 5 seconds to allow the detection of early enhancement 3. As a tradeoff to maintain adequate signal-to-noise ratios (SNR), DCE-MRI for pharmacokinetic analysis is often not as high in resolution as DCE-MRI in routine setting 4. Recently, the k-space weighted image contrast reconstruction using variable-density golden angle stack-of-stars acquisition (4D-FreeBreathing, Philips Medical Systems, Best, The Netherlands) has been employed in many applications since it achieves high SNR with less motion artifacts 5,6. In this technique, the central region of k-space is filled with target phase data, and outside the central region of k-space is continuously filled with other phase data to improve temporal resolution maintaining the SNR. We hypothesized that the 4D-FreeBreathing sequence may obtain DCE-MRI with high spatial and high temporal resolution to fully exploit both the morphologic and kinetic information for PCa. The aim of this study was to compare the image quality and pharmacokinetic parameters of DCE-MRI using 4D-FreeBreathing sequence (4D-FB) to those of the conventional 3D-T1W turbo field echo sequence (e-THRIVE).Materials and Methods
PatientsInstitutional review board approval was obtained for this retrospective study. Twelve patients with biopsy-proven PCa who underwent 3.0T MRI including DCE-MRI with 4D-FB between July 2020 and November 2020 were included in this study. For comparison, the number-, age-, PSA-, and the highest Gleason score(GS)- matched patients who underwent DCE-MRI with e-THRIVE before prostatectomy between January 2017 and December 2019 were also included.
MRI acquisition
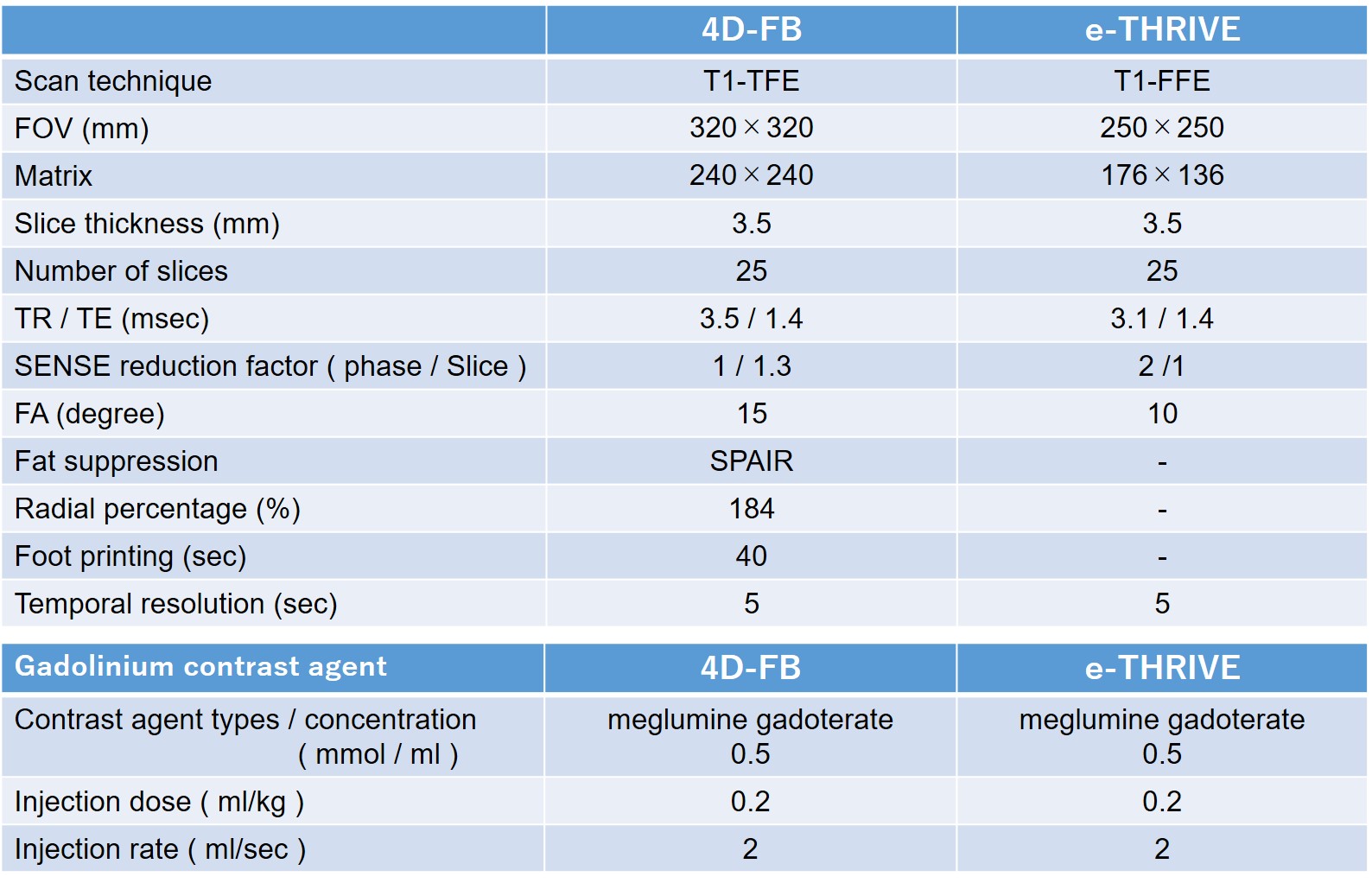
The MR examinations were performed using a 3.0T scanner (Ingenia [for 4D-FB] or Achieva Quasar Dual [for e-THRIVE]; Philips Medical Systems) using a ds-torso coil or 32-element cardiac coil. 4D-FB was continuously scanned during 300 seconds after the initiation of gadolinium contrast agent injection. Foot printing was conducted in 40 seconds, temporal resolution after injection of contrast agent was conducted in 5 seconds, and 60 phase images were consequently acquired in each patient. Summarized sequence parameters for 4D-FB and e-THIRIVE, and schematic diagram for 4D-FB is shown in Figure 1.
Image analysis
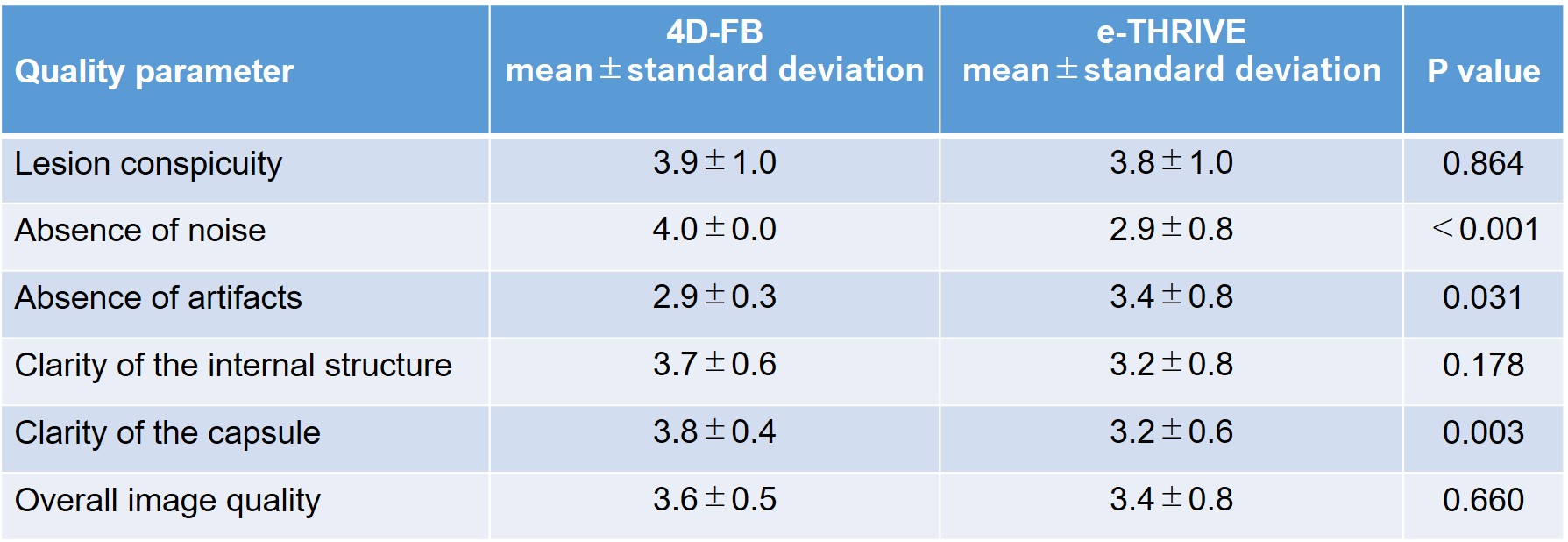
Pharmacokinetic analysis postprocessing software was used to generate colorized parametric maps showing perfusion of enhancing tumors. On the parametric maps, two board-certified radiologists set Regions of interest on the cancerous and non-cancerous lesions with reference to the pathological examinations of MRI-guided biopsy or prostatectomy specimens in consensus. The quantitative DCE-MRI parameters i.e. Ktrans, Kep, and Ve were calculated with the software. For a quantitative image quality assessment, SNRs of PCa, normal prostate tissue, and aorta were measured. As a qualitative image quality assessment, the following items were evaluated with a five-point scale; the lesion conspicuity, absence of noise, absence of artifacts, the clarity of the internal structure of prostate, the clarity of the capsule, and the overall image quality (5=excellent).
Statistical analysis
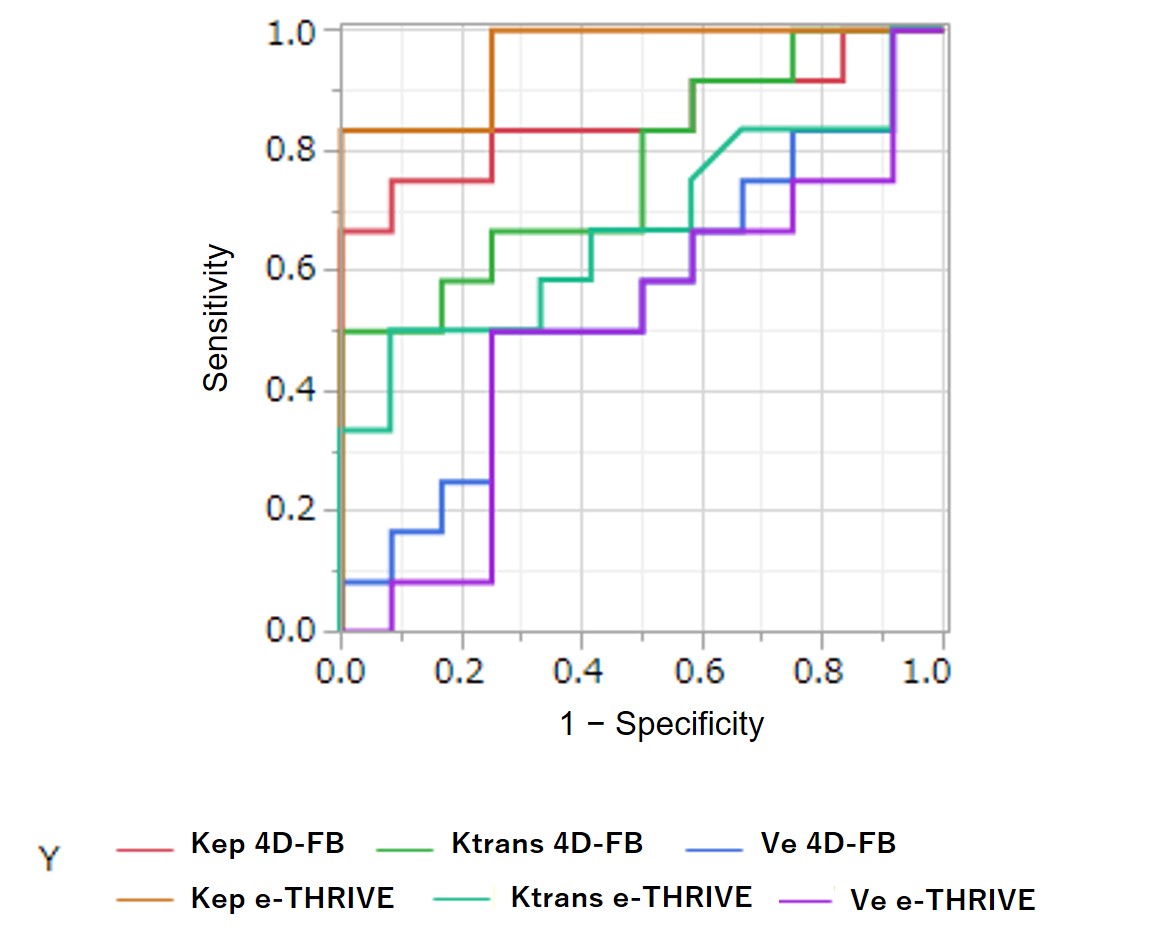
The ability to discriminate PCa from normal tissue of the quantitative DCE-MRI parameters was assessed using areas by the receiver operating characteristic curve (AUC) analysis. AUCs were compared between 4D-FB and e-THRIVE by using the Delong test. The quantitative and qualitative items for image quality assessment were also compared between 4D-FB and e-THRIVE with using Mann–Whitney test.
Results
Twenty-four patients (4D-FB: n=12, e-THRIVE: n=12) were included in this study (age: 68.9±4.94 vs 68.2±4.76 [P>0.05], PSA: 6.73±3.08 vs 8.67±6.20 [P>0.05].) Each number of the highest GS in 4D-FB and in e-THRIVE was as follows; 3+3: n=4, 3+4: n=2, 4+3: n=4, 4+4: n=1, 4+5: n=1. For discrimination PCa from normal tissue, no significant differences were observed in AUCs between 4D-FB and e-THRIVE groups; Ktrans 0.67 vs 0.77(P>0.05), Kep 0.95 vs 0.85(P>0.05), Ve 0.50 vs 0.55(P>0.05) (Figure.2). SNRs of PCa, normal prostate tissue, and aorta of 4D-FB were significantly higher than that of e-THRIVE (14.4±4.4 vs 9.0±1.3, P<0.001, 14.4±3.2 vs 9.4±3.0, P<0.001, 10.4±3.3 vs 8.0±1.9, P=0.03). All qualitative items except for “the absence of artifact” of 4D-FB were higher than those of e-THRIVE (Table 2).Discussion
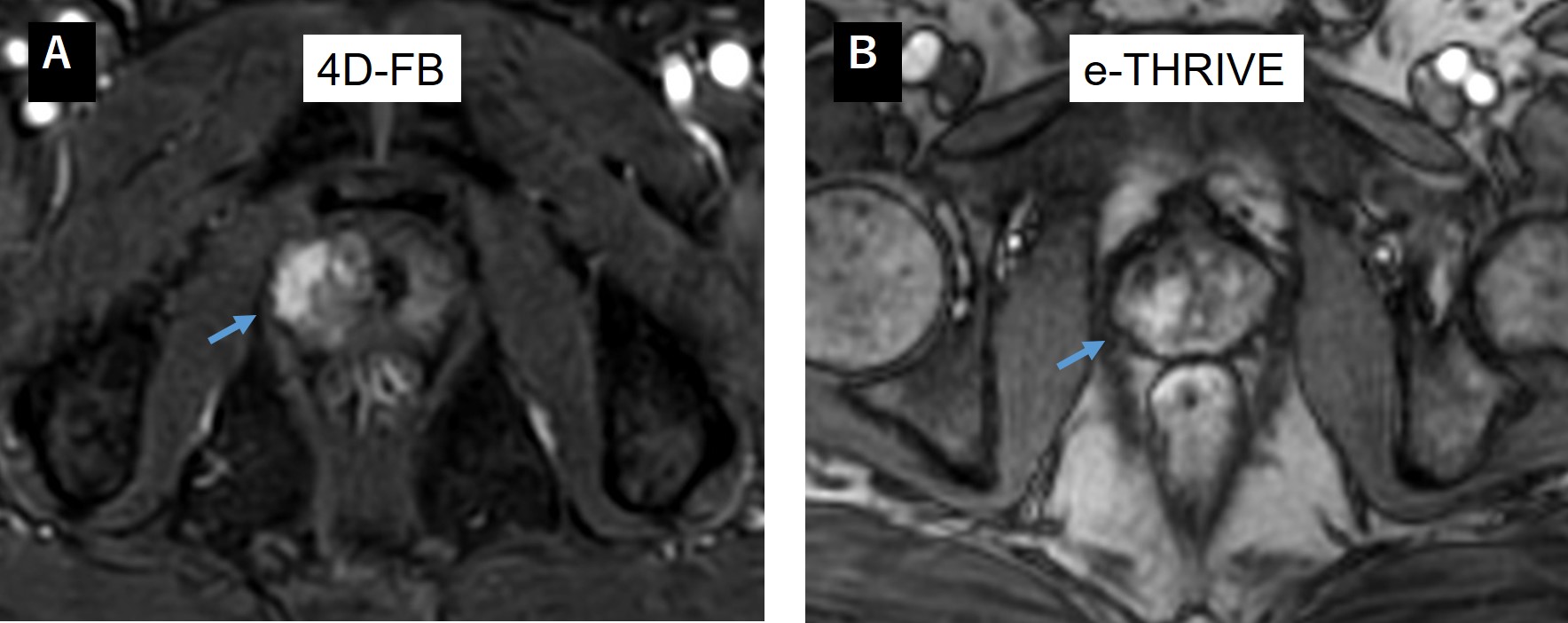
In this study, the ability to discriminate PCa from normal tissue of the quantitative DCE-MRI parameters using 4D-FB was equivalent to that of e-THRIVE. 4D-FB achieved DCE-MRI with high temporal resolution without sacrificing spatial resolution or SNR even under the fat-suppression, leading to the improvement of visual assessment of enhancement (Figure3). However, the artifact caused by radial sampling in 4D-FB should be solved in the future.Conclusion
4D-FB has a potential to improve image quality of high temporal resolution DCE-MRI compared to e-THRIVE, with keeping effective pharmacokinetic information in PCa assessment.Acknowledgements
I would like to thank MRI staffs in Center of Radiology and Radiation Oncology for help with data collection and useful discussions.References
1. Jackson A, Reinsberg S, Sohaib S, et al. Dynamic contrast-enhanced MRI for prostate cancer localization. Br. J. Radiol. 2009 ;82, 148–156 .
2. Vasques, MV, Vasques CRG. Factors that Influence the Permeability Analysis in Magnetic Resonance Studies of the Prostate. Color. Cancer Open Access. 2016;2(3):16 .
3. Verma S, Turkbey B, Muradyan N, et al. Overview of Dynamic Contrast-Enhanced MRI in Prostate Cancer Diagnosis and Management. AIJ. 2012 Jun;198(6) 6072–6078.
4. Turkbey B, Rosenkrantz AB, Haider MA, et al. Prostate Imaging Reporting and Data System Version 2.1: 2019 Update of Prostate Imaging Reporting and Data System Version 2. Eur Urol. 2019 Sep;76(3):340-351.
5. Kim KW, Lee JM, Jeon YS, et al. Free-breathing dynamic contrast-enhanced MRI of the abdomen and chest using a radial gradient echo sequence with K-space weighted image contrast (KWIC). Eur Radiol. 2013 May;23(5):1352-60.
6. Teo QQ, Thng CH, Koh TS, et al Dynamic contrast-enhanced magnetic resonance imaging: applications in oncology. Clin Oncol. 2014 Oct;26(10):e9–e20.
Figures